Page 8 of 21
IM4.10-12 | Febrile Patient Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a medical history that comprehensively delineates the aetiology of fever, including fever evolution and pattern, associated symptoms, immune status, comorbidities, risk factors, and exposure through occupation, travel, and environment
- Perform a systematic physical examination that establishes the diagnosis and severity of a febrile presentation, including skin, mucosa, lymph nodes, chest, abdomen, liver, and spleen
- Generate a differential diagnosis for a febrile patient and prioritise it based on clinical features that distinguish infective, inflammatory, malignant, and rheumatological causes
INSTRUCTIONS
Clinical evaluation of the febrile patient is a performance skill — knowing the theory is necessary but insufficient without structured, disciplined practice at the bedside. This module walks you through the full history-taking and physical examination framework for fever, with emphasis on the diagnostic value of each manoeuvre and on integrating findings into a prioritised differential diagnosis.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 10–11 — Fever, FUO (textbook)
- API Textbook of Medicine, 10th ed., Ch. 3–4 — Fever (textbook)
- Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed., Ch. 27 — Fever (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are called to see a 36-year-old man in the emergency department. His temperature is 39.8°C, pulse 108 bpm, blood pressure 110/70 mmHg, respiratory rate 20 breaths/min. The triage card says 'fever 4 days'. That is all the information you have. Four days of fever in India has a differential that spans malaria, dengue, enteric fever, leptospirosis, scrub typhus, urinary tract infection, pneumonia, infective endocarditis, and dozens of less common diagnoses. In the next 20 minutes, your history and examination will narrow this list from dozens to three or four serious contenders — and will reveal whether this patient needs a malaria RDT and blood film, a urine culture and chest X-ray, or a blood culture set and echocardiogram. No investigation panel can substitute for the clinical information you are about to gather. This module teaches you exactly how to gather it.
WHY THIS MATTERS
The clinical evaluation of the febrile patient is the diagnostic skill that most directly translates academic knowledge into patient benefit. In high-income settings, investigations are relatively cheap and broadly accessible; in the majority of India's clinical environments — district hospitals, primary health centres, and rural settings — the targeted differential diagnosis generated from a skilled history and examination determines which of a limited set of investigations will be ordered and how quickly the patient will be treated. Misdiagnosing dengue as typhoid, or missing a scrub typhus eschar, or overlooking a new cardiac murmur, are errors that arise from incomplete history and examination — not from insufficient laboratory capacity. The NMC competencies IM4.10, IM4.11, and IM4.12 together describe the core clinical evaluation skill set expected of the graduating doctor.
RECALL
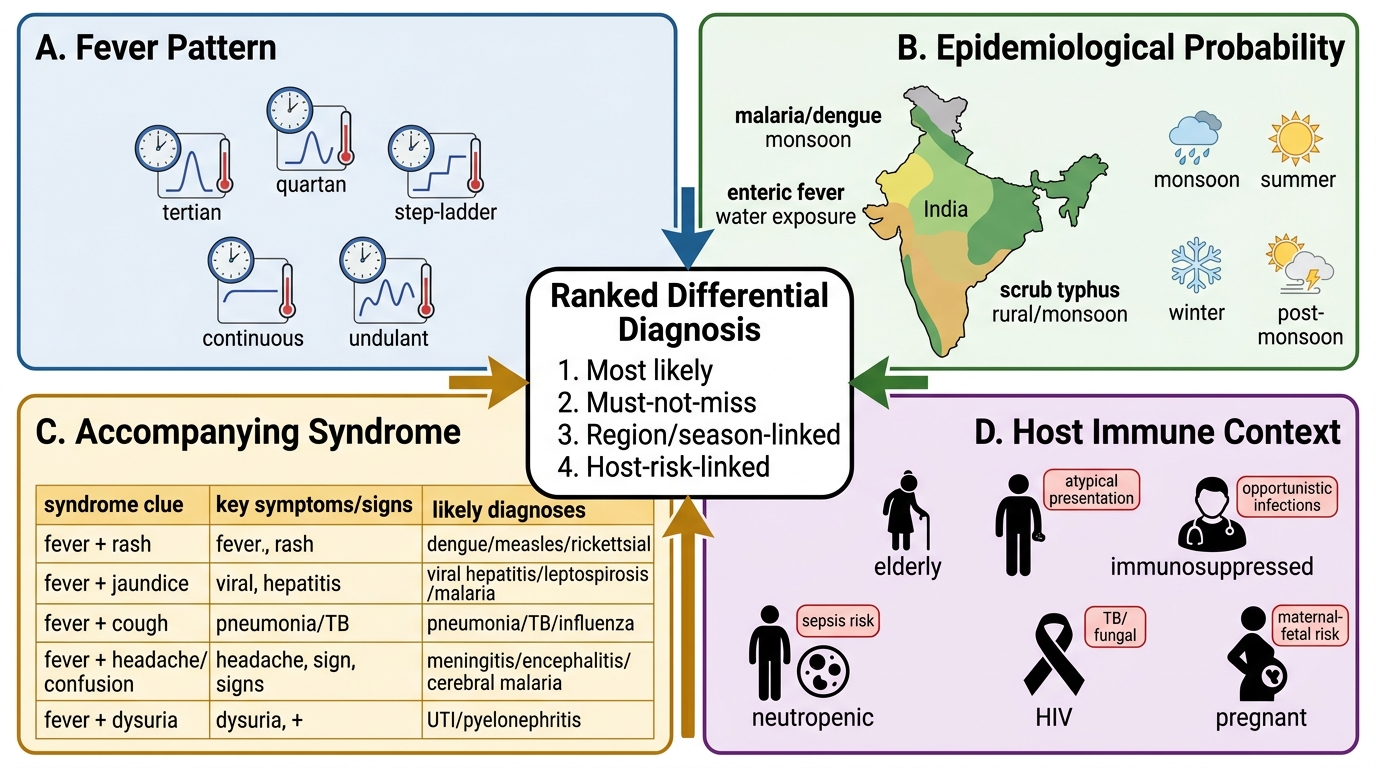
Connect this skills SDL to the mechanistic knowledge from Fever Foundations. The fever pattern reflects the periodicity of pathogen release into the bloodstream or the cytokine burst: tertian (48-hour) fever = Plasmodium vivax or falciparum; quartan (72-hour) fever = P. malariae; step-ladder fever = enteric fever (Salmonella typhi); continuous fever (minimal daily variation) = bacterial pneumonia, Gram-negative bacteraemia; quotidian double-spike = adult-onset Still's disease; undulant fever (waves of fever with afebrile intervals) = brucellosis; hectic or remittent fever (large daily swings) = abscess, TB. The physical examination manoeuvres you will learn derive their diagnostic value from anatomical and pathological changes: splenomegaly from reticuloendothelial hyperplasia (malaria, kala-azar, typhoid, infective endocarditis); hepatomegaly from inflammatory or infiltrative change (viral hepatitis, amoebic abscess); lymphadenopathy from reactive hyperplasia or malignant infiltration; skin signs from vascular occlusion, direct pathogen seeding, or immune-complex deposition.
Clinical Indication and Relevance of Structured Fever Evaluation
A thorough, structured clinical evaluation is the single most powerful diagnostic tool in the evaluation of a febrile patient. Studies of fever workup in resource-limited settings consistently show that the history and physical examination determine the final diagnosis in the majority of cases — investigations confirm or refine a probability already established at the bedside. The NMC competency IM4.10 establishes that the graduating doctor must be able to elicit and document a history that delineates the fever aetiology systematically. Competency IM4.11 establishes that the examination must be methodical and complete. Together these competencies underpin IM4.12 — the ability to generate a prioritised differential diagnosis distinguishing infective, inflammatory, malignant, and rheumatological causes.
The clinical indication for a structured evaluation of the febrile patient is the presentation itself — any patient with measured or reported fever warrants a systematic approach rather than an organ-specific examination. The reason is that the focus of infection or inflammation may not be clinically obvious: extrapulmonary TB presents without respiratory symptoms; infective endocarditis may have no localising symptoms initially; kala-azar presents as progressive constitutional decline with fever; and inflammatory causes (SLE, Still's disease) can mimic infection entirely. A non-systematic approach driven only by the patient's chief complaint will routinely miss the diagnosis.
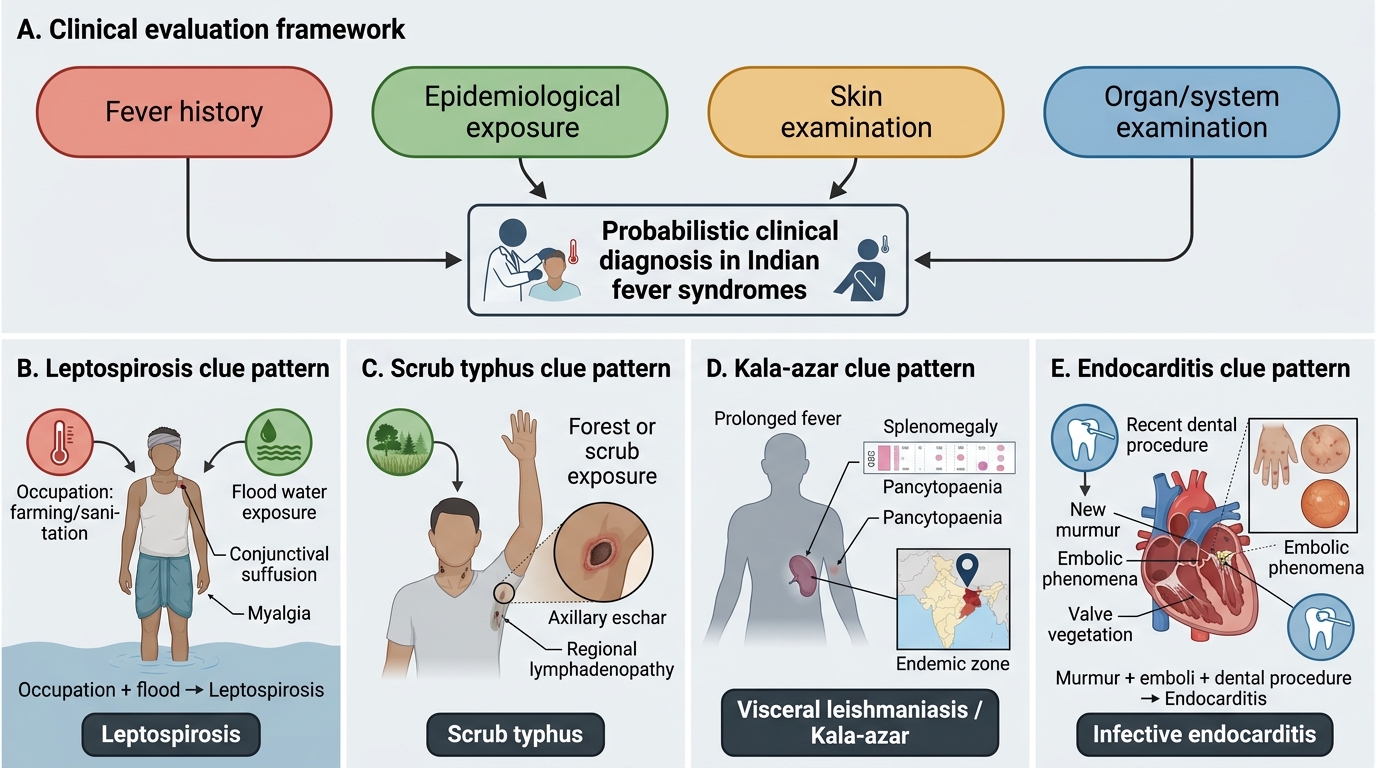
The clinical value of structured evaluation is proportional to the thoroughness of the examiner. In fever wards across India, common diagnostic errors include: failure to ask about occupation and geographic exposure (missing scrub typhus, leptospirosis, kala-azar), failure to perform a full skin survey (missing eschar of scrub typhus, rose spots of typhoid, petechiae of dengue or meningococcaemia), failure to examine for lymphadenopathy (missing lymphoma, HIV, infectious mononucleosis), and failure to auscultate the heart carefully (missing a new murmur of infective endocarditis). Each of these errors can be prevented by a structured, complete approach.
Clinical Clue Patterns in Indian Febrile Syndromes
Governing Principles: Fever Pattern and Differential Diagnosis Framework
The governing principle underlying clinical evaluation of the febrile patient is that every clinical finding has diagnostic discriminating power only within a probabilistic framework shaped by the patient's epidemiological context and host immune status. This principle determines what you ask, what you look for on examination, and how you weight the findings you discover. Understanding it prevents both under-investigation (dismissing a finding as irrelevant) and over-investigation (ordering every available test without a hypothesis).
The diagnostic power of fever pattern rests on the biology of pathogen replication and release. When P. vivax or falciparum merozoites rupture red blood cells every 48 hours, they release a bolus of GPI (glycosylphosphatidylinositol) anchors and Plasmodium falciparum erythrocyte membrane protein (PfEMP1) that triggers a cytokine surge — producing the episodic rigors-fever-sweat cycle that clinically manifests as tertian (every-other-day) fever. When Salmonella typhi bacteraemia gradually intensifies during the first week of enteric fever as the bacillary load builds up via the reticuloendothelial escape pathway, it produces a progressively climbing fever each day — the step-ladder pattern. When pyogenic bacteria invade the bloodstream episodically (as in bacteria seeding from a valve vegetation in endocarditis, or from pus in a liver abscess), they produce an intermittent hectic fever with large temperature swings. When the cytokine drive is continuous and sustained (solid bacterial pneumonia, Gram-negative bacteraemia, TB), the fever is continuous with small daily variation. These biological underpinnings give fever pattern its clinical value — recognising it requires precise fever charting, ideally a temperature chart plotted over time.
The governing framework for differential diagnosis integrates four simultaneous dimensions rather than a sequential checklist: (1) Fever pattern (as above); (2) Epidemiological probability — the geographic, occupational, and seasonal base-rate for each diagnosis in the patient's specific context; a tertian fever in a patient from Odisha is malaria until proved otherwise; the same fever pattern in a professor from an urban Delhi apartment is far less likely to be malaria; (3) Accompanying clinical syndrome — which combination of symptoms and signs points to a specific aetiology? Petechiae + thrombocytopaenia + retro-orbital pain + dengue zone = dengue warning signs; eschar + headache + forest exposure = scrub typhus; arthritis + malar rash + serositis = SLE; (4) Host immune context — the same bacteraemia that causes a high fever in a healthy adult may cause hypothermia or no fever in an elderly diabetic.
This four-dimensional framework should be constructed mentally as the history is taken and refined continuously as the physical examination proceeds — generating and testing hypotheses in real time, not after all data are collected. This iterative hypothesis-driven approach (sometimes called diagnostic reasoning or the Bayesian clinical approach) is the skill that distinguishes the experienced clinician from the novice who defers clinical judgment until the investigation results arrive.
Four-Quadrant Framework for Fever Differential Diagnosis
Procedure: History-Taking and Physical Examination Technique
History-taking for fever should follow a six-domain structured sequence that can be executed efficiently in 10–15 minutes. The six domains are: (1) Fever characterisation — onset, duration, maximum temperature, pattern (intermittent/continuous/remittent), rigors vs chills, response to antipyretics; (2) Associated symptoms — systematically cover neurological (headache, photophobia, confusion), respiratory (cough character, haemoptysis, dyspnoea), gastrointestinal (diarrhoea type, jaundice, abdominal pain), genitourinary (dysuria, loin pain), skin (rash — onset day, distribution, morphology), joints (arthralgia vs arthritis), and constitutional (weight loss, night sweats); (3) Epidemiological history — travel (domestic zone + international), occupation (agricultural/healthcare/sewer worker), water/food exposure (untreated water, unpasteurised dairy, flood), animal contact (livestock, dogs, rodents), sexual history and IVDU, vaccination status (typhoid, hepatitis A/B); (4) Drug history — all current medications, herbal remedies, recent antibiotics (timing and duration relative to fever onset); (5) Past medical and immune history — diabetes, HIV status and CD4 count, malignancy and current treatment, transplant immunosuppression, CKD, prior TB and treatment; (6) Family and household history — TB contact, household cluster of similar illness (dengue, typhoid).
For each domain, the key is not just asking the question but interpreting the answer in real time. When a patient says 'fever every other day with shivering', confirm the rigors are true rigors (whole-body shaking) versus simple chills, and immediately adjust the malaria probability upward. When a patient mentions working in agriculture in Odisha, the probability matrix shifts decisively toward falciparum malaria and leptospirosis.
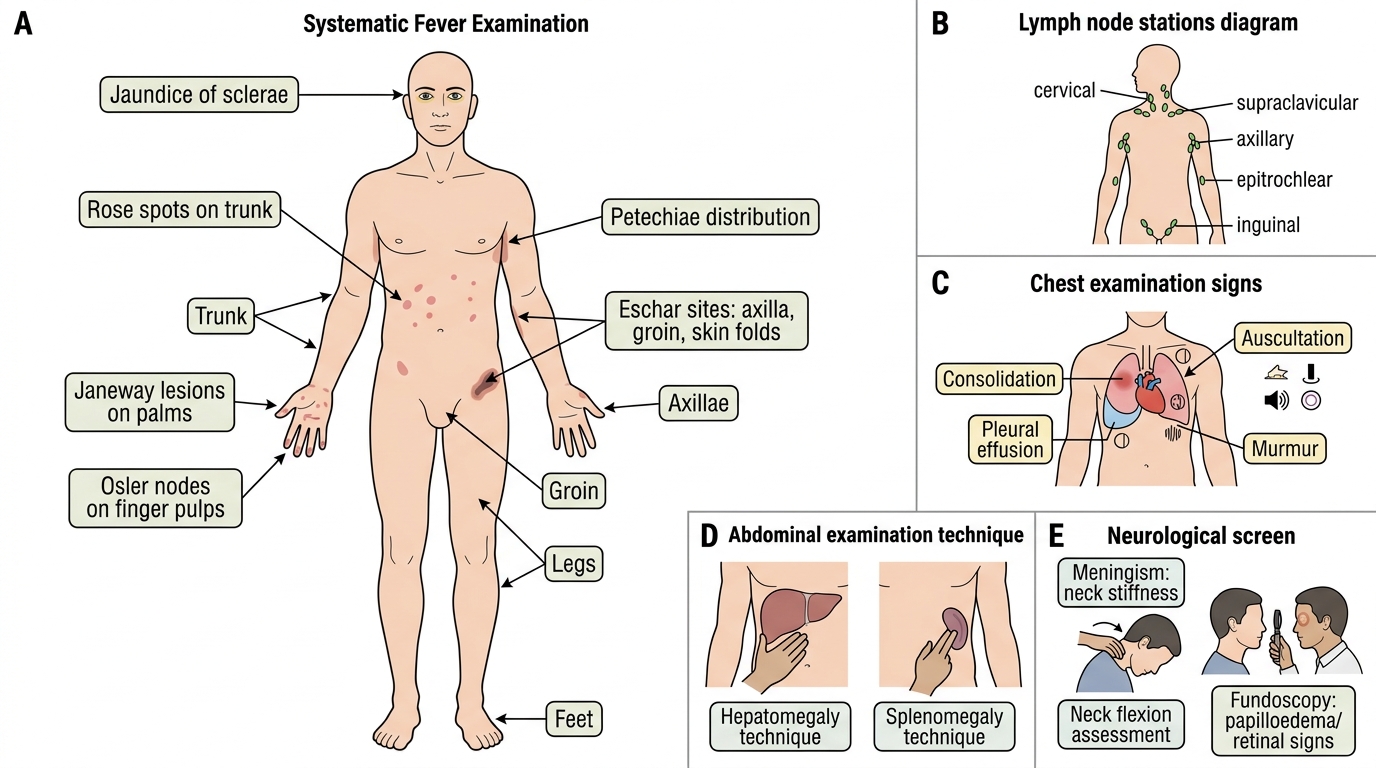
Physical examination technique for the febrile patient must be methodical: begin with vital signs, then proceed as follows. General inspection: level of consciousness (AVPU/GCS), hydration status (skin turgor, mucosae, sunken eyes), nutritional status (acute vs chronic illness wasting), pallor (conjunctival — best site for anaemia assessment), icterus (scleral). Skin and mucosal survey: undress the patient completely; inspect every skin surface including axillary folds, inguinal folds, scalp, behind the ears, and between the toes — specifically seeking: eschar (scrub typhus), petechiae/purpura (dengue/meningococcaemia), rose spots (typhoid), Janeway lesions (palms/soles, endocarditis), maculopapular rash (viral, rickettsial), jaundice distribution, and any track marks (IVDU). Inspect mucosae for: palatal petechiae (infectious mononucleosis), pharyngeal erythema, oral ulcers (HIV, SLE). Lymph node examination: palpate all accessible chains bilaterally — submental, submandibular, anterior and posterior cervical, supraclavicular, axillary (with the patient's arm relaxed at their side and your fingers deep into the axillary apex), epitrochlear, inguinal and femoral; note size, consistency, mobility, and tenderness. Cardiovascular examination: heart rate and rhythm (pulse character: bounding in vasodilated sepsis; irregular in AF — endocarditis risk); auscultate all four valve areas — document any murmur (location, grade, radiation, timing); check for pericardial rub (viral pericarditis, SLE, TB pericarditis). Respiratory examination: percussion (dullness = consolidation or effusion), auscultation (bronchial breathing + crepitations = consolidation; reduced breath sounds = effusion; fine bilateral end-inspiratory crepitations = PJP or ARDS). Abdominal examination: inspect for distension, surgical scars, caput medusae; palpate methodically — hepatomegaly (below the right costal margin in the midclavicular line, at least 2–3 cm = significant; note edge character — tender/smooth = acute hepatitis; irregular = cirrhosis or HCC); splenomegaly (begin palpation from the right iliac fossa and move toward the left costal margin — never start palpation at the costal margin or a massive spleen will be missed; use the Hackney percussion technique to detect splenic dullness before the spleen is palpable); signs of ascites (shifting dullness). Neurological screen: brief cognitive assessment; cranial nerve survey; meningism (neck stiffness, Kernig sign, Brudzinski sign — essential in any febrile patient with headache); fundoscopy (papilloedema = raised ICP; choroidal tubercles = miliary TB; Roth spots = endocarditis; cotton-wool spots = HIV retinopathy). Renal angle percussion: costovertebral angle tenderness = pyelonephritis.
Systematic Examination Checklist in Fever
SELF-CHECK
A 28-year-old who returned from a trek in rural Tamil Nadu has had fever for 10 days with severe headache and myalgia. On examination, temperature is 39.6°C. While examining the axillary folds, you notice a 1 cm circular black-crusted lesion with surrounding erythema. The patient reports no pain at the site. What is this lesion, and what does it diagnose?
A. Janeway lesion; suggests infective endocarditis
B. An infected insect bite with cellulitis; order wound swab
C. Eschar from mite bite; strongly suggests scrub typhus (Orientia tsutsugamushi)
D. Ecthyma gangrenosum; suggests Pseudomonas bacteraemia
Reveal Answer
Answer: C. Eschar from mite bite; strongly suggests scrub typhus (Orientia tsutsugamushi)
A painless black-crusted necrotic lesion (eschar) at the site of a mite bite in a patient from a rural or forested area with fever and headache is pathognomonic of scrub typhus, caused by Orientia tsutsugamushi transmitted by trombiculid mites. Scrub typhus is significantly under-diagnosed in India; the eschar may be found in concealed sites (axillae, inguinal folds, scalp, behind ears, between toes) and must be specifically sought. Janeway lesions are painless macules on palms and soles, not black crusted axillary lesions. Ecthyma gangrenosum is a necrotic ulcer from Pseudomonas in immunosuppressed patients, not a mite-bite eschar. The finding mandates doxycycline 100 mg twice daily for 7–14 days.