Page 13 of 20
IM3.15-22 | Pneumonia Treatment and Prevention — SDL Guide (Part 2)
Empirical Antibiotic Selection: CAP, HAP/VAP, and Aspiration Pneumonia
Empirical antibiotic selection is the most consequential clinical action in pneumonia management and the direct content of NMC competency IM3.15. The choice is made before pathogen identity is known, based on the syndrome classification, host factors, severity, and the pharmacological spectrum of available agents. The following framework operationalises this decision for the three main pneumonia syndromes.
Community-acquired pneumonia (CAP) — ambulatory treatment (CURB-65 0–1): In otherwise healthy adults without comorbidities, the dominant pathogen is Streptococcus pneumoniae, and the empirical choice is oral amoxicillin 500 mg–1 g three times daily for 5 days. Amoxicillin covers pneumococcus and H. influenzae. If atypical pathogen cover is needed (young adult, dry cough, walking pneumonia picture, or failure of prior amoxicillin), add a macrolide (azithromycin 500 mg once daily for 3–5 days or clarithromycin 500 mg twice daily for 5 days) or use a respiratory fluoroquinolone (levofloxacin 750 mg once daily for 5 days) as monotherapy, which covers both typical and atypical pathogens. In patients with COPD or other structural lung disease, amoxicillin-clavulanate (625 mg three times daily) is preferred over plain amoxicillin, as it covers beta-lactamase-producing H. influenzae and Moraxella catarrhalis — both important COPD-related pathogens. Penicillin-allergic patients: use doxycycline 100 mg twice daily (covers atypicals and many typical organisms) or a respiratory fluoroquinolone.
CAP requiring hospitalisation (CURB-65 2 or ≥3, non-ICU): The standard inpatient regimen is a beta-lactam + macrolide combination: IV ceftriaxone 1–2 g once daily (or IV co-amoxiclav 1.2 g three times daily) PLUS azithromycin 500 mg IV or orally once daily. The rationale for dual therapy is that atypical pathogens (Legionella, Mycoplasma) are not covered by cephalosporins alone, and untreated Legionella in hospitalised severe CAP carries significant mortality. The duration of IV therapy should be the minimum necessary to achieve clinical stability (usually 2–3 days), at which point switching to oral therapy (a step-down strategy) reduces IV line complications, reduces hospital stay, and does not reduce efficacy in patients who are improving. An alternative for penicillin-allergic patients or those requiring simpler dosing: levofloxacin 750 mg IV once daily as monotherapy, which covers all CAP pathogens including Legionella with a single drug.
CAP — ICU-level severe (CURB-65 4–5, SpO2 <90% on oxygen, bilateral involvement): In the most severe cases, Legionella must be specifically covered; the regimen is IV ceftriaxone 2 g once daily PLUS IV azithromycin 500 mg once daily or IV levofloxacin 750 mg once daily. In patients with risk factors for Pseudomonas (structural lung disease, bronchiectasis, recent hospitalisation within 90 days, prior antibiotics within 90 days), replace ceftriaxone with an anti-pseudomonal agent: IV piperacillin-tazobactam 4.5 g three times daily or IV cefepime 2 g twice daily. If MRSA CAP is suspected (necrotising pneumonia with cavitation, severe post-influenza pneumonia), add IV vancomycin (15–20 mg/kg every 12 hours, targeting trough 15–20 mg/L) or IV linezolid 600 mg twice daily.
Hospital-acquired pneumonia (HAP) / Ventilator-associated pneumonia (VAP): The empirical regimen must cover MDR Gram-negative organisms. For early-onset HAP (within 4 days, no MDR risk factors): IV ceftriaxone 1–2 g once daily, as the pathogen profile is similar to CAP. For late-onset HAP or VAP (≥5 days, or any HAP with MDR risk factors): IV piperacillin-tazobactam 4.5 g three times daily OR IV cefepime 2 g three times daily OR IV imipenem-cilastatin 500 mg four times daily (carbapenem reserved for known ESBL producers or carbapenem-resistant organism settings). Add an aminoglycoside (gentamicin or amikacin) for double Gram-negative cover if Pseudomonas risk is high — combination therapy is recommended for empirical coverage of Pseudomonas in critically ill patients, then de-escalate to monotherapy once susceptibility is confirmed. For suspected MRSA: add IV vancomycin or IV linezolid.
Aspiration pneumonia: IV amoxicillin-clavulanate 1.2 g three times daily (covers anaerobes and oral Gram-negative organisms). Alternative: IV clindamycin 600 mg three times daily PLUS IV ceftriaxone 1 g once daily (for broader Gram-negative cover). If the patient aspirated in a hospital setting, treat as HAP with anti-pseudomonal cover.
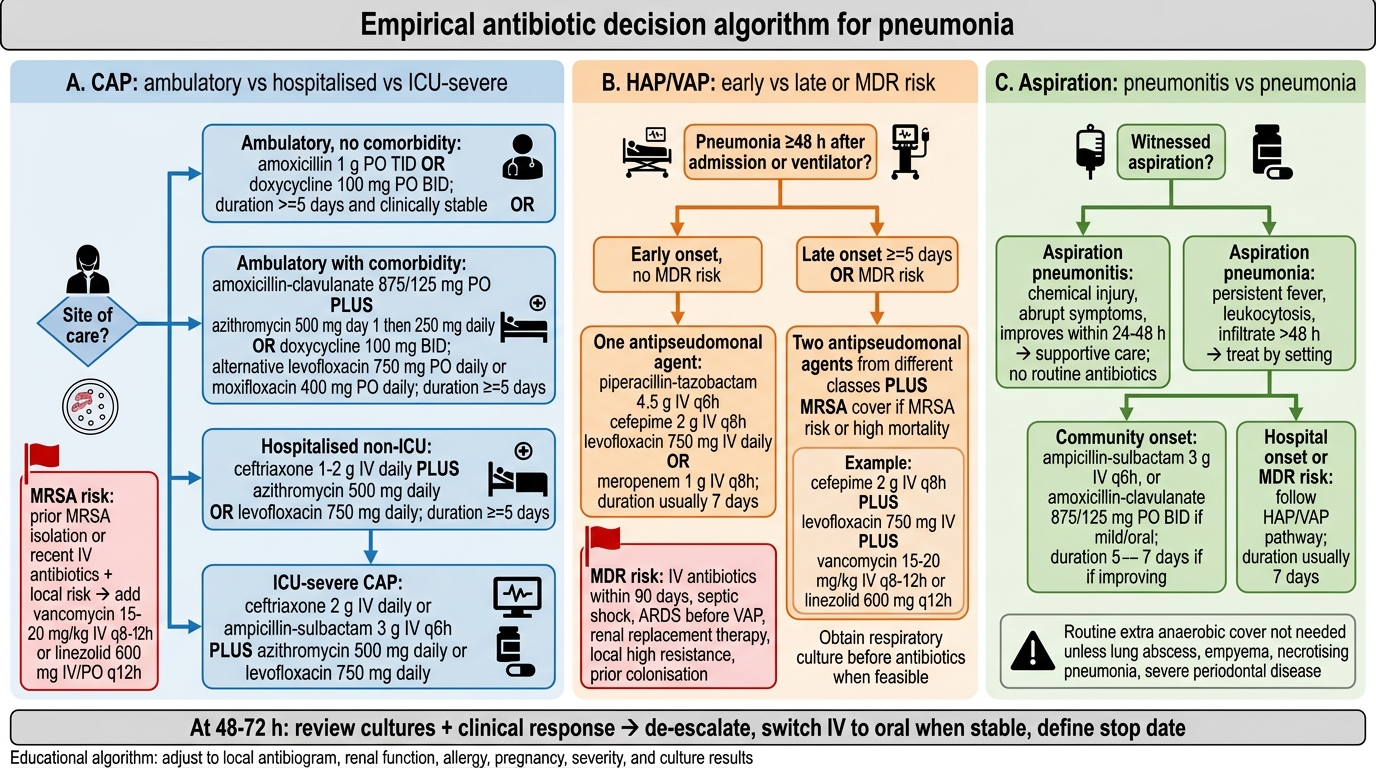
Empirical Antibiotic Algorithm for Pneumonia
Culture-Directed Therapy and Antibiotic Stewardship
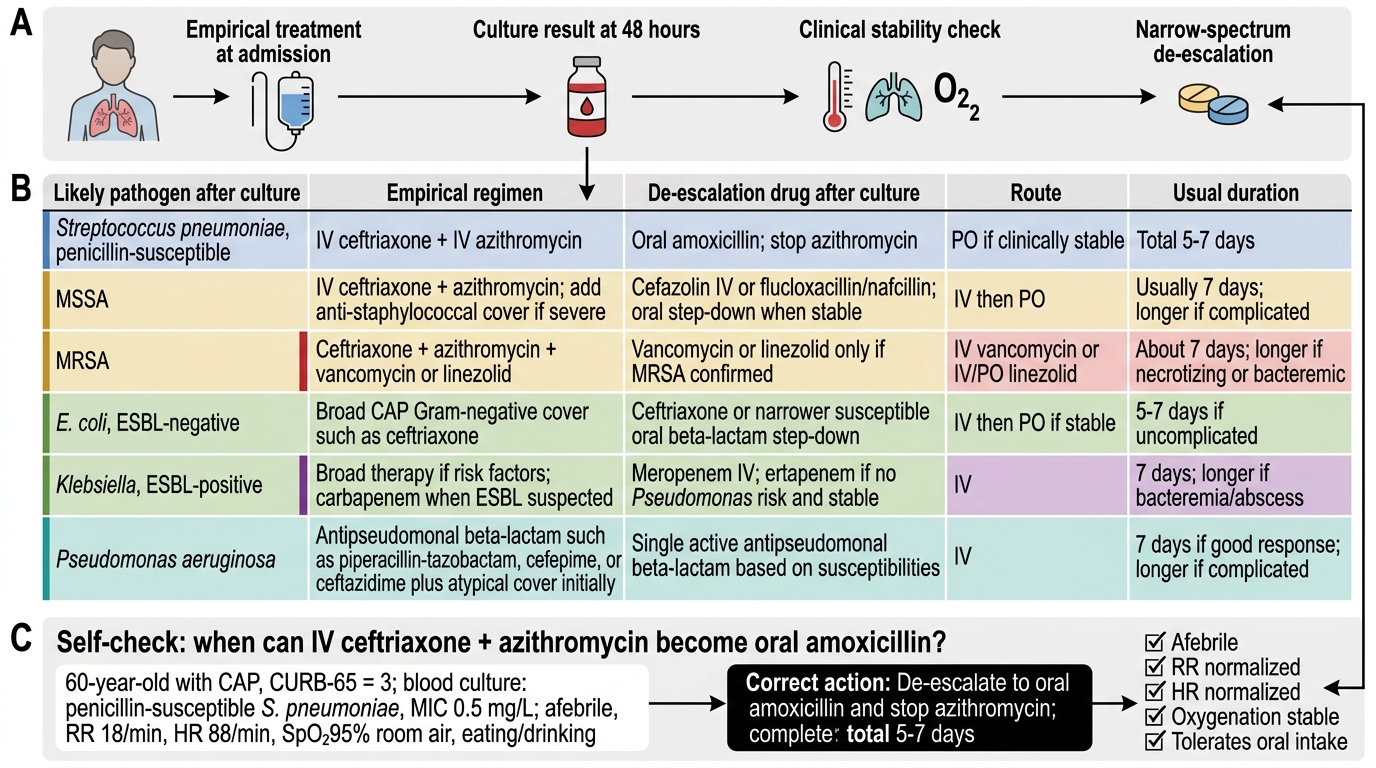
Culture-directed antibiotic therapy — the content of NMC competency IM3.16 — represents the transition from empirical to evidence-based treatment at 48–72 hours. It is the single most important opportunity for antibiotic stewardship in pneumonia management: narrowing the spectrum to cover only the identified pathogen reduces adverse drug effects, limits Clostridioides difficile risk, reduces cost, and — critically — slows the emergence of resistance. In the Indian hospital context, where multidrug-resistant organisms are prevalent and antibiotic use is often empirically broad and prolonged, the discipline of de-escalation based on culture results is a patient safety competency as much as a clinical one.
The culture result provides two pieces of information: the identity of the organism and its antibiotic sensitivity profile (the antibiogram, or MIC values for each tested drug). The clinical response at 48–72 hours provides the third piece of information: is the patient improving? The de-escalation decision integrates both. If blood cultures or sputum cultures confirm Streptococcus pneumoniae susceptible to penicillin (MIC ≤2 mg/L) and the patient is clinically improving, de-escalate from IV ceftriaxone + azithromycin to IV benzylpenicillin 1.2 g four times daily or, once oral therapy is feasible, oral amoxicillin 500 mg three times daily. The clinical switch criteria from IV to oral are: temperature <37.8°C for >24 hours, respiratory rate <25/min, heart rate <100/min, improving WBC count, tolerating oral intake, and SpO2 >94% on room air or on minimal oxygen. If blood cultures confirm Staphylococcus aureus susceptible to methicillin (MSSA), de-escalate from vancomycin (or maintain cover) to IV flucloxacillin 2 g four times daily — which has superior bactericidal activity against MSSA compared to vancomycin. If blood cultures confirm MRSA, continue or initiate vancomycin (trough 15–20 mg/L) or linezolid 600 mg twice daily. For Gram-negative bacteraemia with a confirmed sensitivity pattern, choose the narrowest drug covering the organism: for E. coli sensitive to co-amoxiclav, de-escalate from carbapenem to IV co-amoxiclav; for ESBL-producing Klebsiella confirming carbapenem sensitivity, continue the carbapenem (no de-escalation is possible when ESBLs are confirmed).
An important principle in culture interpretation: the antibiogram reports sensitivity for a single drug in ideal laboratory conditions (broth microdilution MIC testing) and may not perfectly predict clinical outcome — pharmacokinetic factors (drug penetration to the site of infection, protein binding, urinary vs. tissue concentration), the immune status of the host, and the burden of infection all modify the clinical response. A sensitivity report showing 'S' (sensitive) to a drug is a necessary but not sufficient condition for clinical cure. Always consider whether the drug will reach adequate concentrations at the infection site — for pneumococcal meningitis complicating CAP, the antibiotic must cross the blood-brain barrier, which narrows the choice to penicillin (high meningeal doses) or ceftriaxone, not all the drugs in the sensitivity panel.
Antibiotic stewardship in practice: (1) always review antibiotics at 48–72 hours with culture results and clinical response; (2) stop empirical double Gram-negative cover once sensitivity is confirmed (a single anti-pseudomonal agent is sufficient for a confirmed sensitive organism); (3) convert IV to oral as soon as clinical stability criteria are met — this reduces IV catheter infection risk; (4) set a target duration at the time of prescribing (5 days for non-severe CAP, 7 days for severe CAP, 7–14 days for HAP/VAP), not 'until clinically better'; (5) document the indication, choice, dose, route, and target duration in the case notes for every antibiotic prescription — this is the medicolegal standard and the stewardship record.
Antibiotic De-escalation in Pneumonia
SELF-CHECK
A 60-year-old man with CAP (CURB-65 3) is started on IV ceftriaxone + IV azithromycin. His blood culture at 48 hours grows Streptococcus pneumoniae sensitive to penicillin (MIC 0.5 mg/L). His temperature is 37.2°C, RR 18/min, HR 88/min, SpO2 95% on room air, and he is eating and drinking normally. What is the most appropriate antibiotic management now?
A. Continue IV ceftriaxone + azithromycin for 7 more days
B. Switch to IV vancomycin to cover possible penicillin resistance
C. De-escalate to oral amoxicillin and stop azithromycin — total 5–7 day course
D. Add an aminoglycoside for double cover of the identified pathogen
Reveal Answer
Answer: C. De-escalate to oral amoxicillin and stop azithromycin — total 5–7 day course
This patient meets clinical stability criteria (afebrile, RR normalised, HR normalised, SpO2 normal, tolerating oral intake) and the blood culture confirms a penicillin-susceptible S. pneumoniae. The correct antibiotic stewardship action is de-escalation: switch to oral amoxicillin 500 mg three times daily and discontinue azithromycin (the macrolide was added for atypical pathogen cover — now that the pathogen is confirmed as pneumococcus without atypicals, the macrolide is not needed). Total antibiotic course for non-severe CAP with clinical improvement: 5 days. Continuing broad-spectrum IV antibiotics beyond clinical stability is the most common antibiotic stewardship failure in pneumonia management.
Indications for Hospitalisation, Isolation, and Supportive Therapy
Three clinical management decisions are addressed by NMC competencies IM3.17, IM3.18, and IM3.19: when to hospitalise, when to isolate, and how to manage supportive care including oxygen and ventilation. Each decision has specific criteria that define the standard of care.
Indications for hospitalisation (IM3.17): The CURB-65 score is the primary tool. Hospitalise all patients with CURB-65 ≥3. Additionally, hospitalise regardless of CURB-65 for: SpO2 <92% on room air; bilateral lobar involvement on CXR; hypotension (systolic <90 mmHg or systolic fall >40 mmHg from baseline); inability to maintain oral hydration; failure to manage at home (lives alone, no carer, inability to comply with oral therapy); active comorbidities requiring monitoring (severe COPD, decompensated heart failure, AKI); immunocompromised state (HIV, neutropenia, transplant — requires closer monitoring for opportunistic infection); clinical concern of the attending physician despite a low CURB-65 score. Consider ICU admission for patients with CURB-65 ≥4, those requiring vasopressors, those with PaO2/FiO2 ratio <250 mmHg, bilateral infiltrates, or those who fail to maintain SpO2 ≥90% on high-flow oxygen.
Indications for isolation and barrier nursing (IM3.18): Not all pneumonias require isolation — the indication is based on the suspected or confirmed pathogen and its transmission route, not the diagnosis of pneumonia per se. Standard droplet precautions (surgical mask for healthcare worker within 1 metre, gloves, apron; single room preferred) are required for: confirmed or suspected influenza, parainfluenza, RSV, or other respiratory viral infections; pertussis; Mycoplasma pneumoniae; meningococcal pneumonia; pneumococcal pneumonia in the first 24 hours of treatment (until pathogen fully identified and susceptibility confirmed). Airborne precautions (N95 respirator for healthcare worker, negative-pressure room, door closed) are required for: confirmed or strongly suspected pulmonary tuberculosis (until three consecutive early-morning sputum smears are negative — a patient can be taken off isolation if smear-negative, though GeneXpert result should be followed); SARS-CoV-2 (COVID-19); Middle East Respiratory Syndrome (MERS); other airborne-transmitted pathogens. Standard precautions (gloves, handwashing) apply to all patients. Critically: in India, TB isolation is the most commonly indicated airborne isolation in respiratory medicine wards — any patient with suspected TB should be isolated as soon as the suspicion is raised, not after AFB smear results return (the pre-test probability may be high enough to justify isolation before results).
Supportive therapy: oxygen (IM3.19): The goal of oxygen therapy in pneumonia is to correct hypoxaemia while avoiding the complications of excessive oxygen. Targets: SpO2 ≥94% in all non-COPD patients; SpO2 88–92% in patients with confirmed or suspected COPD or type 2 respiratory failure (to avoid suppressing hypoxic drive). Oxygen delivery modes, in escalating intensity: (a) Nasal cannulae — 1–6 L/min, FiO2 ~24–44%; appropriate for mild hypoxia (SpO2 88–94%); (b) Simple face mask — 5–10 L/min, FiO2 ~40–60%; appropriate for moderate hypoxia; (c) Venturi mask — precise FiO2 (24%, 28%, 31%, 35%, 40%, 60%) by controlled air-entrainment; essential for COPD patients where precise FiO2 prevents CO2 retention; (d) Non-rebreather mask with reservoir bag — 10–15 L/min, FiO2 ~80–100%; for severe hypoxia requiring high FiO2 as a bridge; (e) High-flow nasal cannula (HFNC) — humidified, heated oxygen at flows up to 60 L/min, FiO2 up to 100%; reduces work of breathing by generating mild positive airway pressure and washing out nasopharyngeal dead space; the current standard of care for moderate-severe hypoxaemic respiratory failure before intubation in non-COPD patients; (f) Non-invasive ventilation (NIV, BiPAP/CPAP) — delivers positive pressure support via face mask; NIV (BiPAP: inspiratory positive airway pressure + expiratory positive airway pressure) reduces work of breathing and is the first-line ventilatory support for hypercapnic respiratory failure (type 2 failure) in COPD exacerbation; also used for immunocompromised patients with respiratory failure to avoid intubation; not appropriate for patients with severe haemodynamic instability, impaired consciousness, or inability to maintain the mask seal; (g) Invasive mechanical ventilation — endotracheal intubation and positive-pressure mechanical ventilation; indicated for: SpO2 persistently <88% on high-flow oxygen or HFNC; type 2 respiratory failure with pH <7.25 or falling level of consciousness despite NIV; haemodynamic instability; inability to protect the airway.
Additional supportive measures: IV fluid resuscitation for dehydration and early sepsis (30 mL/kg crystalloid bolus in first 3 hours for septic shock, per surviving sepsis campaign); vasopressors (noradrenaline first-line) if SpO2 remains <65 mmHg MAP despite 30 mL/kg fluids; analgesia for pleuritic chest pain (paracetamol 1 g four times daily ± an NSAID if no contraindication — adequate analgesia is important because pain inhibits deep breathing and coughing, worsening ventilation); antipyretics (paracetamol); deep vein thrombosis prophylaxis (LMWH enoxaparin 40 mg once daily SC in all immobile hospitalised patients without contraindication).
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
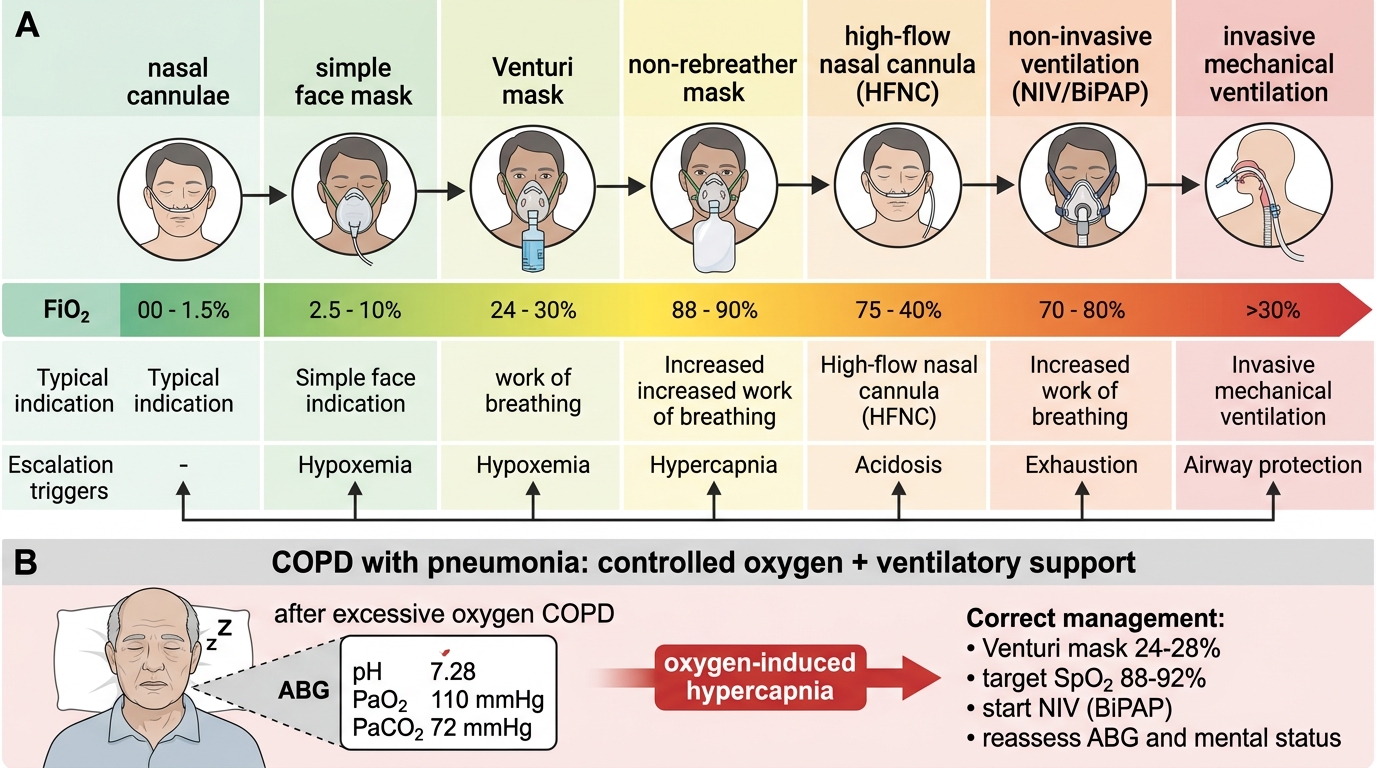
Oxygen Delivery Escalation Ladder in Pneumonia
SELF-CHECK
A 68-year-old man with known COPD is admitted with pneumonia. His SpO2 on room air is 82%. You start supplemental oxygen via a simple face mask at 8 L/min. Forty minutes later his SpO2 is 98% but he is drowsy and his RR has fallen from 28 to 10/min. An ABG shows: pH 7.28, PaO2 110 mmHg, PaCO2 72 mmHg. What is the correct management?
A. Increase oxygen to 15 L/min via non-rebreather mask
B. Maintain current oxygen, request urgent chest CT
C. Reduce oxygen to target SpO2 88–92% (use Venturi mask 24–28%) and start non-invasive ventilation (BiPAP)
D. Proceed to immediate intubation and mechanical ventilation
Reveal Answer
Answer: C. Reduce oxygen to target SpO2 88–92% (use Venturi mask 24–28%) and start non-invasive ventilation (BiPAP)
This is oxygen-induced hypercapnia in a COPD patient — a classic and preventable complication. The patient's hypoxic drive was his primary ventilatory stimulus; high-flow oxygen corrected the hypoxia but removed the stimulus to breathe, causing hypoventilation, CO2 retention (PaCO2 72 mmHg from a likely baseline of ~50 mmHg), and respiratory acidosis (pH 7.28). The correct management: (1) reduce oxygen to a controlled FiO2 targeting SpO2 88–92% (use a 24% or 28% Venturi mask — NOT the simple face mask at 8 L/min, which delivers uncontrolled FiO2); (2) initiate NIV (BiPAP) to support ventilation and reduce CO2 — NIV is the evidence-based first-line treatment for hypercapnic respiratory failure in COPD. Intubation is not yet indicated given the responsiveness and the availability of NIV; increasing oxygen would worsen the CO2 retention.