Page 14 of 20
IM3.15-22 | Pneumonia Treatment and Prevention — SDL Guide (Part 3)
Patient and Family Communication in Pneumonia
Effective communication with the patient and their family is an NMC-mandated clinical skill (IM3.20) and is as essential to good pneumonia management as the correct antibiotic choice. In the Indian healthcare context, patients frequently attend with a family member or group of family members who are the primary decision-makers in the household, and communicating accurately and empathetically with both the patient and the family is the norm rather than an exception. Poor communication leads to treatment non-adherence (incomplete antibiotic courses, failure to return for review), missed follow-up, failure to understand warning signs requiring emergency return, and loss of trust in the healthcare system.
A structured communication framework for pneumonia has three phases: diagnosis communication, treatment explanation, and safety-net counselling. The diagnosis should be explained in simple, accessible language: 'Your lungs have developed an infection — this is called pneumonia. Your body is fighting this infection, which is why you have a fever and it is hard to breathe. We have started medicines to fight the infection.' For patients who require hospitalisation, the rationale must be explained: 'The infection is serious enough that we need to give you medicines directly into a vein and watch you closely. We expect you to improve over the next few days with treatment.' For patients going home with oral antibiotics, the treatment explanation must include: the name of the antibiotic, the dose and timing (specific times to take it, with or without food), the duration (e.g., 'Take all 10 tablets — do not stop early even if you feel better, because stopping early allows the infection to return and the bacteria to become resistant'), and common side effects to expect and tolerate.
The most important communication task is the safety-net instruction — telling the patient and family exactly when to return to hospital. For outpatient CAP: 'Return immediately if: breathlessness gets worse or you cannot speak in full sentences; your lips or fingernails turn blue; you cannot take the tablets or are vomiting; you develop new confusion or are very drowsy; your fever goes above 39.5°C despite the tablets.' For hospitalised patients: 'We will keep you here until your fever goes down, your breathing is comfortable, and your oxygen levels are back to normal. Your family can ask the nurses any questions about how you are doing.' In Indian clinical settings, the family will often want a prognosis question answered ('Will he be alright?') — address this honestly and proportionately: for a low-severity CAP in a young healthy adult, reassurance is appropriate; for an elderly patient with CURB-65 of 4 and bilateral pneumonia, a frank but compassionate conversation about the severity of illness and the possibility of ICU escalation is required, framed around what is being done actively to support recovery.
For patients with HAP or VAP, family communication takes on additional dimensions: explaining that the patient's original hospitalisation for another condition has been complicated by a lung infection; the role of the ventilator (if applicable); the expected duration of treatment; and — in cases of severe MDR organisms — a frank discussion of prognosis and, when appropriate, treatment escalation/limitations. Documentation of all significant conversations is a medicolegal requirement.
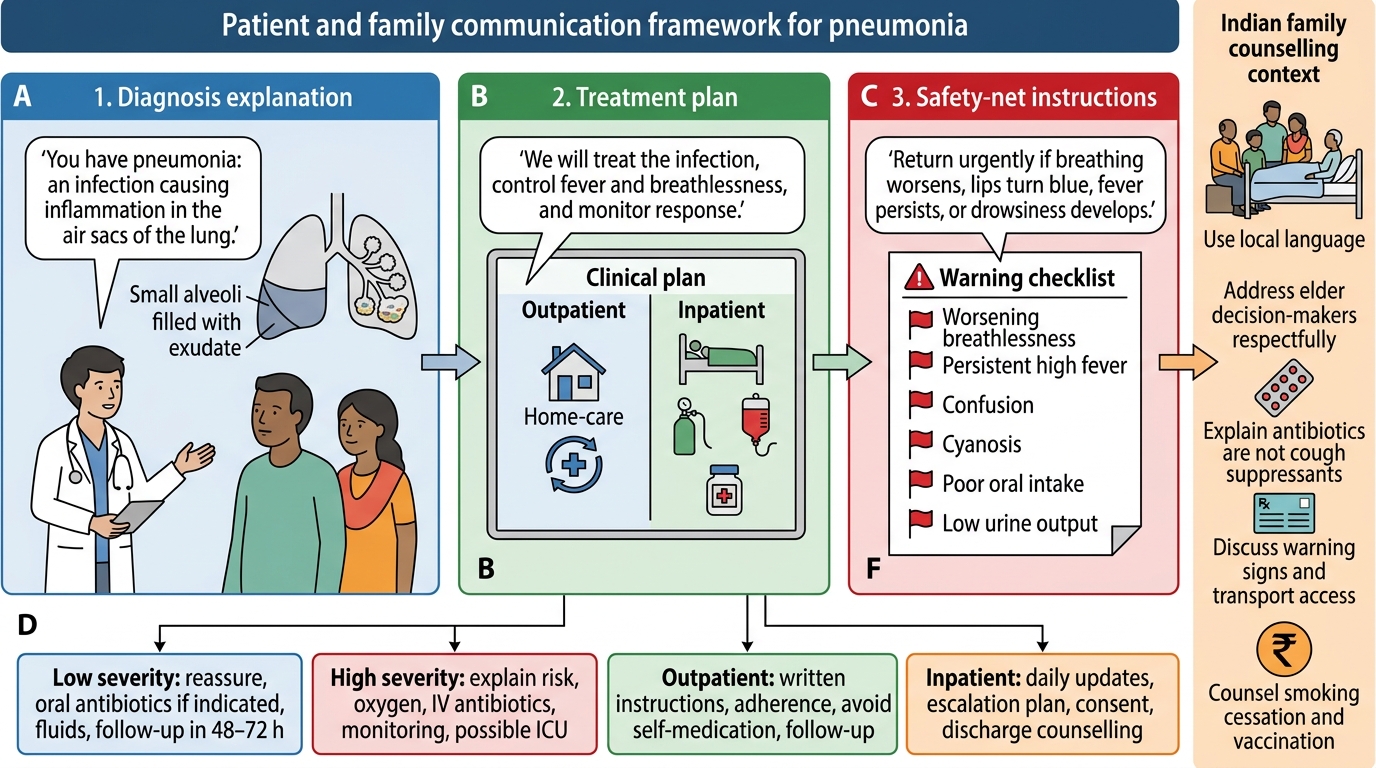
Pneumonia Communication Framework
Pneumococcal and Influenza Vaccination: Indications and Counselling
Prevention of pneumonia through vaccination is one of the most cost-effective interventions in clinical medicine, and the NMC competencies IM3.21 and IM3.22 require both knowledge of the indications and the ability to counsel patients. In India, vaccination against pneumococcal disease and influenza is systematically underutilised — knowledge of the specific eligibility criteria and the ability to identify and counsel eligible patients at every clinical contact are clinical skills that a final-year medical student must acquire.
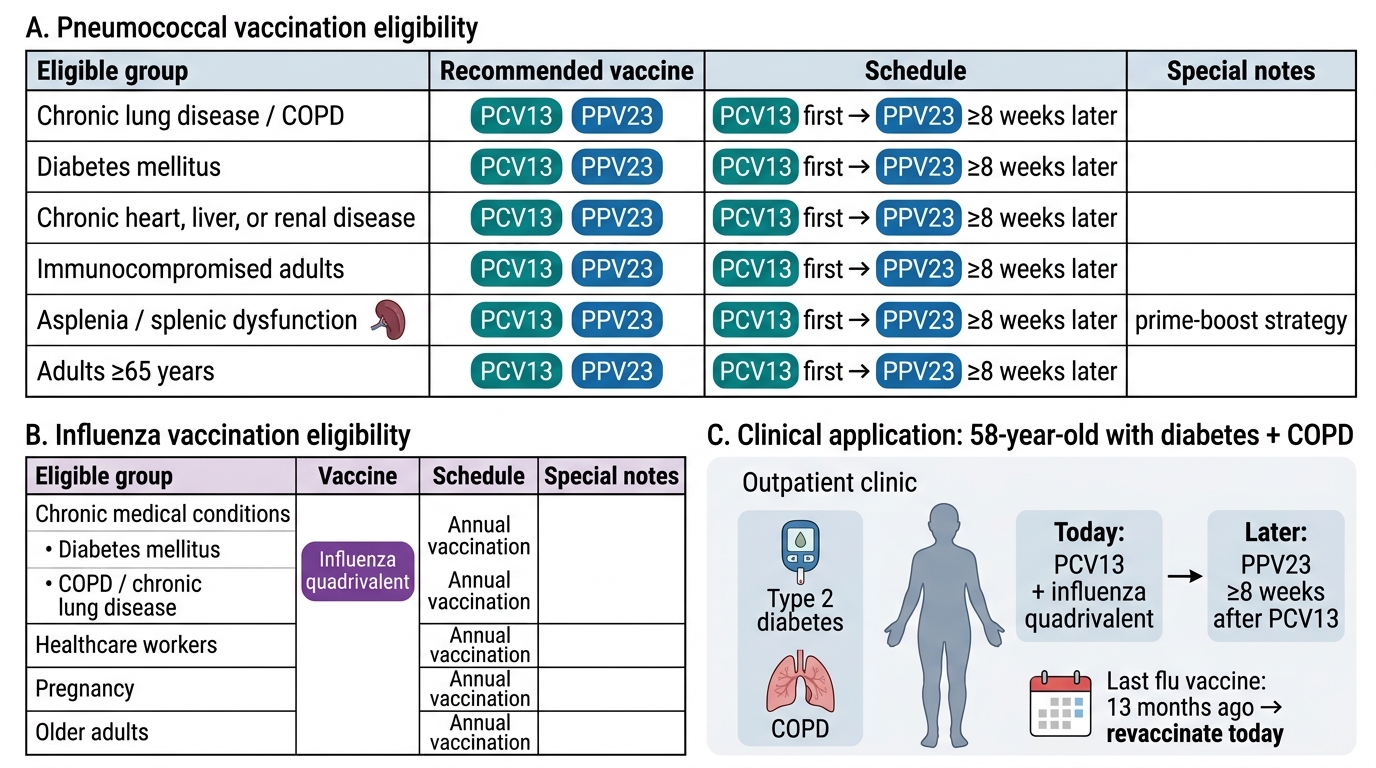
Pneumococcal vaccination: Two pneumococcal vaccines are available: the 23-valent polysaccharide vaccine (PPV23, Pneumovax) and the 13-valent conjugate vaccine (PCV13, Prevenar-13). The polysaccharide vaccine covers 23 pneumococcal serotypes responsible for ~85–90% of invasive pneumococcal disease; it induces T-cell-independent immunity and is less immunogenic in immunocompromised patients and children under 2 years. The conjugate vaccine covers 13 serotypes but uses a protein carrier that induces T-cell-dependent immunity, providing a more robust response in children and immunocompromised individuals. Indications for pneumococcal vaccination in adults (all age groups, not just the elderly): (1) Age ≥65 years — a single dose of PPV23 if not previously vaccinated; (2) Chronic lung disease — COPD, asthma requiring preventive treatment, bronchiectasis; (3) Chronic cardiovascular disease — heart failure, ischaemic heart disease, cardiomyopathy; (4) Diabetes mellitus — both type 1 and type 2; (5) Chronic kidney disease and nephrotic syndrome; (6) Chronic liver disease including cirrhosis; (7) Immunocompromised — HIV, haematological malignancy, solid organ transplant, immunosuppressive therapy, asplenia (anatomical or functional — asplenic patients have the highest risk of overwhelming pneumococcal sepsis and should ideally receive both PCV13 and PPV23 in sequence); (8) Cochlear implant recipients (high risk of pneumococcal meningitis via direct spread); (9) Residents of long-term care facilities. The preferred sequence for adults who have not previously been vaccinated: PCV13 first, then PPV23 ≥8 weeks later (the conjugate vaccine primes the immune system for a more robust polysaccharide response — the 'prime-boost' strategy). Re-vaccination with PPV23 at 5 years is recommended for immunocompromised patients and those ≥65 years who received their first dose before age 65.
Influenza vaccination: Annual influenza vaccination is recommended for the following groups: (1) All adults ≥65 years; (2) Pregnant women (any trimester — influenza poses particular risks during pregnancy including miscarriage, premature labour, and neonatal influenza); (3) Chronic medical conditions — heart disease, chronic lung disease (including COPD and asthma), chronic kidney disease, diabetes mellitus, chronic liver disease, haematological malignancy, haemoglobinopathy (sickle cell disease), obesity (BMI >30); (4) Immunocompromised patients — HIV, organ transplant, chemotherapy; (5) Healthcare workers — to prevent transmission to vulnerable patients; (6) Residents of long-term care facilities and their household contacts; (7) Children aged 6 months to 5 years and adults caring for children under 6 months (who are too young to be vaccinated themselves). The influenza vaccine is an inactivated (killed) vaccine for most formulations (safe in immunocompromised patients) — the live attenuated intranasal vaccine is available in some settings but should NOT be given to immunocompromised patients or pregnant women. Timing: the vaccine should be administered before the start of the influenza season (typically before October in the Northern Hemisphere; in India, before the winter respiratory season — October/November). Annual re-vaccination is required because influenza viruses undergo antigenic shift and drift, and the vaccine composition is updated annually to match circulating strains. The quadrivalent influenza vaccine (covering 2 influenza A strains and 2 influenza B strains) is now preferred over the trivalent vaccine.
Contraindications to pneumococcal and influenza vaccines: Severe allergy (anaphylaxis) to a previous dose or to a vaccine component (egg protein allergy is a relative contraindication to some influenza vaccines — patients with egg allergy can receive most modern influenza vaccines safely, but should be observed for 30 minutes post-vaccination). Acute febrile illness is a temporary deferral (postpone until fever resolves) — not an absolute contraindication. Pregnancy is NOT a contraindication to influenza vaccination (inactivated); it is a contraindication to live attenuated influenza vaccine only.
Vaccination Eligibility in Pneumonia Prevention
SELF-CHECK
A 58-year-old man with type 2 diabetes and COPD is attending your outpatient clinic. He has never received a pneumococcal vaccine. He received influenza vaccine 13 months ago. Which of the following is the MOST appropriate vaccination recommendation today?
A. PPV23 (pneumococcal polysaccharide) only — no influenza needed for another 11 months
B. PCV13 today, followed by PPV23 ≥8 weeks later; plus repeat annual influenza vaccine today
C. Influenza vaccine only — pneumococcal vaccine is only for patients aged ≥65 years
D. PPV23 today plus influenza vaccine; no need for PCV13 in adults
Reveal Answer
Answer: B. PCV13 today, followed by PPV23 ≥8 weeks later; plus repeat annual influenza vaccine today
This patient has two indications for pneumococcal vaccination (type 2 diabetes AND COPD — either alone is sufficient). The preferred sequence for a previously unvaccinated adult: PCV13 first, then PPV23 ≥8 weeks later (prime-boost strategy for optimal immunogenicity). For influenza: annual vaccination is recommended for patients with diabetes, COPD, and anyone aged ≥18 with chronic medical conditions — he received his last flu vaccine 13 months ago and should receive the current season's vaccine today (annual re-vaccination). Option A incorrectly defers influenza and misses the prime-boost sequence. Option C is wrong — pneumococcal vaccine is indicated below age 65 for multiple comorbid conditions. Option D misses PCV13 and the prime-boost sequence.
Self-Assessment: Integrating Treatment and Prevention
The competencies covered in this module — empirical antibiotic selection (IM3.15), culture-directed therapy (IM3.16), hospitalisation criteria (IM3.17), isolation indications (IM3.18), supportive therapy including oxygen and ventilation (IM3.19), patient and family communication (IM3.20), and vaccination (IM3.21, IM3.22) — represent the complete treatment and prevention framework for pneumonia. In clinical practice, these decisions are made rapidly, often under time pressure, and frequently with incomplete information. The discipline of applying a structured framework — CURB-65 for hospitalisation and antibiotic tier, oxygen target by COPD status, cultures before antibiotics, de-escalation at 48–72 hours, isolation by transmission route, and vaccination at every outpatient contact with an eligible patient — is what translates knowledge into consistently safe clinical practice.
The self-assessment below presents four integrated scenarios that require you to apply the full treatment and prevention framework, not individual components in isolation. For each, identify the empirical antibiotic regimen and route, the site of care, the oxygen target, isolation requirements, and the communication priorities. These scenarios are modelled on the types of clinical situations you will face in your first weeks as a junior doctor.

Integrated Pneumonia Treatment Decision Card
Scenario A: A 33-year-old previously healthy IT professional presents with 2 days of fever (39°C), productive cough with rust-coloured sputum, right-sided pleuritic chest pain, and an SpO2 of 94% on room air. CXR shows dense right lower lobe consolidation. CURB-65: age <65 (0), no confusion (0), RR 22/min (0), BP 128/80 (0), urea pending — assumed 0. CURB-65 = 0.
Management: Low-severity CAP. Outpatient treatment appropriate (CURB-65 0). Empirical antibiotic: oral amoxicillin 1 g three times daily for 5 days (pneumococcal CAP is the leading diagnosis — typical presentation with rust-coloured sputum, lobar consolidation, young adult). No isolation required for ambulatory care. Safety-net instructions: return if breathlessness worsens, lips turn blue, cannot complete sentences, fever >39.5°C on tablets. Follow up in 2–3 days for clinical response; repeat CXR at 6–8 weeks to confirm radiological clearance. Vaccination: offer influenza vaccine when acute illness resolves; check pneumococcal vaccination status.
Scenario B: A 72-year-old woman with heart failure and type 2 diabetes is admitted with confusion, fever 38.8°C, RR 32/min, BP 90/60 mmHg. SpO2 78% on room air. CXR: bilateral lower lobe infiltrates. Serum urea: 12 mmol/L. CURB-65: C (1) + U (1) + R (1) + B (1) + 65 (1) = 5.
Management: Severe CAP, CURB-65 5 — ICU-level care. Oxygen: start non-rebreather mask at 10–15 L/min, escalate to HFNC if needed; target SpO2 ≥94% (not COPD). IV fluids: 30 mL/kg crystalloid over 3 hours for septic shock. Empirical antibiotics: IV ceftriaxone 2 g once daily + IV azithromycin 500 mg once daily (severe CAP requiring ICU — Legionella must be covered). Blood cultures ×2 and sputum before antibiotics. Legionella urinary antigen. Droplet precautions in the first 24 hours. HIV test (PITC). Review at 48 hours: de-escalate if culture-confirmed pneumococcus. Communicate with family: severity of illness, ICU decision, risk of deterioration.
Scenario C: A 45-year-old ventilated patient in the surgical ICU develops new fever, purulent secretions, and a new bilateral CXR infiltrate on day 7 post-coronary artery bypass grafting (CABG). He received ceftriaxone for 3 days post-operatively for prophylaxis.
Management: Late-onset VAP with prior antibiotic exposure — high MDR risk. Isolation: contact precautions + droplet precautions until pathogen identified. Empirical antibiotics: IV piperacillin-tazobactam 4.5 g three times daily + IV amikacin 15 mg/kg once daily (double Gram-negative cover for Pseudomonas) + IV vancomycin 15 mg/kg twice daily (MRSA risk post-cardiac surgery). Endotracheal aspirate for Gram stain and culture before antibiotics. Review cultures at 48–72 hours for de-escalation. Ventilator bundle precautions (elevate head of bed 30–45°, oral decontamination, subglottic suction, pressure sore prevention) to prevent further VAP episodes.
CLINICAL PEARL
The single most preventable management error in pneumonia treatment is failing to review antibiotics at 48–72 hours. Empirical therapy is a clinical hypothesis — it is based on the most likely pathogen before the evidence is available. At 48–72 hours, the evidence arrives: blood culture results, sputum culture, clinical response, and sometimes a urinary antigen result. If a penicillin-sensitive S. pneumoniae is confirmed and the patient is improving, every day of continued broad-spectrum IV cephalosporin + macrolide instead of oral amoxicillin has a real cost: increased risk of C. difficile, increased IV line infection risk, prolonged hospitalisation, and contribution to institutional antibiotic resistance. Make the 48–72 hour antibiotic review a non-negotiable daily habit from your first week as a junior doctor — it is as important as the morning ward round vital signs check. For vaccination: every clinical contact with a patient who has diabetes, COPD, heart failure, or age ≥65 is an opportunity to ask 'Are you up to date with your pneumococcal and influenza vaccines?' — this opportunistic vaccination practice is the single most cost-effective preventive intervention in pneumonia public health.