Page 12 of 22
IM28.{15-19,21-22} | Obstructive Airway Disease Treatment — SDL Guide (Part 2)
Oxygen Therapy: Hospital and Home Principles
Oxygen is the most commonly used drug in hospitalised respiratory patients, and like any drug it has both indications and contraindications, correct and incorrect dosing, and potential for harm if used without understanding the underlying physiology. A clear understanding of oxygen therapy principles is therefore essential — this is competency IM28.19. The fundamental error in clinical practice is treating oxygen as universally beneficial and harmless. In patients without CO₂ retention — asthmatics, pneumonia, pulmonary embolism — high-flow oxygen is appropriate and life-saving when hypoxaemia is severe. In patients with COPD and chronic CO₂ retention, however, the same high-flow oxygen can suppress the residual hypoxic ventilatory drive, worsen alveolar hypoventilation, raise PaCO₂ further, and cause CO₂ narcosis. The Venturi mask was designed specifically to solve this problem — delivering a precise, fixed FiO₂ regardless of how hard or how slowly the patient is breathing. Mastery of oxygen therapy requires knowing the target SpO₂, the delivery device, and the physiological mechanism behind each choice.
Indications for supplemental oxygen:
- Acute hypoxaemia: SpO₂ <94% in most patients; SpO₂ <88% in known CO₂ retainers
- Post-operative patients, acute MI (if hypoxaemic), septic shock, carbon monoxide poisoning (high-flow 100% O₂ regardless of SpO₂)
- Target SpO₂ 94–98% in most patients; 88–92% in COPD with known or suspected chronic CO₂ retention
Oxygen delivery devices in hospital:
| Device | FiO₂ Range | Notes |
|---|---|---|
| Nasal cannula (1–6 L/min) | 24–44% | Imprecise; patient-breath-dependent; comfortable for low flow |
| Simple face mask (5–10 L/min) | 35–55% | Imprecise; risk of CO₂ rebreathing below 5 L/min |
| Venturi mask | 24%, 28%, 35%, 40%, 60% (colour-coded valves) | Precise FiO₂ regardless of patient's flow or effort — device of choice for COPD exacerbation with CO₂ retention; venturi principle entrains room air in a fixed ratio |
| Non-rebreather mask (15 L/min) | 60–90% | For severe acute hypoxaemia (not CO₂ retainers); used in anaphylaxis, trauma, severe pneumonia |
| High-flow nasal cannula (HFNC) | Up to 100% | Heated humidified; high flow reduces anatomical dead-space; useful in type-1 respiratory failure; limited evidence in acute COPD |
Pathophysiology of oxygen toxicity in COPD:
As covered in the Foundations module, chronic CO₂ retainers with compensated respiratory acidosis (elevated HCO₃⁻) rely on the peripheral hypoxic drive (carotid body stimulation by low PaO₂) as their dominant ventilatory stimulus. Raising PaO₂ rapidly with uncontrolled oxygen abolishes this drive, reduces ventilatory effort, and causes progressive CO₂ retention — CO₂ narcosis (drowsiness, confusion, asterixis, coma) and respiratory arrest. The Venturi mask, delivering a precise fixed FiO₂, allows controlled oxygenation targeting SpO₂ 88–92% without over-oxygenating.
Long-term oxygen therapy (LTOT) at home:
LTOT is prescribed for COPD patients with severe resting chronic hypoxaemia. The two landmark trials (MRC 1981, NOTT 1980) established that LTOT for ≥15 hours/day prolongs survival — the only intervention in COPD that has this proven survival benefit apart from smoking cessation. Criteria for LTOT:
- PaO₂ ≤55 mmHg on room air during stable state (two measurements ≥3 weeks apart)
- PaO₂ 56–60 mmHg if accompanied by cor pulmonale (elevated JVP, peripheral oedema), pulmonary hypertension, or polycythaemia (haematocrit >55%)
- Note: SpO₂ ≤88% on room air is a surrogate threshold used in practice but ABG confirmation is preferred for formal LTOT assessment
- LTOT is NOT indicated in patients who continue to smoke (fire risk; no survival benefit demonstrated in active smokers; does not help rehabilitation)
- Device: concentrator (extracts O₂ from room air) preferred for home use — cheaper running cost than cylinders for ≥15 hours use
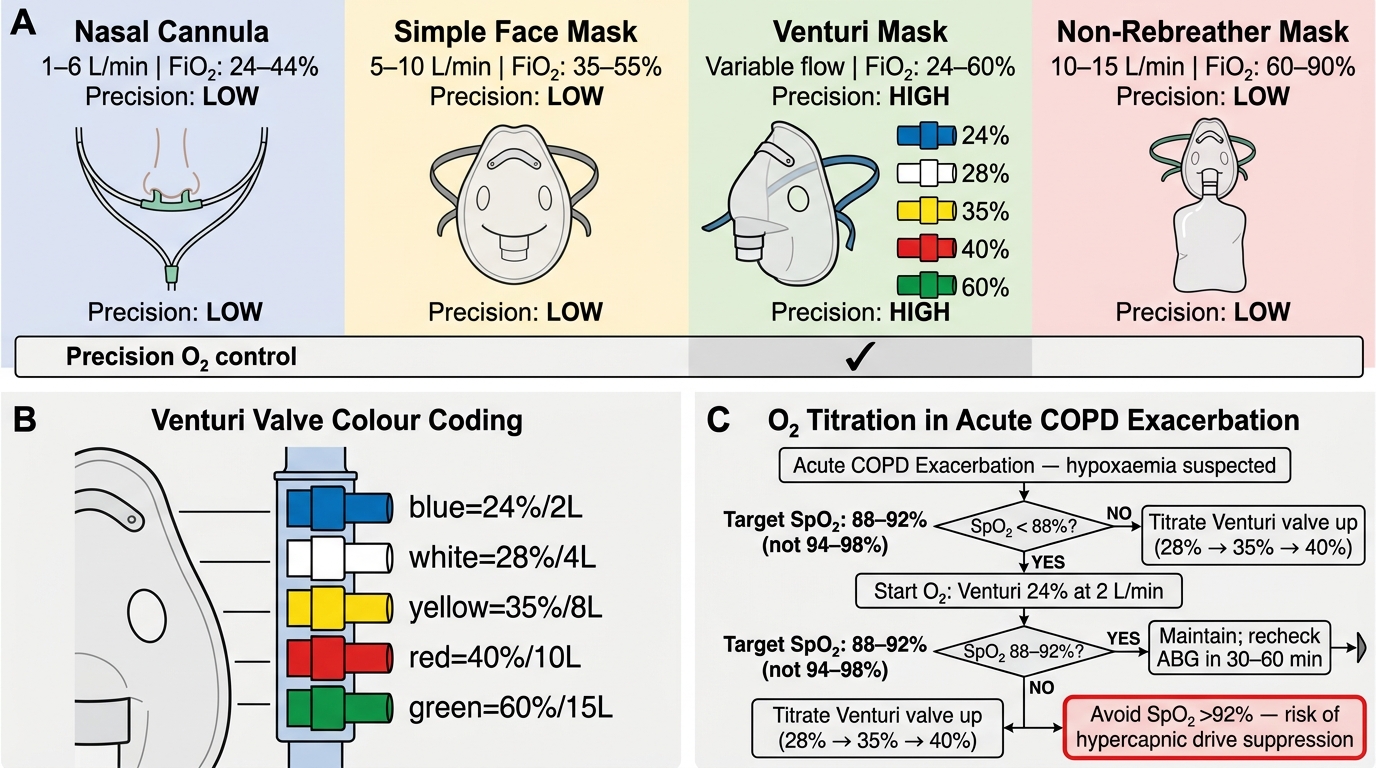
Oxygen Delivery Devices and Titration in Acute COPD
Inhaler Devices: Counselling and Technique
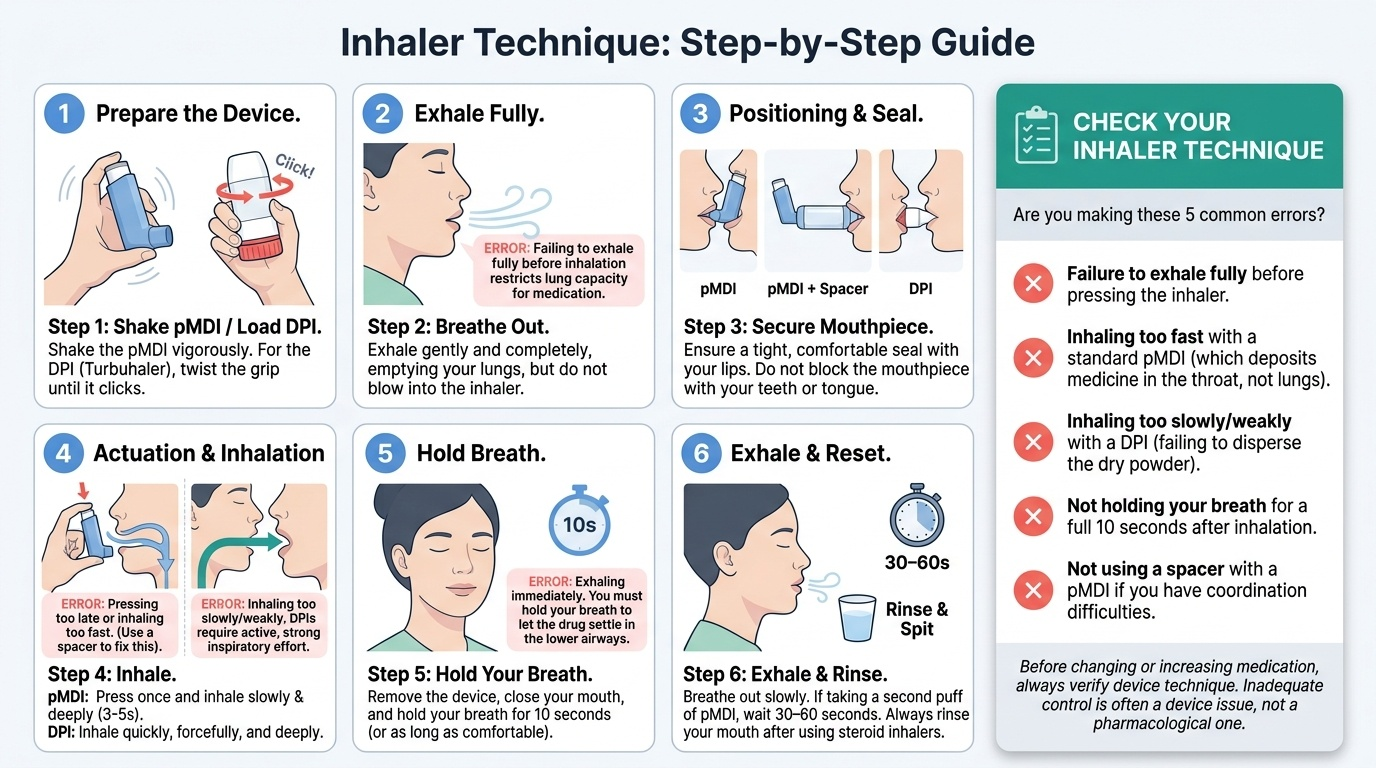
Inhaler therapy is the cornerstone of both asthma and COPD management, but its benefit is entirely dependent on correct technique and consistent use. Surveys in India and globally consistently show that more than 70% of patients use inhalers incorrectly — the most common errors being failure to exhale fully before actuation, inhaling too fast with a pMDI, inhaling too slowly with a DPI, not holding the breath after inhalation, and not using a spacer with a pMDI. The therapeutic consequence is stark: a patient taking a correctly prescribed ICS/LABA combination inhaler with poor technique receives a fraction of the labelled dose to the lower airways, meaning a pharmacologically optimal prescription delivers subtherapeutic clinical results. Before adding or changing a drug, always check and correct the existing inhaler technique — inadequate control may be a device problem, not a pharmacological inadequacy. Competency IM28.21 requires you to DEMONSTRATE the correct technique and counsel patients effectively — not just describe it.
Provided image
Types of inhaler devices:
1. Pressurised metered-dose inhaler (pMDI): the most widely used device; a canister in a plastic actuator delivers a metered dose on pressing; requires coordination between pressing and inhaling (the 'press-and-breathe' technique); the most common source of technique error. A spacer (large-volume spacer device) eliminates the coordination requirement by acting as a reservoir — especially important for children, elderly patients, and anyone who struggles with coordination. All pMDI prescriptions should include spacer counselling.
- Technique: shake well; exhale fully; seal lips around mouthpiece or spacer; press canister once; inhale slowly and deeply over 3–5 seconds; hold breath for 10 seconds; exhale slowly; wait 30–60 seconds between doses.
2. Dry-powder inhaler (DPI): no propellant — drug is released as a powder by the patient's inspiratory effort; therefore requires adequate inspiratory flow (≥30–60 L/min depending on device type — Turbuhaler requires 30 L/min, Accuhaler/Diskus requires 30 L/min, Handihaler 20 L/min minimum). Problem: in acute severe asthma or COPD exacerbation, inspiratory flow may be inadequate to draw sufficient drug from the DPI — pMDI + spacer is preferred in acute settings. Each DPI type has specific technique (Turbuhaler: twist and click; Diskus: slide and click; Handihaler: pierce and inhale) — always demonstrate and check.
3. Soft-mist inhaler (SMI, Respimat): generates a slow-moving mist; lower impaction than pMDI; less coordination-dependent; useful in elderly patients. Requires loading and twisting to prime.
4. Nebulisers: liquid drug converted to aerosol by compressed air or ultrasound; used in acute exacerbations (can be driven by oxygen — important in asthma; use air nebuliser in COPD to avoid O₂ over-delivery); also used for patients unable to use pMDI or DPI. Less portable than inhalers.
Universal technique errors to correct:
- Not shaking the pMDI canister before use
- Inhaling too fast (pMDI) — should be slow and deep (3–5 seconds)
- Not holding breath for 10 seconds after inhalation
- Using the DPI in acute attack when inspiratory flow is inadequate
- Not cleaning the device — blocked actuator reduces dose delivery
- Continuing to use an empty inhaler (dose counter not checked)
Patient counselling on inhalers:
Effective counselling requires a structured approach: (1) demonstrate the correct technique yourself using a placebo device; (2) ask the patient to demonstrate it back to you ('teach-back'); (3) identify and correct specific errors; (4) provide a written instruction leaflet in the patient's language; (5) re-check technique at every review visit. Studies show that device education at a single visit reduces incorrect technique by 50%, but technique degrades over weeks without reinforcement — technique checking at every visit is a standard of care, not an optional extra.
Key counselling messages for asthma patients:
- Take the ICS preventer inhaler every day, even when symptom-free — it is treating inflammation, not just symptoms
- Use the reliever (salbutamol or ICS-formoterol) only when needed — increasing reliever use is a signal that the preventer is not controlling the disease adequately
- Rinse mouth after ICS use to prevent oral candidiasis
- Bring all inhalers to every appointment — check technique and adherence
Key counselling messages for COPD patients:
- Your inhalers reduce breathlessness and prevent exacerbations — they do not cure COPD
- Smoking cessation is the single most important step you can take to slow the progression of your disease
- Use the LAMA/LABA inhalers every day at the same time; they are maintenance devices, not rescue devices
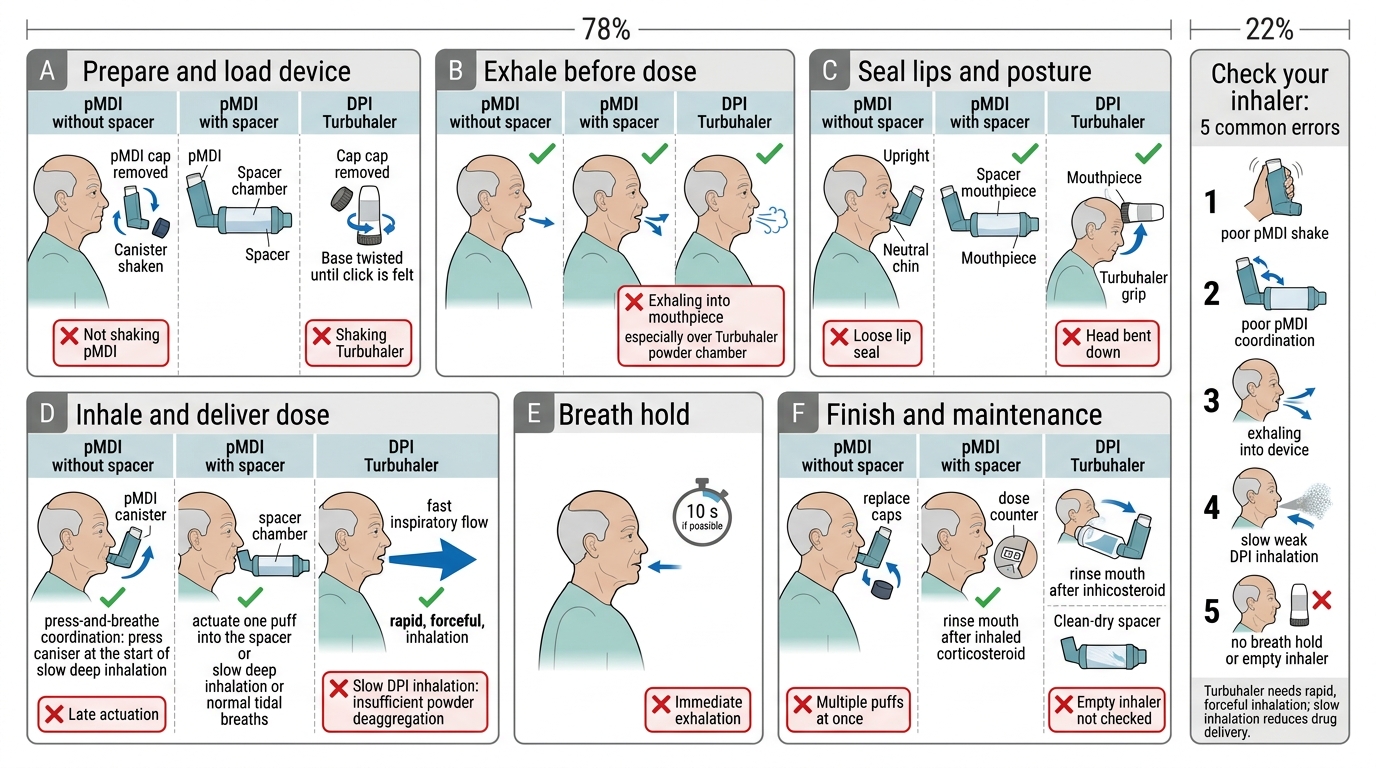
Correct Inhaler Technique and Common Errors
SELF-CHECK
During an outpatient COPD review, a 68-year-old man demonstrates his Turbuhaler technique. You observe him: (1) loading the device correctly, (2) exhaling fully, (3) placing the mouthpiece in his mouth but inhaling very slowly over 8 seconds. What is the critical error, and what is the consequence?
A. No error — a slow deep breath maximises drug deposition in the lower airways
B. Exhaling before actuation is incorrect — he should inhale immediately after loading
C. Turbuhaler requires a rapid, forceful inspiratory effort — slow inhalation provides insufficient flow to deaggregrate the powder particles and deliver the drug
D. He should shake the Turbuhaler before use — without shaking, the powder clumps
Reveal Answer
Answer: C. Turbuhaler requires a rapid, forceful inspiratory effort — slow inhalation provides insufficient flow to deaggregrate the powder particles and deliver the drug
DPI devices including the Turbuhaler require a sufficiently fast and forceful inspiratory effort (minimum ~30 L/min for Turbuhaler) to create the turbulent airflow needed to deaggregate and carry the fine powder particles into the lower airways. A slow inhalation at 8 seconds fails to generate this flow, resulting in insufficient drug delivery — the drug remains in the device or deposits in the oropharynx rather than reaching the small airways. This is the most consequential inhaler technique error for DPI users. Unlike pMDI (where slow inhalation is correct), DPI requires an inspiratory effort that is fast and deep — not a gentle tidal breath. Turbuhaler does not need shaking (unlike pMDI).
Vaccinations and Patient Communication
Two competencies that are often under-taught deserve specific attention in the management of OAD: the role of vaccinations in preventing infective exacerbations (IM28.16), and the communication skills required to convey the diagnosis, treatment plan, and follow-up to patients in a way that builds understanding, adherence, and self-efficacy (IM28.22). Both competencies sit at the intersection of clinical knowledge and professional behaviour — they require not just knowing what to do, but doing it well with every patient. Studies show that communication failures account for a significant proportion of medication non-adherence in chronic respiratory disease: patients who leave the clinic without clearly understanding which inhaler is the preventer (taken daily) versus the reliever (taken as needed) will reverse the two, taking the SABA daily and reaching for the ICS only when breathless. Similarly, the evidence that vaccinations prevent infective exacerbations is strong, yet vaccination rates in COPD patients in India remain well below targets. Both of these translate directly to preventable hospitalisations.
Vaccinations in OAD (IM28.16):
Infective exacerbations are the leading cause of OAD-related hospitalisations and mortality. Vaccination is a proven, cost-effective preventive strategy:
- Influenza vaccine (annual): indicated for ALL patients with asthma and COPD; reduces influenza-related exacerbations and hospitalisations by approximately 40–50%. The inactivated vaccine is preferred (live attenuated nasal spray is contraindicated in severe asthma). Optimal timing in India: October–November before the winter respiratory season.
- Pneumococcal vaccine: PCV13 (conjugate, one lifetime dose) + PPSV23 (polysaccharide, repeated at 5-year intervals for high-risk patients); indicated for COPD and severe asthma. Reduces the incidence of community-acquired pneumonia, a major COPD exacerbation trigger. GOLD guidelines recommend pneumococcal vaccination in all COPD patients.
- COVID-19 vaccination: COPD and severe asthma are high-risk conditions for severe COVID-19; vaccination is strongly recommended and reduces hospitalisation and mortality risk.
- Bordetella pertussis (Tdap): a booster dose is recommended for adults with COPD who have not received a recent Tdap, as pertussis can cause severe prolonged cough exacerbations.
- Zoster vaccine (herpes zoster / shingles): recommended for COPD patients ≥50 years, particularly those on systemic corticosteroids (which increase zoster risk).
Communicating diagnosis, treatment plan, and follow-up (IM28.22):
Effective patient communication is a clinical competency — not a social courtesy. Studies consistently show that patients who understand their diagnosis, know why they are taking each medication, and have a written action plan have fewer exacerbations, better adherence, and lower emergency visits.
Key elements of a complete communication encounter for an OAD patient:
- Diagnosis explanation: use plain language — 'You have COPD, which is a long-term lung condition caused by years of smoking. It means your airways are narrowed and do not open fully, making breathing harder. It cannot be cured, but we can slow it down and treat the symptoms.'
- Smoking cessation counselling (for COPD): 'The single most important thing you can do is to stop smoking. It will not reverse the damage already done, but it will slow down further loss of lung function. I would like to refer you to our smoking cessation programme.'
- Medication explanation: for each inhaler — what it is for (preventer vs reliever), when to use it, how to use it (demonstrate + teach-back), potential side effects to watch for (rinsing after ICS, dry mouth from anticholinergics).
- Asthma/COPD action plan: a written personalised plan in the patient's language that specifies: (a) what 'green zone' (stable, continue current therapy) looks like for them; (b) 'yellow zone' (worsening — increase reliever, start prednisolone, see doctor within 48 hours); (c) 'red zone' (emergency — call ambulance, use reliever continuously, go to A&E).
- Follow-up appointment: specify date and what will be reviewed (PEFR, inhaler technique, control questionnaire, spirometry if needed).
- Empathy and address concerns: 'Many patients worry about becoming dependent on inhalers — can I address that for you?' 'Are there any practical difficulties with taking the inhalers — cost, storage, using them at work?'
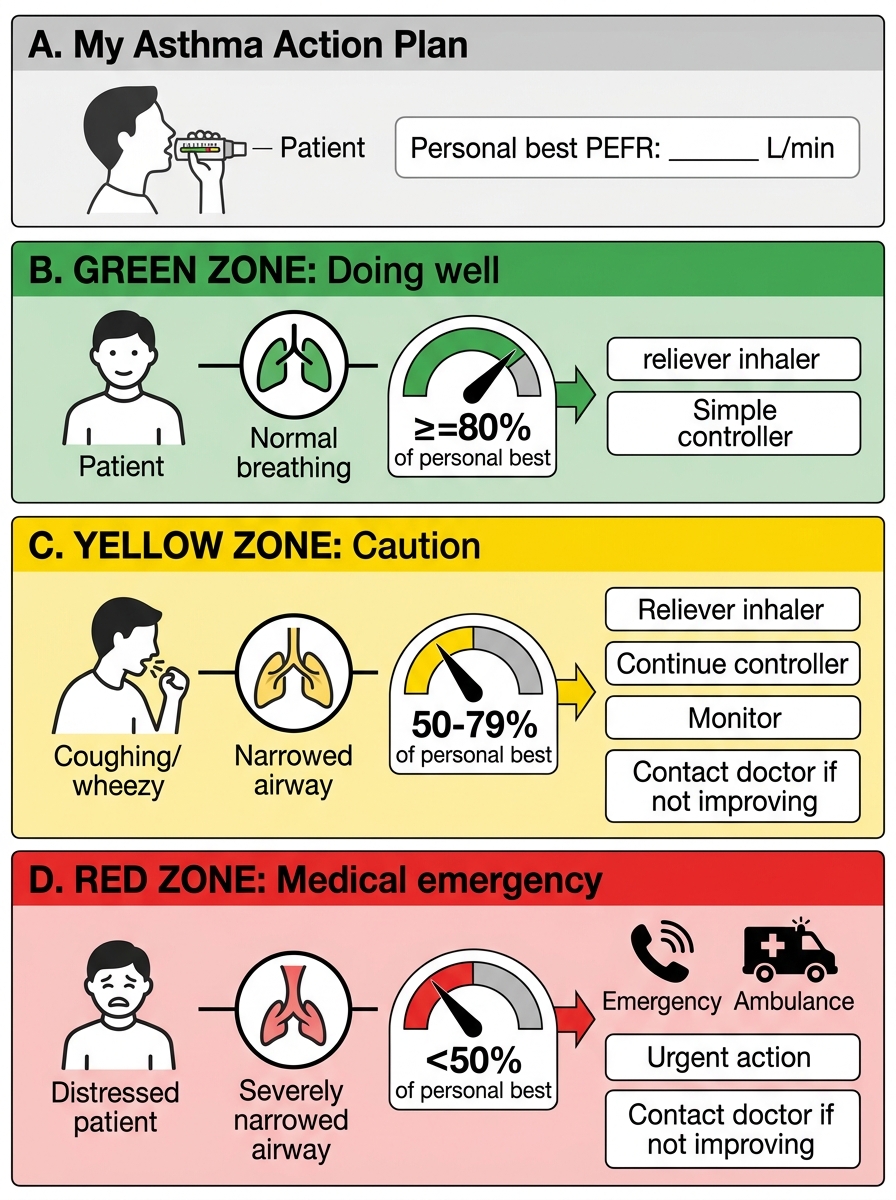
Patient-Friendly Three-Zone Asthma Action Plan
CLINICAL PEARL
Three treatment pearls for OAD: First, LABA monotherapy is contraindicated as sole therapy in asthma — LABAs must always be combined with ICS in asthma because LABA-only therapy masks worsening inflammation and has been associated with increased asthma deaths. Never prescribe a LABA inhaler without ICS for an asthmatic patient. Second, NIV is first-line, not a last resort, in AECOPD with pH <7.35 and elevated PaCO₂ — NIV reduces intubation rates, ICU mortality, and hospital stay; early initiation (not waiting until the patient is near-arrest) produces the best outcomes. Third, systemic corticosteroids in AECOPD should be for exactly 5 days — the REDUCE trial showed no benefit beyond 5 days; prolonged courses add steroid side effects without therapeutic gain.
Self-Assessment: Treatment Decision Scenarios
Apply the treatment principles from this module to the following clinical scenarios. For each, identify the correct management approach and its rationale.
Provided image
Scenario A: A 30-year-old asthmatic teacher has been on low-dose ICS (budesonide 200 mcg BD) for 12 months. She reports symptom control is good — no nocturnal wakening, uses her SABA inhaler once weekly at most. Her ACT score is 22 (well-controlled). She asks whether she can reduce her inhaler. What is your recommendation?
Analysis: Well-controlled asthma on low-dose ICS for at least 3 months = candidate for GINA step-down. Reduce the ICS dose by 50% (to budesonide 100 mcg BD) and review in 3 months. Stopping ICS entirely risks relapse. At the reduced dose, if she remains well-controlled for a further 3 months, consider stepping down to as-needed ICS-formoterol. Always check inhaler technique before attributing control to the medication.
Scenario B: A 72-year-old man with GOLD 3 COPD (FEV1 38% predicted) on LAMA+LABA combination has had 3 moderate exacerbations requiring antibiotics in the past year. His blood eosinophil count is 420 cells/mcL. What should be added to his therapy, and why?
Analysis: Frequent exacerbations (≥2 moderate or ≥1 severe) despite LAMA+LABA, with blood eosinophils ≥300 cells/mcL — both criteria for adding ICS are met. Step up to triple therapy (LAMA + LABA + ICS). GOLD recommends ICS addition in patients with ≥2 moderate exacerbations or ≥1 leading to hospitalisation, and the eosinophil count ≥300 cells/mcL is the key biomarker predicting ICS response in COPD. A single-inhaler triple therapy (e.g., fluticasone/umeclidinium/vilanterol or budesonide/glycopyrronium/formoterol) improves adherence.
Scenario C: A 45-year-old woman with AERD (aspirin-exacerbated respiratory disease, Samter's triad) has poorly controlled asthma on medium-dose ICS/LABA. She has nasal polyps causing persistent rhinorrhoea and nasal obstruction. What add-on therapy is most appropriate?
Analysis: AERD with nasal polyps and poorly controlled asthma on ICS/LABA = montelukast (LTRA add-on) is specifically beneficial. The mechanism of AERD is excess leukotriene production from COX-1 inhibition; leukotriene receptor antagonism with montelukast targets the pathogenic mechanism directly. Additionally, dupilumab (anti-IL-4Rα biologic) is now approved for uncontrolled moderate-severe asthma with type-2 inflammation AND for chronic rhinosinusitis with nasal polyps — it addresses both problems simultaneously. NSAID avoidance counselling is also essential.
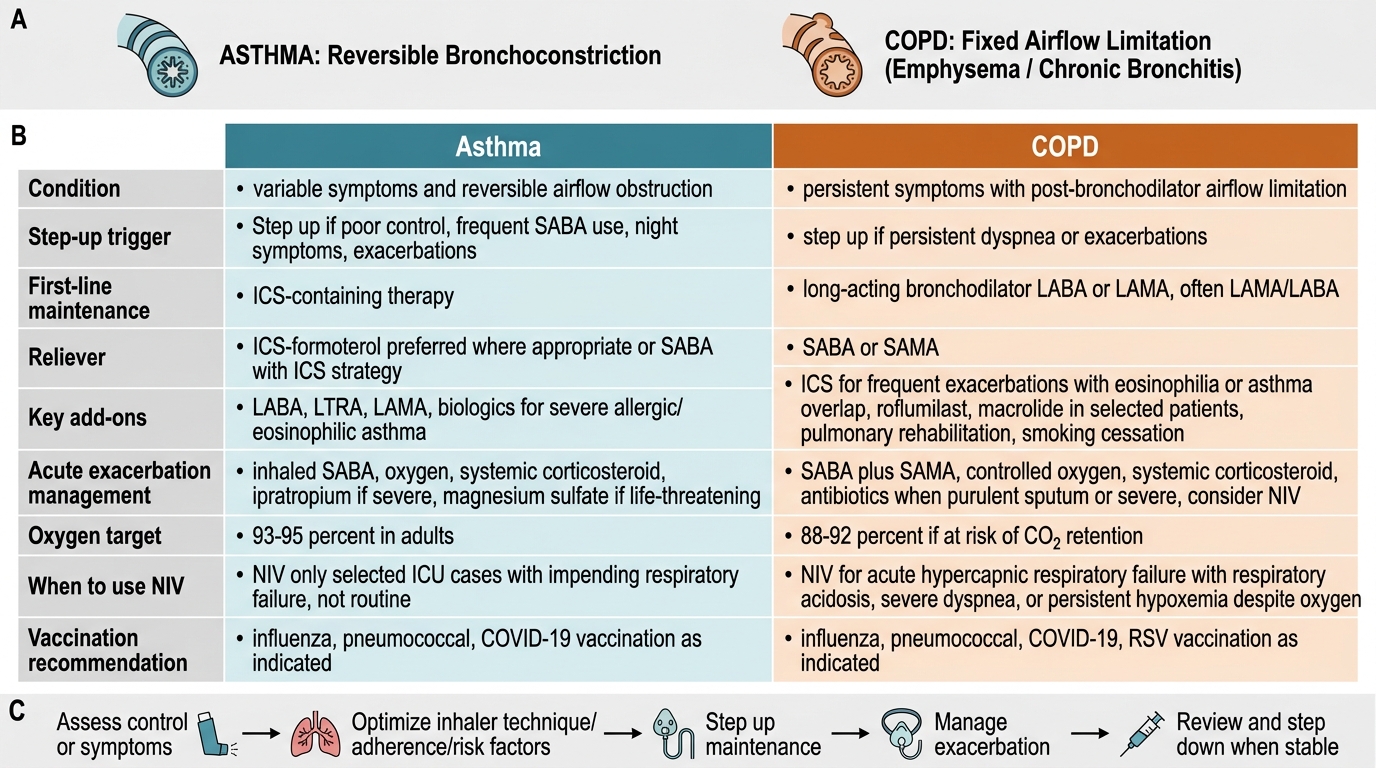
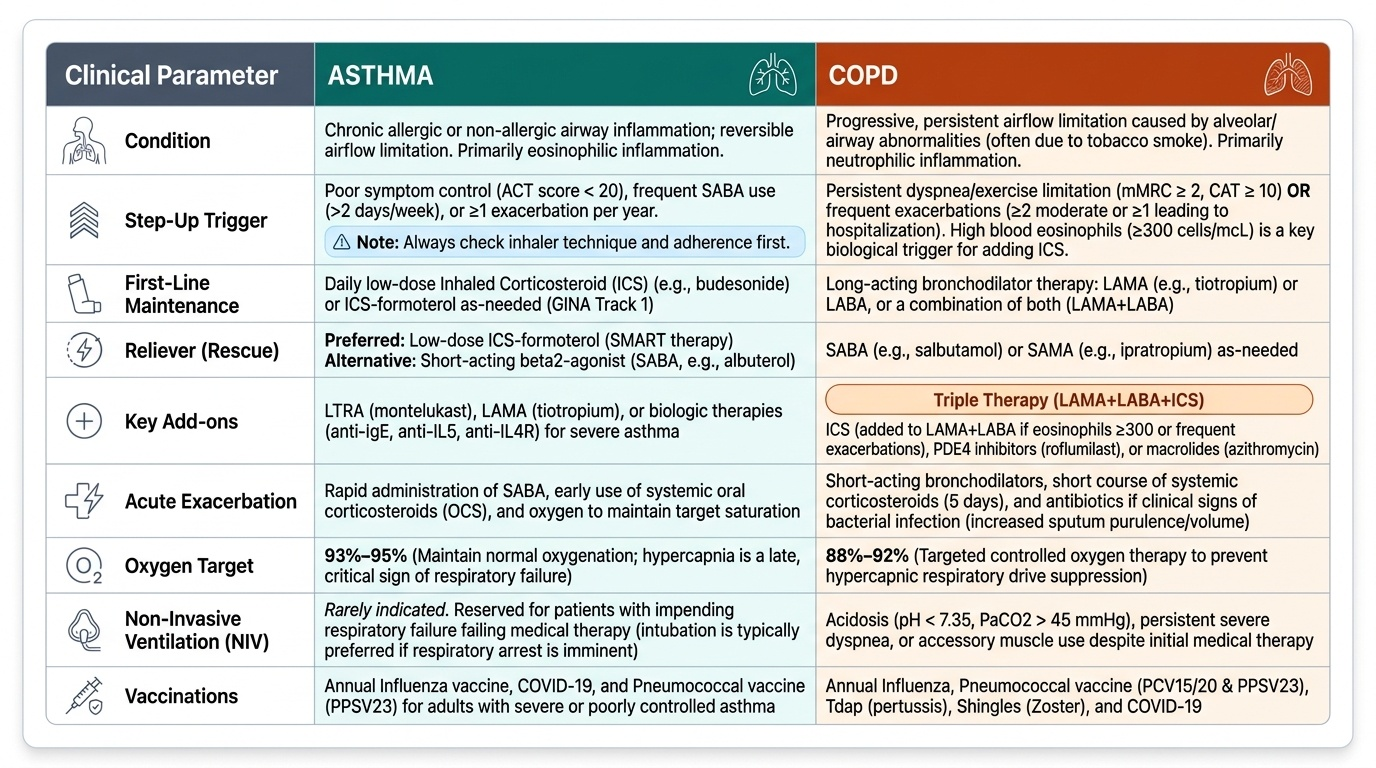
Asthma vs COPD: Treatment Principles