Page 12 of 20
IM3.15-22 | Pneumonia Treatment and Prevention — SDL Guide
Learning Objectives
- Select, prescribe, and justify an appropriate empirical antibiotic regimen for CAP, HAP/VAP, and aspiration pneumonia based on the clinical syndrome, host factors, and severity tier
- Review and adjust antibiotic therapy at 48–72 hours based on culture results and clinical response, applying de-escalation principles
- Apply the CURB-65 score and clinical judgment to determine the appropriate site of care and indications for ICU admission
- Identify the transmission-based precautions required for specific pneumonia pathogens (airborne for TB, droplet for influenza/Mycoplasma)
- Prescribe and titrate supplemental oxygen appropriate to the patient's diagnosis, including the different SpO2 targets for COPD versus non-COPD patients, and identify the indications for NIV and invasive mechanical ventilation
- Counsel patients and families on pneumonia diagnosis, treatment, and safety-net instructions; counsel eligible patients on pneumococcal and influenza vaccination
INSTRUCTIONS
This module covers the complete treatment and prevention framework for pneumonia. The clinical decisions covered here — antibiotic selection, de-escalation, oxygen titration, isolation, and vaccination counselling — are made daily in every acute medical setting and form the core of the junior doctor's clinical competence in respiratory medicine.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 121 — Pneumonia (textbook)
- API Textbook of Medicine, 10th ed. — Management of Respiratory Infections (textbook)
- IDSA/ATS Consensus Guidelines for Community-Acquired Pneumonia in Adults, 2019 (guideline)
- Indian Academy of Pediatrics (IAP) Immunization Schedule and Pneumococcal/Influenza Vaccine Recommendations, 2023 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 6 PM on a Saturday. You are the on-call medical officer at a district hospital in Tamil Nadu. Three patients are waiting: a 72-year-old man with CURB-65 of 4 who arrived by ambulance with oxygen saturation of 79%, a 28-year-old woman with HIV (CD4 unknown) presenting with two weeks of dry cough and worsening breathlessness, and a 55-year-old man who came in for a routine follow-up for his COPD and mentioned, almost as an afterthought, that he had not had his flu vaccine this year and wanted to know if he should get the pneumococcal vaccine too. Three patients, three fundamentally different treatment and prevention decisions. For the first, you must choose the right empirical antibiotic combination, decide on the site of care, titrate oxygen without suppressing his hypoxic drive, and determine the threshold for ventilatory escalation — all before the on-call consultant calls back. For the second, you must recognise that standard CAP antibiotics will not cover Pneumocystis, and that starting the wrong treatment may be more dangerous than the delay. For the third, you must know exactly who qualifies for pneumococcal and influenza vaccines and be able to counsel him accurately. This module gives you the clinical framework to manage all three.
WHY THIS MATTERS
The management competencies IM3.15 through IM3.22 span the full treatment and prevention spectrum for pneumonia — from empirical antibiotic prescription based on pharmacological principles (IM3.15), to culture-directed therapy (IM3.16), to the criteria for hospitalisation (IM3.17), isolation (IM3.18), supportive therapy including oxygen and ventilation (IM3.19), patient and family communication (IM3.20), and vaccination counselling (IM3.21, IM3.22). These are the competencies that translate diagnostic acuity into clinical action. In India, pneumonia remains the leading infectious cause of hospitalisation and death across all age groups — and each of these competencies has a direct and immediate impact on whether a patient survives, recovers without sequelae, and does not infect others, and whether their family understands the diagnosis and the treatment plan. The skills-level (SH) demands of IM3.15, IM3.16, IM3.20, and IM3.22 mean you must be able to prescribe, communicate, and counsel — not merely name the drugs or vaccines.
RECALL
Before proceeding, activate your pharmacology foundation. Beta-lactam antibiotics (penicillins, cephalosporins, carbapenems) inhibit penicillin-binding proteins (PBPs), blocking cell-wall peptidoglycan synthesis — bactericidal; their activity is time-dependent (the critical parameter is the time the free drug concentration exceeds the minimum inhibitory concentration, or T>MIC). Macrolides (azithromycin, clarithromycin, erythromycin) inhibit the 50S ribosomal subunit and protein synthesis — bacteriostatic against most organisms; they achieve excellent intracellular and tissue concentrations, making them effective against atypical intracellular organisms (Mycoplasma, Chlamydophila, Legionella). Fluoroquinolones (levofloxacin, moxifloxacin, ciprofloxacin) inhibit DNA gyrase (topoisomerase II) and topoisomerase IV — bactericidal; concentration-dependent activity; excellent bioavailability allowing switch from IV to oral; 'respiratory fluoroquinolones' (levofloxacin, moxifloxacin) cover Streptococcus pneumoniae (unlike older fluoroquinolones such as ciprofloxacin which have poor pneumococcal activity). Aminoglycosides (gentamicin, amikacin) inhibit the 30S ribosomal subunit — bactericidal; concentration-dependent; nephrotoxic and ototoxic; require therapeutic drug monitoring. Vancomycin inhibits cell-wall synthesis by binding to D-Ala-D-Ala terminus of peptidoglycan precursors — bactericidal against Gram-positive organisms; active against MRSA; requires trough level monitoring (target 15–20 mg/L for serious infections).
Clinical Presentation Recap and the Treatment Decision Framework
The treatment of pneumonia is driven by two simultaneous clinical streams that run in parallel from the moment the diagnosis is made: the empirical antibiotic selection stream (choose the right drug for the most likely pathogen based on the syndrome, host, and severity) and the supportive care stream (correct hypoxia, maintain haemodynamic stability, provide analgesia for pleuritic pain, ensure adequate hydration). Neither stream should wait for the other — antibiotics and oxygen are given simultaneously, and neither is optional in a hospitalised patient. The third stream — driven by microbiological results at 48–72 hours — enables de-escalation or escalation of the antibiotic regimen. Understanding this three-stream framework prevents both the error of waiting for cultures before starting treatment (which allows deterioration) and the error of never reviewing antibiotics once started (which drives resistance and adverse effects).
The first clinical decision in the treatment stream is to categorise the patient into the correct management tier, because the tier determines both the antibiotic choice and the site of care. This categorisation uses the same CURB-65 score derived from clinical examination and initial blood results: CURB-65 0–1 = low severity, ambulatory treatment appropriate, oral antibiotics; CURB-65 2 = intermediate severity, consider 24-hour observation or short hospital admission, oral or parenteral antibiotics depending on clinical condition; CURB-65 3–5 = high severity, hospital admission mandatory, parenteral antibiotics and oxygen; CURB-65 4–5 = high risk of death, ICU admission and ICU-level monitoring should be considered. Additional severity indicators that warrant escalation regardless of CURB-65: bilateral involvement on CXR, SpO2 persistently <90% on 6 L/min oxygen, PaO2 <60 mmHg on room air on ABG, systolic BP <90 mmHg despite fluids, new-onset confusion, or failure to improve clinically within 48–72 hours of appropriate treatment.
The guiding principles of antibiotic selection in empirical treatment are: (1) Spectrum adequacy — the empirical regimen must cover all plausible pathogens for the clinical syndrome, setting, and host immune status; (2) Pharmacokinetic/pharmacodynamic (PK/PD) appropriateness — dose, route (IV vs oral), frequency, and duration must be chosen to achieve the PK/PD target for the antibiotic class against the likely pathogen; (3) De-escalation commitment — the empirical choice should be reviewed at 48–72 hours and narrowed to the most targeted drug active against the identified pathogen; (4) Local antibiogram — the choice of agent must be informed by local resistance patterns, which vary significantly between Indian cities and regions; a hospital formulary reflecting local resistance data is essential for rational HAP/VAP management.
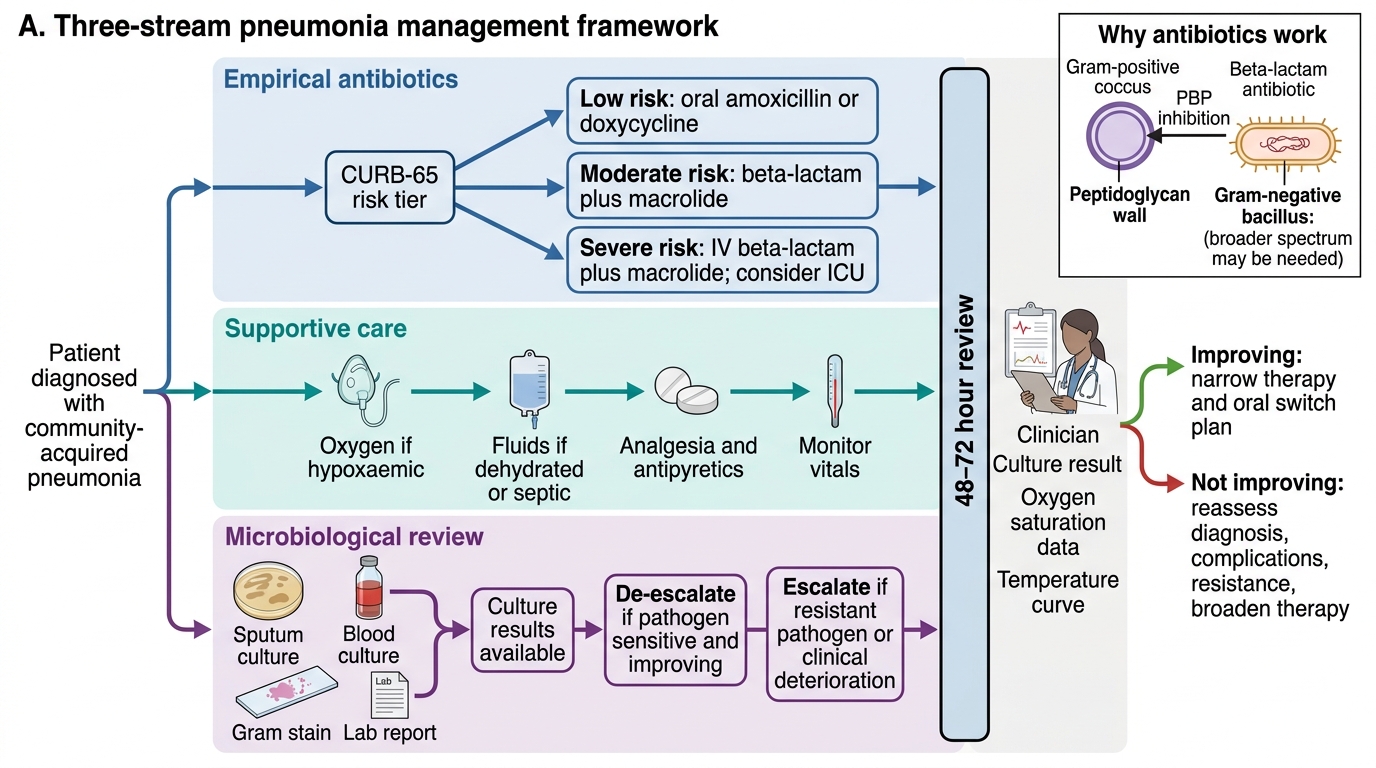
Three-Stream Pneumonia Management Framework
Pathophysiological Basis of Antibiotic Selection and Resistance
Understanding the pathophysiological and microbiological basis of antibiotic selection — rather than memorising regimens by rote — is what allows a clinician to adapt empirical therapy to unusual clinical scenarios, understand why de-escalation is safe, and explain resistance to a patient. The foundation of rational antibiotic prescribing in pneumonia rests on three paired concepts: the match between antibiotic spectrum and pathogen, the pharmacokinetic/pharmacodynamic (PK/PD) principle governing dosing, and the mechanisms of resistance that threaten effective therapy.
Antibiotic spectrum and organism type: The bacterial cell provides the structural and metabolic targets for antibiotic action. Beta-lactam antibiotics (penicillins, cephalosporins, carbapenems) share a common mechanism — inhibition of transpeptidases (penicillin-binding proteins, PBPs) that cross-link peptidoglycan chains in the bacterial cell wall. Gram-positive bacteria (S. pneumoniae, S. aureus) have a thick peptidoglycan layer as their outer boundary and are therefore primary targets for beta-lactams. Gram-negative bacteria have a thin peptidoglycan layer but are surrounded by an additional outer membrane (lipopolysaccharide layer) that beta-lactams must penetrate via porins — and loss or modification of these porins is a key resistance mechanism in Gram-negative HAP/VAP organisms. Atypical organisms (Mycoplasma, Chlamydophila, Legionella) have no cell wall at all — making beta-lactams intrinsically ineffective and requiring macrolides or fluoroquinolones, which target ribosomal or DNA targets present in all bacteria.
PK/PD principles in dosing: Beta-lactam activity is time-dependent: the critical parameter is the proportion of the dosing interval during which the free-drug concentration exceeds the minimum inhibitory concentration (T>MIC). This means that for beta-lactams, the critical dosing decisions are frequency and duration of infusion, not merely total dose — hence IV beta-lactams are often given three to four times daily, and extended infusion strategies (infusing over 3–4 hours rather than 30 minutes) may improve outcomes against partially resistant organisms by maximising T>MIC. Fluoroquinolones are concentration-dependent: their activity is optimised by achieving a peak concentration or area under the curve (AUC) that is well above the MIC — hence once-daily dosing of levofloxacin 750 mg achieves superior bactericidal activity compared to twice-daily lower-dose regimens.
Key resistance mechanisms in CAP and HAP/VAP pathogens: Penicillin resistance in S. pneumoniae arises from modification of PBPs (altered penicillin-binding proteins with reduced beta-lactam affinity) — NOT from beta-lactamase production; this is why co-amoxiclav does not overcome pneumococcal penicillin resistance, while higher-dose amoxicillin (3 g/day) or cephalosporins may. Beta-lactamase production in H. influenzae and Moraxella catarrhalis (and in Gram-negative organisms) hydrolyses the beta-lactam ring, inactivating penicillins — overcome by beta-lactamase inhibitors (clavulanate in co-amoxiclav; tazobactam in piperacillin-tazobactam). Extended-spectrum beta-lactamases (ESBLs) in Klebsiella and E. coli hydrolyse most penicillins and cephalosporins — carbapenems are required. Carbapenemases (NDM, OXA-48, KPC) in Klebsiella and Acinetobacter (particularly common in Indian hospitals) destroy carbapenems — the last-resort options are colistin and tigecycline. MRSA carries the mecA gene encoding an altered PBP2a that is not inhibited by any beta-lactam — requiring vancomycin, linezolid, or newer agents. The escalating resistance landscape in Indian hospitals is the direct context for the HAP/VAP empirical regimens that use piperacillin-tazobactam + aminoglycoside, and for the critical importance of de-escalating once culture susceptibility is confirmed.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
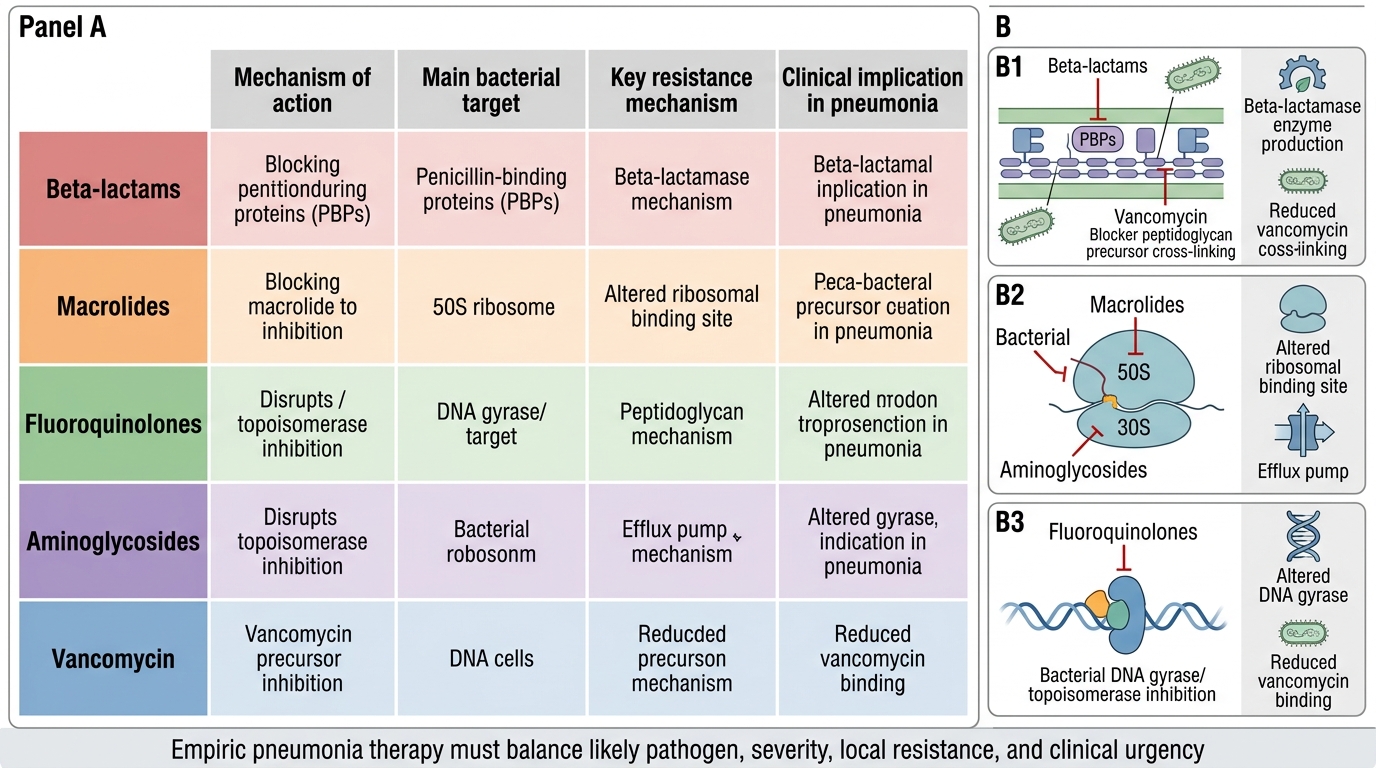
Antibiotic Mechanisms and Resistance in Pneumonia
Severity Assessment and the Diagnostic-to-Treatment Transition
The transition from the diagnostic to the treatment phase in pneumonia management is defined by the point at which sufficient clinical and investigative data are available to make three simultaneous decisions: the site of care, the empirical antibiotic regimen, and the initial oxygen and supportive care plan. This transition must occur within the first 1–4 hours of hospital presentation — evidence from large pneumonia cohort studies consistently shows that antibiotic delay beyond 4 hours from presentation is associated with increased 30-day mortality, particularly in severe CAP. The diagnostic and treatment phases are therefore not sequential but overlapping.
The central instrument for managing this transition is the CURB-65 score, which synthesises the five most reproducible clinical and biochemical severity markers into a single numeric score that drives care decisions. Each CURB-65 component reflects a distinct pathophysiological severity marker: C (Confusion) reflects cerebral hypoperfusion or the systemic inflammatory effects of bacteraemia — it is the most ominous single component because it indicates brain involvement; U (Urea >7 mmol/L) reflects renal hypoperfusion from systemic inflammatory response and sepsis physiology; R (Respiratory rate ≥30/min) reflects ventilatory compromise from consolidation and the metabolic demand of systemic infection; B (Blood pressure systolic <90 or diastolic ≤60) reflects cardiovascular decompensation, the clinical expression of early septic shock; and 65 (age ≥65) is a proxy for diminished physiological reserve and impaired acute immune response. The prognostic value of the score is that 30-day mortality rises approximately 10-fold from ~1.5% for CURB-65 0–1 to ~17–40% for CURB-65 4–5 — this mortality gradient is what justifies the categorical change in site of care and antibiotic route at each tier.
Beyond CURB-65, the diagnostic investigations inform the severity assessment and the antibiotic choice simultaneously. The ABG result determines the oxygenation tier (SpO2 alone may miss impending ventilatory failure — a rising PaCO2 in a COPD patient with apparently adequate SpO2 is the signal to escalate). The urea feeds directly into the CURB-65 score. Blood culture results, when they return at 48–72 hours, define the de-escalation decision. The CXR infiltrate extent (unilateral vs bilateral, lobar vs diffuse) modifies the severity estimate — bilateral infiltrates predict higher mortality independent of CURB-65 and should prompt consideration of ICU-level care even with a CURB-65 of 2–3. The PSI (Pneumonia Severity Index) — a 20-variable scoring system — is the alternative validated severity tool with higher discrimination than CURB-65 for low-risk outpatients; it is more cumbersome and less bedside-practical but may be used in research and some tertiary centres. For Indian district hospital practice, CURB-65 is the validated, practical, and clinically accepted tool.
The antibiotic prescription itself is a diagnostic act — the response to the empirical regimen at 48–72 hours is a diagnostic test. Improvement confirms that the empirical regimen covered the pathogen; non-improvement is a diagnostic signal to widen the differential (TB, malignancy, empyema, resistant organism, non-infectious diagnosis). This is why the empirical regimen must be documented with a specific 48–72 hour review date — it is not a standing order but a time-limited clinical hypothesis.
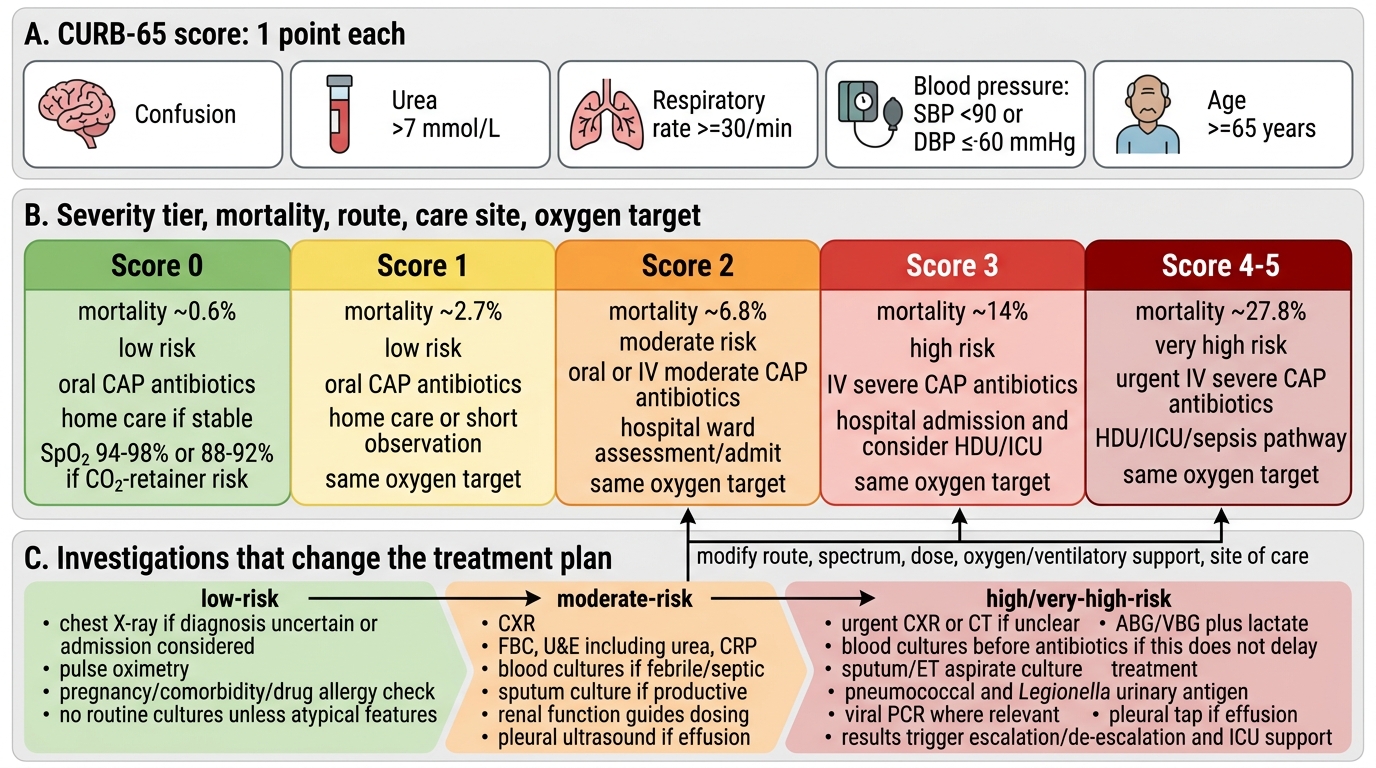
CURB-65 Severity Tiers in Pneumonia