Page 11 of 22
IM28.{15-19,21-22} | Obstructive Airway Disease Treatment — SDL Guide
Learning Objectives
- Discuss therapies for obstructive airway disease including bronchodilators, leukotriene inhibitors, mast cell stabilisers, theophylline, inhaled and systemic steroids, oxygen, and immunotherapy
- Describe the indications for vaccinations in obstructive airway disease
- Develop a therapeutic plan for stable asthma and COPD using bronchodilators and inhaled corticosteroids following GINA/GOLD step-up frameworks
- Develop a management plan for acute exacerbations including bronchodilators, systemic steroids, and antimicrobial therapy
- Describe the principles and use of oxygen therapy in the hospital and at home
- Demonstrate and counsel patients on the correct use of inhalers
- Communicate diagnosis, treatment plan, and follow-up plan to patients
INSTRUCTIONS
Treatment of obstructive airway disease requires mastery of pharmacology, inhaler devices, step-up and step-down frameworks, and acute exacerbation management — all applied to the individual patient's disease severity, comorbidities, and ability to use devices. This module covers stable disease management, acute exacerbation management, oxygen therapy, inhaler counselling, and patient communication — the full scope of NMC competencies IM28.15–28.22.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 281–282 — Asthma and COPD Management (textbook)
- API Textbook of Medicine, 10th ed. — Treatment of Obstructive Airway Disease (textbook)
- GINA Report: Global Strategy for Asthma Management and Prevention, 2023 (guideline)
- GOLD Report: Global Strategy for Diagnosis, Management and Prevention of COPD, 2023 (guideline)
- BTS/SIGN British Guideline on the Management of Asthma, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients leave your outpatient clinic on the same afternoon. The first is a 28-year-old asthmatic woman who has had three nocturnal awakenings this week and is using her salbutamol inhaler six times a day. You step up her therapy from low-dose ICS to ICS/LABA combination. She has never been shown how to use a dry-powder inhaler — so the medication, however correctly chosen, will not reach her airways. The second is a 64-year-old COPD patient who has had two exacerbations requiring hospitalisation this year. You add a LAMA to his LABA, discuss flu vaccination, and give him an action plan for self-management — but you forget to ask about his smoking status. He is still smoking a pack a day. The lesson: pharmacological excellence is necessary but not sufficient. Treatment of obstructive airway disease requires the right drug, the right device, the right technique, and the right non-pharmacological framework — delivered to a patient who understands their diagnosis and has a personalised plan.
WHY THIS MATTERS
Treatment of obstructive airway disease is one of the highest-yield clinical competencies in the NMC final-year curriculum — it spans pharmacology, device skills, communication, and emergency management. In India, asthma and COPD together affect approximately 55–60 million people; yet surveys consistently show that 70–80% of patients use inhalers incorrectly, adherence to maintenance therapy is poor, and under-treatment is the norm in both primary and secondary care. As a final-year graduate you will immediately begin managing these patients — in the outpatient clinic, on the ward, and in the emergency department. Competencies IM28.15–28.22 require you to prescribe correctly, counsel on devices, manage exacerbations, explain oxygen therapy, and communicate with patients in a way that builds adherence and partnership.
RECALL
Recall the key drug classes before proceeding. Beta₂-agonists act on airway smooth muscle β₂-adrenoceptors, activating adenyl cyclase, raising cAMP, activating protein kinase A, and relaxing smooth muscle — bronchodilation. Short-acting (SABA, e.g., salbutamol, duration 4–6 hours) vs long-acting (LABA, e.g., salmeterol, formoterol, duration 12 hours). Anticholinergics (muscarinic antagonists) block M3 receptors on airway smooth muscle and mucus glands, reducing bronchoconstriction and mucus hypersecretion. Short-acting (SAMA, e.g., ipratropium, 6–8 hours) vs long-acting (LAMA, e.g., tiotropium, 24 hours). Corticosteroids suppress airway inflammation — inhaled (ICS, e.g., budesonide, fluticasone) act locally with minimal systemic effects; oral/IV (prednisolone, hydrocortisone) act systemically. Leukotriene receptor antagonists (LTRA) (e.g., montelukast) block CysLT1 receptors, reducing bronchoconstriction, oedema, and mucus secretion driven by cysteinyl leukotrienes. Theophylline is a non-selective phosphodiesterase inhibitor — prevents cAMP breakdown, causing bronchodilation; also has anti-inflammatory and respiratory muscle stimulant effects; narrow therapeutic window.
Pharmacology of OAD Therapies: Mechanisms and Drugs
Understanding the pharmacological basis of obstructive airway disease treatment allows rational drug selection, recognition of drug interactions and side effects, and adaptation of therapy to individual patient needs. The treatments used in asthma and COPD overlap substantially but differ in emphasis — COPD management centres on long-acting bronchodilators and exacerbation prevention, while asthma management centres on inhaled corticosteroids and step-up of anti-inflammatory therapy.
Provided image
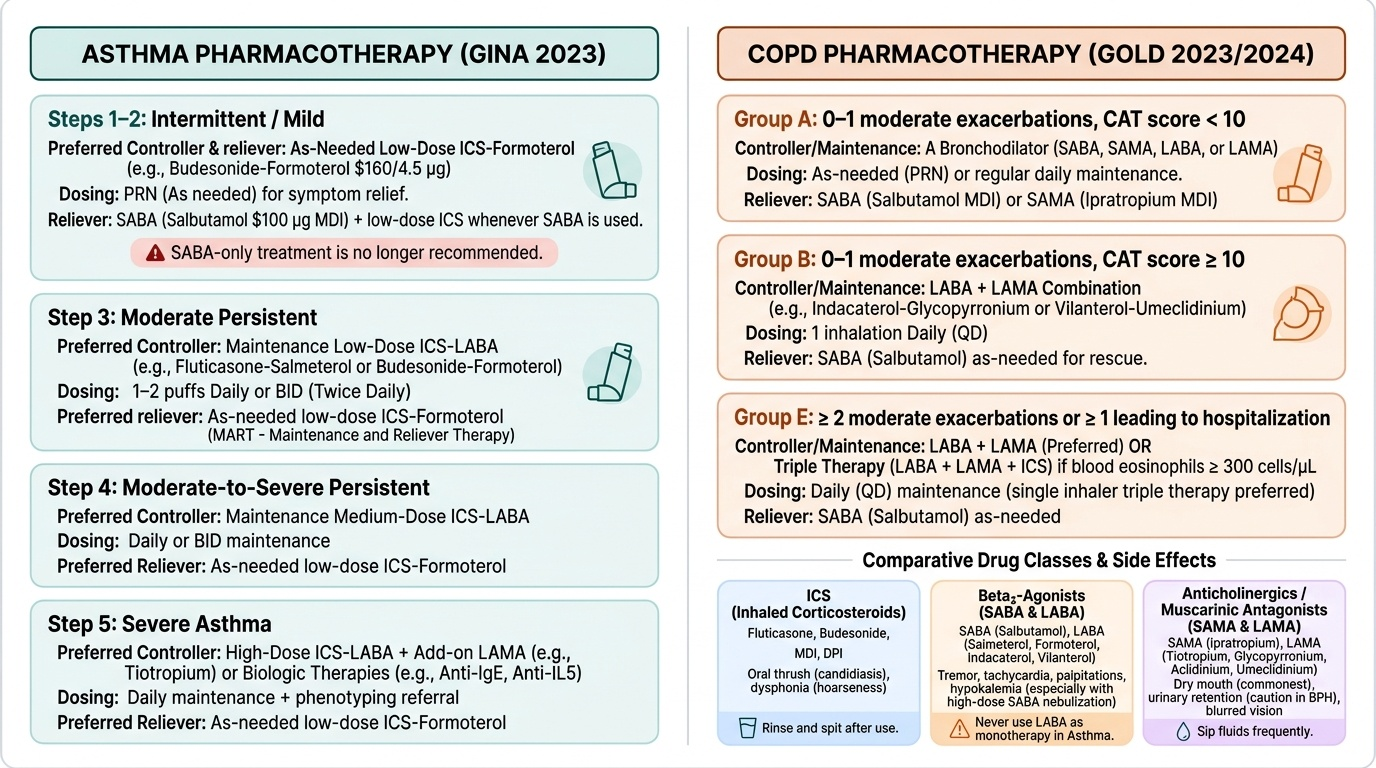
Bronchodilators — Beta₂-agonists:
Salbutamol (albuterol) is the prototype SABA — onset within 5 minutes, peak at 30 minutes, duration 4–6 hours. It is the reliever of choice for acute bronchospasm in both asthma and COPD exacerbations. In asthma, GINA 2023 has moved away from SABA-only as a reliever, preferring ICS-formoterol (low-dose) as the preferred reliever for Step 1–2 asthma — because each symptomatic episode is also an inflammatory event, and ICS-containing reliever ensures anti-inflammatory coverage at every use. In COPD, SABA is used as a rescue medication alongside maintenance LABA/LAMA. Side effects of beta₂-agonists: tremor, tachycardia, palpitations, hypokalaemia (particularly with high-dose nebulisation or IV salbutamol — monitor serum potassium in acute severe asthma), and paradoxical bronchospasm (rare, with some formulations).
LABAs (salmeterol, formoterol, indacaterol, vilanterol): 12–24 hour duration; never used as monotherapy in asthma (risk of masking worsening inflammation without addressing it — associated with increased asthma deaths in older studies; always combined with ICS in asthma). In COPD, LABAs can be used as monotherapy or in combination with LAMA.
Anticholinergics (muscarinic antagonists):
Ipratropium bromide (SAMA): onset 15–30 minutes, duration 6–8 hours; particularly effective in COPD (where cholinergic tone is a more prominent contributor to obstruction than in asthma); used in combination with SABA in acute COPD exacerbations (salbutamol + ipratropium nebulisation is the first-line bronchodilator therapy). Tiotropium (LAMA, 24-hour): the pivotal UPLIFT trial demonstrated significant reduction in exacerbation frequency and hospitalisations in COPD. Other LAMAs: glycopyrronium, aclidinium, umeclidinium. Side effects: dry mouth (commonest), urinary retention (caution in BPH), blurred vision (angle-closure glaucoma — never nebulise without mouthpiece), constipation.
Inhaled Corticosteroids (ICS):
ICS are the cornerstone of asthma management — they reduce airway eosinophilic inflammation, decrease airway hyperresponsiveness, reduce exacerbation frequency, and improve quality of life. They do NOT significantly alter the rate of lung function decline in COPD (unlike in asthma), but reduce exacerbation frequency when added to LABA in patients with frequent exacerbations and elevated blood eosinophils. Drugs: budesonide, fluticasone propionate, beclomethasone dipropionate, mometasone. Side effects: oral candidiasis (advise rinsing mouth and gargling after each use), dysphonia (hoarseness from laryngeal deposition), paradoxical bronchospasm. Systemic effects are minimal at standard doses but increase with high-dose ICS (adrenal suppression, reduced bone density, cataracts with long-term use).
Leukotriene Receptor Antagonists (LTRA):
Montelukast (5–10 mg daily, oral) blocks CysLT1 receptors. Indications: add-on therapy in mild-moderate asthma not controlled on low-dose ICS; particularly useful in exercise-induced asthma, aspirin-exacerbated respiratory disease (AERD), and asthma with allergic rhinitis (montelukast addresses both). Less effective than ICS as monotherapy; used as an add-on or ICS-sparing agent. Also approved in children from age 6 months. Note: FDA 2020 black box warning — neuropsychiatric events (behaviour changes, depression, suicidality) reported; prescribe with caution and counsel patients/parents.
Mast Cell Stabilisers:
Sodium cromoglicate and nedocromil sodium prevent mast cell degranulation, reducing both the early and late-phase asthmatic response. They are inhaled, non-steroidal, and very safe. However, they are less effective than ICS and require four-times-daily dosing — their use has declined substantially. Residual role: exercise-induced asthma (pre-exercise use) in patients who cannot use ICS, and paediatric allergic asthma.
Theophylline:
Theophylline is a methylxanthine bronchodilator with a narrow therapeutic window (therapeutic serum level 10–20 mcg/mL; toxic above 20 mcg/mL). Benefits: bronchodilation, improved mucociliary clearance, respiratory muscle strengthening, weak anti-inflammatory effect. Significant drug interactions: erythromycin, ciprofloxacin, cimetidine, and oral contraceptives INCREASE theophylline levels (risk of toxicity); rifampicin, phenytoin, and smoking DECREASE levels. Toxicity: nausea, vomiting, arrhythmias (AF, VT), seizures. In the modern era, theophylline is a third-line add-on in COPD (useful when LABA/LAMA are insufficient or unavailable) and a rescue add-on in severe asthma. It has no role as first-line therapy.
Immunotherapy (allergen-specific immunotherapy, ASIT):
AIT involves repeated administration of increasing doses of the sensitising allergen (subcutaneous or sublingual route) to induce immunological tolerance. Indications: IgE-mediated allergic asthma with a clearly identified single dominant allergen (house dust mite, grass pollen) that is not adequately controlled with pharmacotherapy. Contraindications: severe/unstable asthma (FEV1 <70% predicted), use of beta-blockers. Requires specialised allergy centre; 3–5 year course; risk of anaphylaxis (subcutaneous route requires supervised injection and 30-minute observation period with adrenaline available).
Biological therapies (advanced OAD — for awareness):
For severe refractory asthma not controlled with high-dose ICS/LABA ± add-ons: anti-IgE (omalizumab — for IgE-mediated asthma with elevated total IgE); anti-IL-5/anti-IL-5Rα (mepolizumab, benralizumab — for eosinophilic asthma with persistent elevated blood eosinophils); anti-IL-4Rα (dupilumab — for type-2 asthma and concurrent eosinophilic sinusitis with nasal polyps). These are Step 5 add-on therapies.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
Pharmacological Classes in Asthma and COPD
Stable Disease Management: GINA and GOLD Step-up Frameworks
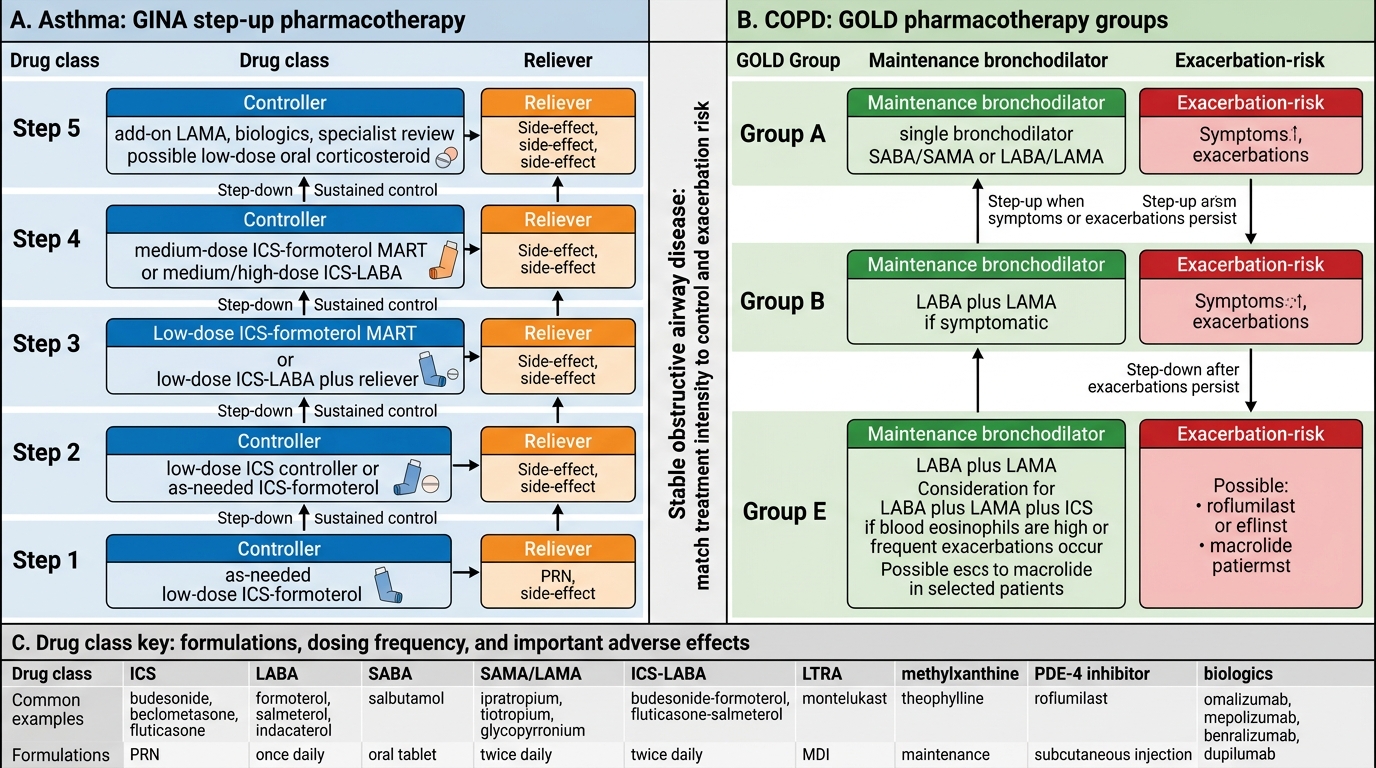
The treatment of stable obstructive airway disease follows evidence-based step-up frameworks — the GINA steps for asthma and the GOLD algorithm for COPD. The key principle in both is that treatment intensity is matched to disease severity and control level, adjusted by regular review, and escalated when control is inadequate and de-escalated when sustained control has been achieved.
Provided image
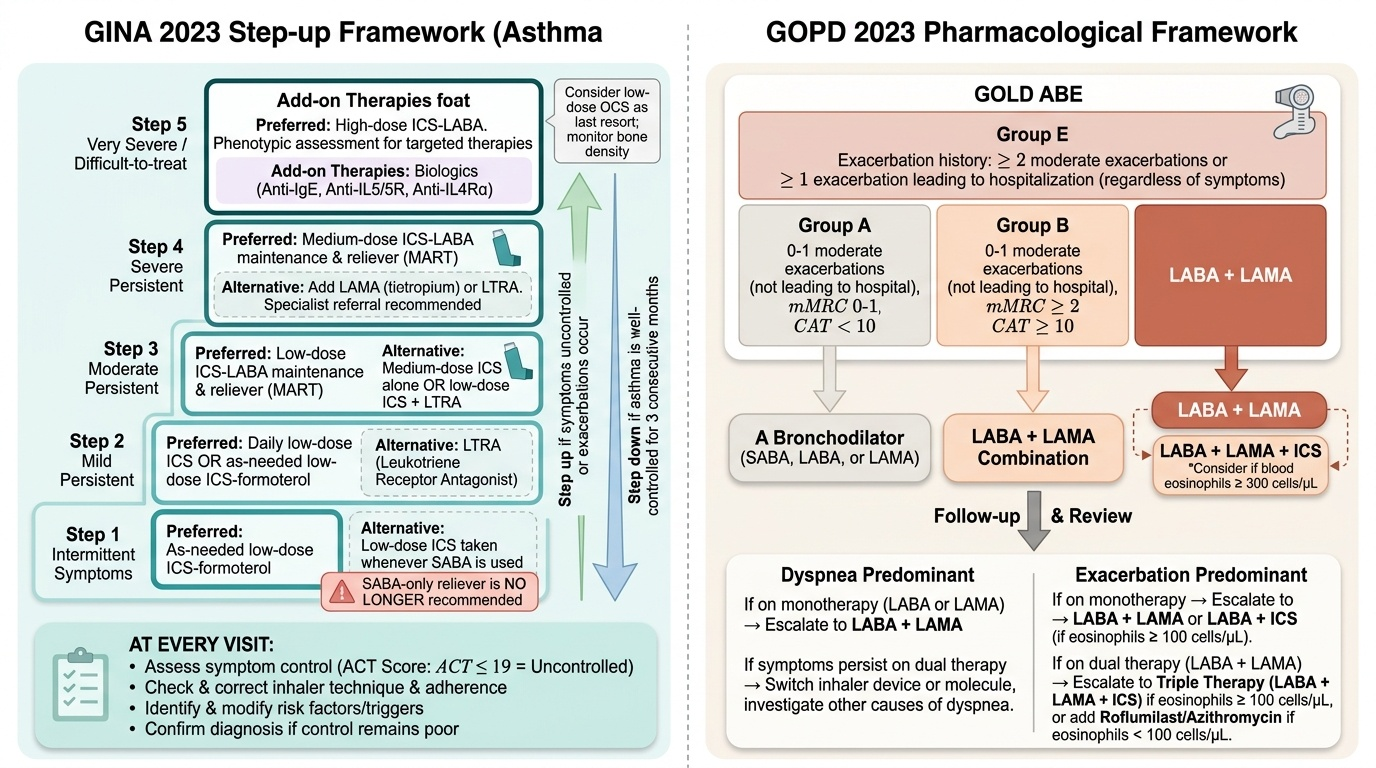
GINA Step-up Framework for Asthma (2023):
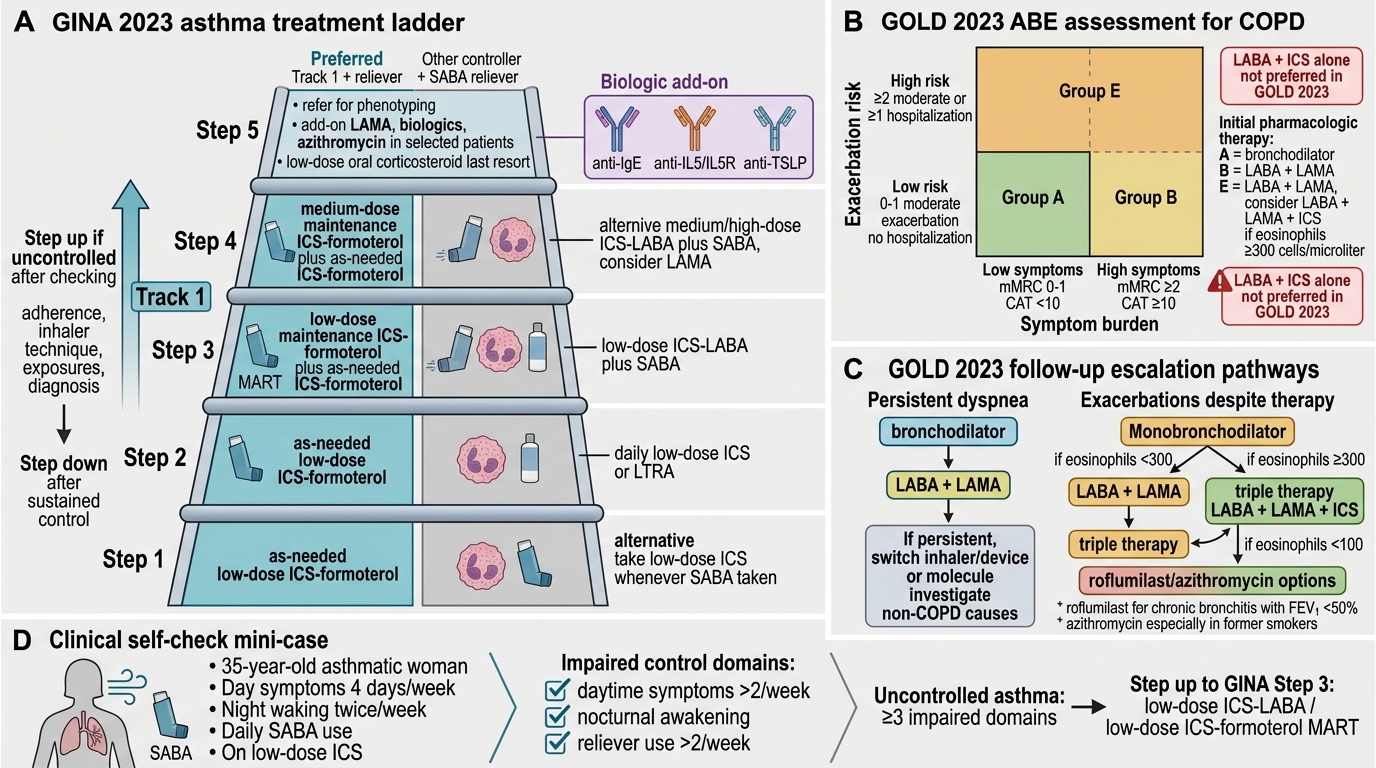
GINA 2023 has made a paradigm shift: SABA-only reliever therapy is no longer recommended at any step for adults and adolescents. The preferred reliever is now low-dose ICS-formoterol (used as both controller and reliever — the MART approach: Maintenance And Reliever Therapy). This approach ensures that every symptomatic episode is accompanied by anti-inflammatory ICS dosing, reducing the risk of severe exacerbations from under-treated inflammation masked by SABA relief. The five GINA steps:
- Step 1 (intermittent symptoms): As-needed low-dose ICS-formoterol (preferred) OR low-dose ICS taken whenever SABA is used (alternative). SABAs alone are NO LONGER the preferred first step.
- Step 2 (mild persistent): Low-dose ICS as daily controller + as-needed SABA or low-dose ICS-formoterol as reliever; add LTRA as an alternative controller.
- Step 3 (moderate persistent): Low-dose ICS/LABA combination (preferred); OR medium-dose ICS alone. Plus LTRA add-on if inadequate.
- Step 4 (severe persistent): Medium-to-high dose ICS/LABA; consider add tiotropium, LTRA, or theophylline. Refer to specialist.
- Step 5 (very severe/difficult to treat): High-dose ICS/LABA; evaluate and treat treatable traits; add-on anti-IgE, anti-IL-5, or anti-IL-4Rα biologics per eligibility; low-dose oral corticosteroids as last resort (minimum effective dose; monitor bone density).
At every visit: assess symptom control (Asthma Control Test score — ACT ≤19 = uncontrolled); check and correct inhaler technique; assess adherence; review triggers; confirm the diagnosis is correct if control is poor.
GOLD Pharmacological Framework for Stable COPD (2023):
GOLD 2023 uses the ABE classification (Group A = low symptoms/low exacerbation risk; Group B = high symptoms/low risk; Group E = exacerbation risk regardless of symptoms) alongside spirometric GOLD grade to guide initial therapy:
- Group A (low symptoms, ≤1 moderate exacerbation): A bronchodilator (SABA or LAMA as needed)
- Group B (high symptoms, ≤1 moderate exacerbation): LAMA + LABA combination preferred (better than either alone for dyspnoea and exercise tolerance)
- Group E (≥2 moderate or ≥1 hospitalised exacerbation): LAMA + LABA as initial therapy; if blood eosinophils ≥300 cells/mcL OR if on LAMA+LABA with ongoing exacerbations: escalate to LAMA + LABA + ICS (triple therapy)
Additional COPD management essentials:
- Smoking cessation — the single most important intervention; refer to cessation clinic; offer pharmacotherapy (varenicline first-line, bupropion, NRT patches/gum)
- Pulmonary rehabilitation — supervised exercise training plus education; improves dyspnoea, exercise capacity, and quality of life in all GOLD grades; reduces exacerbation-related hospitalisations
- Long-term oxygen therapy (LTOT) — ≥15 hours/day; indications: resting PaO₂ ≤55 mmHg, or PaO₂ 56–60 mmHg with cor pulmonale or haematocrit >55%; proven survival benefit
- Non-invasive ventilation (NIV) — for chronic nocturnal hypercapnia (PaCO₂ >52 mmHg during stable state) reduces hospitalisation risk
- Vaccinations — annual influenza (all COPD patients); pneumococcal vaccine (PCV13 + PPSV23 per schedule); COVID-19 vaccination
- Nutrition — low BMI in COPD is a poor prognostic marker; nutritional supplementation in underweight patients
GINA 2023 Asthma Ladder vs GOLD 2023 COPD Pharmacotherapy
SELF-CHECK
A 35-year-old asthmatic woman has daytime symptoms 4 days per week, wakes twice per week with wheeze, and uses her SABA inhaler daily. She is currently on low-dose ICS alone. According to GINA, what is her asthma control level, and what is the appropriate next step?
A. Well-controlled — continue current therapy and review in 3 months
B. Partly controlled — add LTRA and reassess in 3 months
C. Uncontrolled — step up to low-dose ICS/LABA combination (GINA Step 3)
D. Severe asthma — refer immediately to a specialist for biologic therapy
Reveal Answer
Answer: C. Uncontrolled — step up to low-dose ICS/LABA combination (GINA Step 3)
GINA classifies asthma control based on the past 4 weeks: well-controlled = daytime symptoms ≤2 days/week, no nocturnal awakening, SABA use ≤2 days/week, no activity limitation. This patient has daytime symptoms >2 days/week, nocturnal awakenings, and daily SABA use — all three control domains are impaired. This is UNCONTROLLED asthma (≥3 impaired domains = uncontrolled). She is at GINA Step 2 (low-dose ICS alone) and uncontrolled, so the appropriate step is to step up to Step 3: low-dose ICS/LABA combination. LTRA alone would be an alternative Step 2 option, not a Step 3 escalation. Biologic referral is reserved for Step 5.
Acute Exacerbation Management
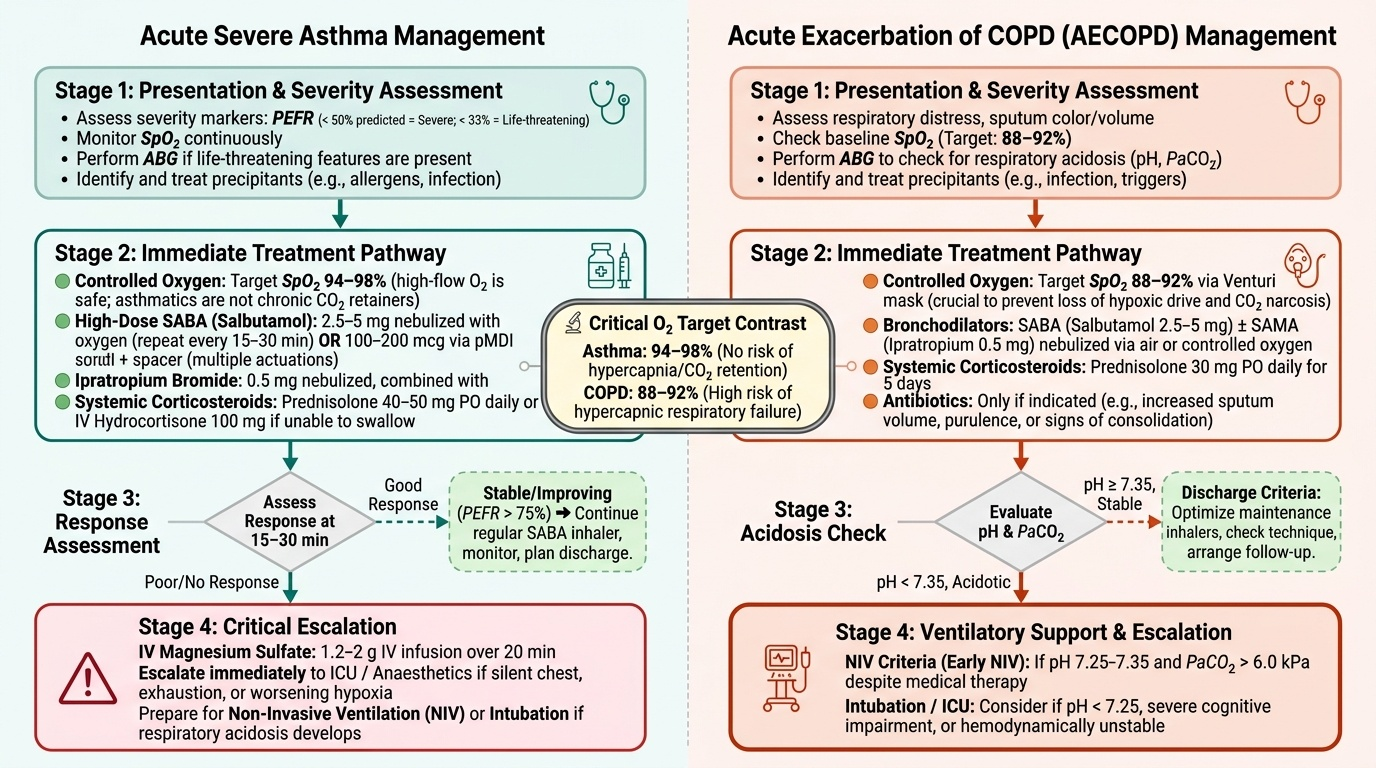
Acute exacerbations of obstructive airway disease represent time-sensitive clinical emergencies in which the speed and completeness of treatment directly determines outcome. The critical difference between a well-managed and a poorly-managed acute exacerbation is not merely the choice of drug but the sequence of actions, the oxygen target used, and the decisiveness with which ventilatory support is escalated. Delayed steroid administration prolongs hospital stay; wrong oxygen targets cause CO₂ narcosis in COPD; failure to start NIV early in a patient with pH 7.30 leads to avoidable intubation. The management framework differs between asthma and COPD exacerbations but shares key elements: bronchodilation, anti-inflammatory treatment, controlled oxygenation, identification and treatment of the precipitant, and escalation to ventilatory support when needed.
Provided image
Acute Severe Asthma — Emergency Management:
All patients with severe or life-threatening acute asthma require hospital management. The immediate treatment sequence:
- Controlled oxygen: target SpO₂ 94–98% (note: this is different from COPD — in asthma, high-flow oxygen does NOT cause CO₂ retention because asthmatics are not chronic CO₂ retainers; the standard safe target of 94–98% applies)
- High-dose SABA (salbutamol): 2.5–5 mg nebulised with oxygen, repeated every 15–30 minutes (back-to-back nebulisations in life-threatening asthma); OR salbutamol 100–200 mcg via pMDI + spacer (multiple actuations) — equally effective as nebulisation for moderate attacks and faster to administer
- Ipratropium 0.5 mg nebulised with salbutamol: addition of ipratropium to salbutamol significantly improves FEV1 and reduces hospital admission rate in moderate-severe asthma
- Systemic corticosteroids: prednisolone 40 mg orally (or IV hydrocortisone 100 mg QID if unable to swallow) — start within 1 hour; continue for 5 days (no need for taper after a short course). Mechanism: suppress eosinophilic airway inflammation; peak clinical effect takes 4–6 hours
- ABG in severe or life-threatening attacks (SpO₂ <92% or not responding to treatment)
- Magnesium sulphate IV (2 g over 20 minutes) — for life-threatening asthma or severe asthma not responding to initial bronchodilator therapy; relaxes smooth muscle by blocking calcium channels; NNT approximately 10
- IV salbutamol or IV aminophylline — in patients who cannot inhale (unconscious, intubated, or very severe obstruction preventing effective inhalation); aminophylline requires a loading dose (if not already on theophylline) followed by infusion with serum level monitoring
- NIV — limited role in acute asthma (contrasted with COPD where NIV is first-line for hypercapnic exacerbation); may be considered as a bridge to intubation in selected cases
- Invasive mechanical ventilation — if impending respiratory arrest, deteriorating consciousness, or PaCO₂ rising despite maximal medical therapy; use pressure-controlled ventilation with permissive hypercapnia strategy (avoid high pressures — auto-PEEP and barotrauma risk in hyperinflated lungs)
Response assessment: PEFR measured at 15–30 minutes after bronchodilators. PEFR rising to >75% personal best and sustained = can consider discharge with step-up of maintenance therapy, written action plan, and follow-up within 48 hours.
Acute Exacerbation of COPD (AECOPD) — Hospital Management:
AECOPD is defined as an acute worsening of respiratory symptoms requiring a change in treatment. Management priorities:
- Controlled oxygen: target SpO₂ 88–92% (not 94–98%) — the Venturi mask (24% or 28%) is the device of choice to deliver precise FiO₂ in known or suspected CO₂ retainers. High-flow O₂ risks CO₂ narcosis
- Bronchodilators (short-acting): nebulised salbutamol 2.5–5 mg + ipratropium 0.5 mg combined — given 4–6 hourly; titrate to response
- Systemic corticosteroids: prednisolone 30–40 mg orally × 5 days (GOLD 2023 recommendation; longer courses add side effects without benefit); reduces treatment failure, shortens hospital stay, and reduces early relapse rate
- Antibiotics: prescribed when Anthonisen type-1 criteria are met (all three: increased dyspnoea + increased sputum volume + purulent sputum) OR if patient requires mechanical ventilation. First choice: co-amoxiclav (amoxicillin-clavulanate) or doxycycline or azithromycin. In severe COPD (GOLD 3–4) or prior Pseudomonas isolation: ciprofloxacin. Duration: 5–7 days
- NIV (BiPAP): first-line treatment for acute hypercapnic respiratory failure in AECOPD — indicated when pH < 7.35 and PaCO₂ elevated despite controlled oxygen and bronchodilators. Reduces intubation rate, ICU mortality, and hospital length of stay. Contraindications to NIV: reduced consciousness, inability to protect airway, vomiting, facial trauma, haemodynamic instability, respiratory arrest
- Invasive mechanical ventilation: when NIV fails or is contraindicated
- Theophylline IV (aminophylline): use only if insufficient response to inhaled bronchodilators; monitor serum levels; requires dose adjustment for cardiac failure, liver disease, elderly patients, and drug interactions
- DVT prophylaxis: LMWH (enoxaparin) — hospitalised COPD patients have elevated DVT risk; prophylaxis reduces PE mortality
Discharge criteria from AECOPD hospitalisation: SpO₂ stable on usual O₂ therapy; stable on q4h or less frequent bronchodilators; patient able to walk safely; eating and sleeping well; able to self-manage with an action plan.
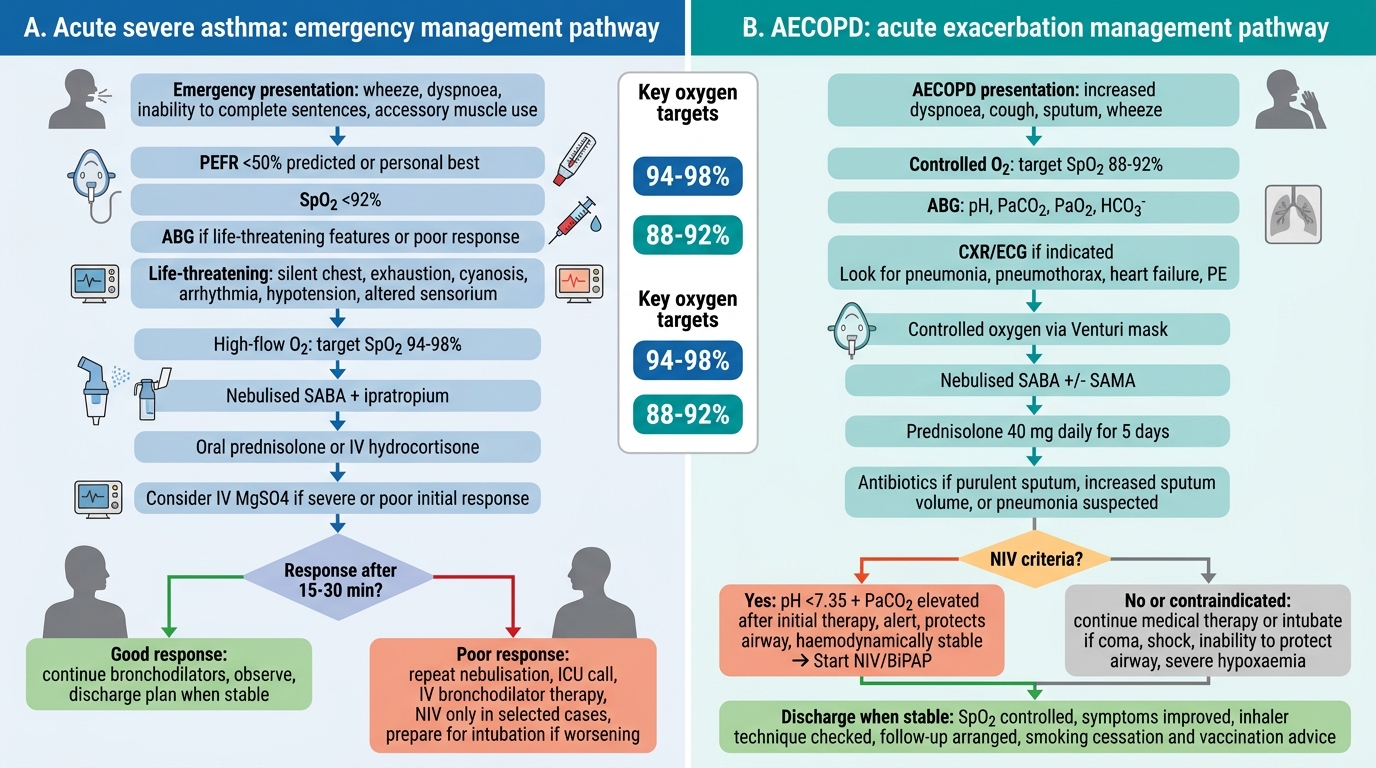
Emergency Management of Acute Asthma and AECOPD
SELF-CHECK
A 67-year-old COPD patient is admitted with acute exacerbation. ABG: pH 7.30, PaCO₂ 72 mmHg, PaO₂ 52 mmHg, HCO₃⁻ 34 mEq/L. After 2 hours of controlled oxygen (SpO₂ 88–92%) and nebulised bronchodilators, his pH is 7.31 and PaCO₂ is 75 mmHg. His GCS is 14, he can protect his airway, and he is not haemodynamically unstable. What is the most appropriate next intervention?
A. Increase oxygen flow rate to target SpO₂ 94–98% to improve PaO₂
B. Initiate NIV (BiPAP) — pH <7.35 with elevated PaCO₂ and clinical stability meet NIV criteria
C. Immediate intubation and invasive mechanical ventilation
D. Repeat bronchodilators and reassess in 2 hours before escalating
Reveal Answer
Answer: B. Initiate NIV (BiPAP) — pH <7.35 with elevated PaCO₂ and clinical stability meet NIV criteria
This patient has persistent acute-on-chronic hypercapnic respiratory failure (pH <7.35, elevated PaCO₂) not responding adequately to 2 hours of first-line therapy. He is alert (GCS 14), can protect his airway, and is haemodynamically stable — all prerequisites for NIV trial. GOLD and BTS guidelines recommend NIV (BiPAP) as the first-line treatment for AECOPD-related hypercapnic respiratory failure when pH <7.35 and PaCO₂ is elevated. NIV significantly reduces the need for intubation and mortality. Increasing oxygen would worsen CO₂ retention. Invasive ventilation is appropriate only if NIV fails or is contraindicated. Waiting 2 more hours without escalation in a patient with pH 7.30 is inappropriate.