Page 9 of 21
IM4.10-12 | Febrile Patient Clinical Evaluation — SDL Guide (Part 2)
Interpretation of Findings: Integrating History and Examination into a Diagnosis
The interpretation of clinical findings in a febrile patient is an active synthesis process — each finding is not analysed in isolation but is weighted in the context of all other findings and the epidemiological framework. This section describes how to integrate the history and examination data into a probability-ranked differential diagnosis, which is the direct output of the clinical evaluation and the input to targeted investigation.
The interpretation of fever pattern: a well-documented tertian fever (rigors and sweat exactly every 48 hours) in a patient from a malaria-endemic zone makes malaria the lead diagnosis and should trigger an immediate peripheral blood smear and malaria RDT without waiting for further workup. A step-ladder fever charted over 7 days, with relative bradycardia on examination and a palpable spleen, in a patient who drinks municipal water or travelled in North India, makes typhoid the lead diagnosis and should trigger blood cultures (the highest-yield investigation in the first week). A continuous high fever with respiratory signs and tachypnoea in a previously healthy adult should trigger a chest X-ray immediately (pneumonia, TB). A double-spike quotidian fever with evanescent salmon rash and arthritis should prompt ferritin testing and consideration of adult-onset Still's disease.
The interpretation of skin findings: an eschar in an axillary fold of a patient from a forested area = scrub typhus (doxycycline immediately); petechiae in a non-dependent distribution with thrombocytopaenia = dengue (avoid aspirin/NSAIDs, monitor for warning signs); rose spots on the trunk with step-ladder fever and hepatosplenomegaly = typhoid (blood culture + chloramphenicol/ceftriaxone); Janeway lesions + Osler nodes + splinter haemorrhages + new murmur = infective endocarditis (blood cultures × 3 + echocardiography + urgent cardiology referral).
The interpretation of organomegaly: massive splenomegaly (≥8 cm below the costal margin) with prolonged fever and pancytopaenia in a patient from Bihar/Jharkhand/West Bengal = visceral leishmaniasis until proven otherwise (rK39 test + bone marrow aspirate). Moderate splenomegaly (3–6 cm) with intermittent fever and anaemia in a patient from Odisha = malaria (blood smear). Tender hepatomegaly with right upper quadrant pain and high fever in a patient who had recent dysentery = amoebic liver abscess (ultrasound abdomen immediately). Non-tender irregular hepatomegaly in an older patient with constitutional weight loss = malignancy (HCC, lymphoma — liver imaging and biopsy).
The interpretation of lymphadenopathy patterns: soft, tender, regional lymphadenopathy adjacent to an eschar or skin lesion = reactive to a local infectious focus; firm, non-tender, generalised lymphadenopathy (cervical + axillary + inguinal) in a febrile patient with weight loss = lymphoma or HIV or infectious mononucleosis; supraclavicular lymphadenopathy (Virchow's node on the left) = thoracic or abdominal malignancy until proven otherwise.
The interpretation of the cardiac examination: a new or changing murmur in a febrile patient with any bacteraemia risk factor (dental procedure in the preceding 6 weeks, IVDU, intravascular device, known structural heart disease) must be investigated for infective endocarditis. The absence of a murmur does NOT exclude endocarditis — right-sided endocarditis (in IVDU) and early-stage endocarditis may initially lack a murmur. Pericardial rub + fever + pleuritic chest pain = pericarditis (viral, TB, uraemic, post-MI).
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
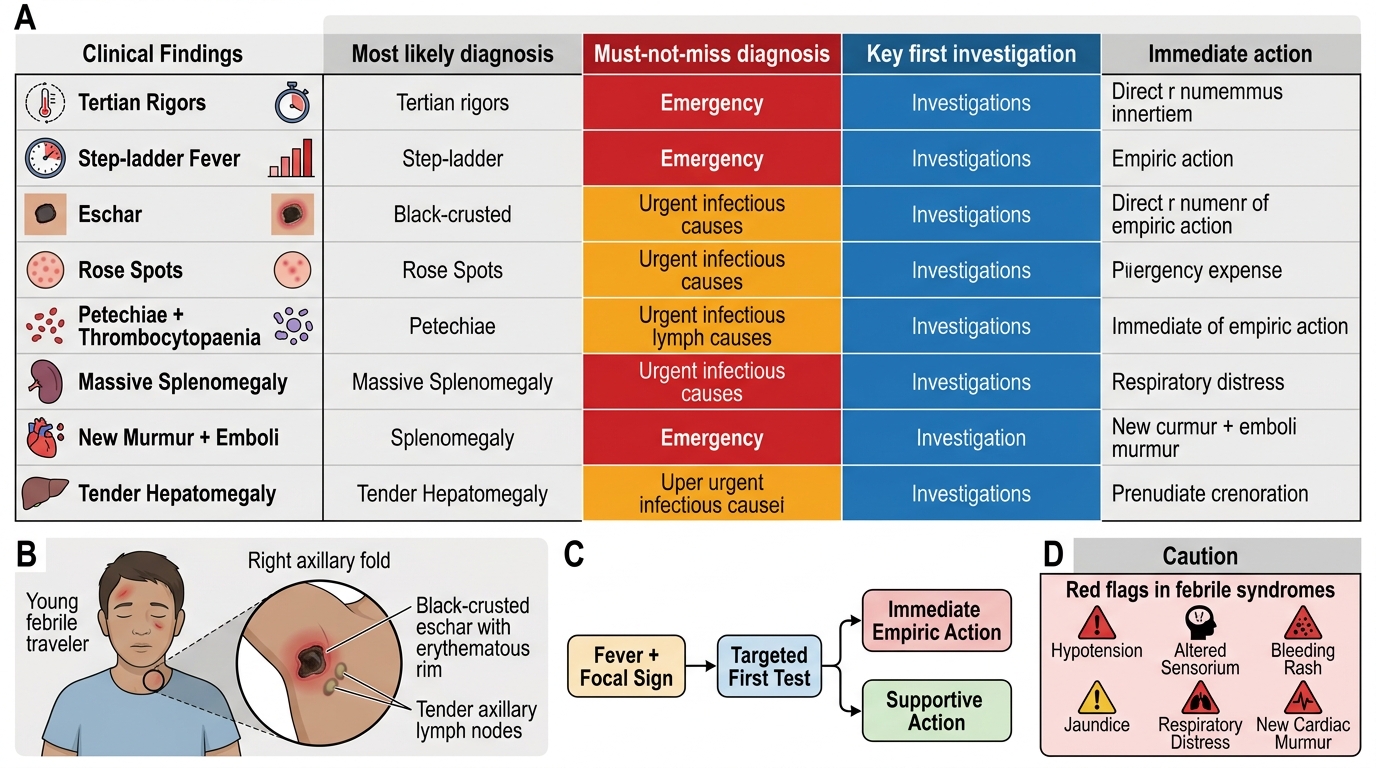
Interpretation Matrix for Fever and Febrile Syndromes
Applied Practice: Integrated Clinical Evaluation Scenarios
This section presents two clinical scenarios that require you to integrate history-taking, physical examination findings, and differential diagnosis generation — the three skills of this module. Work through each scenario independently before reading the analysis.
Scenario A: A 22-year-old male student, returning yesterday from a 10-day trip to Bihar near forested areas, presents to the outpatient department with 5 days of high fever (temperature 40°C), severe headache, and myalgia. No respiratory symptoms, no diarrhoea. On examination: temperature 39.6°C, pulse 116 bpm, blood pressure 108/68 mmHg. General: pallor not marked, mild jaundice absent. Skin: on careful inspection of the right axillary fold, a 0.8 cm circular black-crusted lesion is visible with surrounding erythema; no tenderness. Lymph nodes: bilateral axillary nodes 1 × 1 cm, tender. No hepatosplenomegaly. Chest: clear. No meningism. What is your ranked differential and what is the single most important next step?
Analysis: The most important clinical finding is the eschar in the axillary fold — a pathognomonic sign of scrub typhus (Orientia tsutsugamushi). The epidemiological context (forested Bihar), the combination of high fever, severe headache, myalgia, regional lymphadenopathy adjacent to the eschar site, and the eschar itself fulfil a clinical diagnosis. Ranked differential: (1) Most likely = scrub typhus; (2) Must not miss = falciparum malaria (Bihar, fever + headache — exclude immediately with blood smear + RDT); (3) Treatable and worth excluding = enteric fever (fecal-oral, Bihar — but pattern and exam do not fit). The most important next step: doxycycline 100 mg twice daily for 7–14 days should be started empirically — a rapid clinical response (defervescence within 24–48 hours) confirms the diagnosis. Order Weil-Felix (OXK) and IFA serology to confirm. Also order malaria RDT and blood smear to exclude concurrent falciparum malaria.
Scenario B: A 55-year-old woman with known rheumatic mitral valve disease presents with 3 weeks of fever (38.5–39°C), progressive weakness, and loss of appetite. She had a dental extraction 5 weeks ago. On examination: temperature 38.7°C, pulse 92 bpm irregular (atrial fibrillation). On inspection of the hands: three tiny painless erythematous macules on the thenar eminence of both palms; on the left ring finger pulp, a raised, tender red nodule is palpated. On fundoscopy: an oval pale-centred retinal haemorrhage is seen in the left eye. On auscultation: a pansystolic murmur at the apex radiating to the axilla, louder than previously documented. What is the diagnosis, what specific signs have you identified, and what are the immediate investigations?
Analysis: This is infective endocarditis on the mitral valve. The specific signs are: Janeway lesions (painless macules on palms — septic microemboli), Osler node (painful tender nodule on ring finger pulp — immune-complex deposition), Roth spot on fundoscopy (pale-centred retinal haemorrhage — immune-complex or embolic), and new or worsening mitral regurgitation murmur. The Duke criteria major criterion of echocardiographic evidence plus new murmur is met; positive blood cultures will complete the major criteria. Trigger: dental extraction 5 weeks ago (streptococcal bacteraemia from oral cavity). Immediate investigations: blood cultures × 3 sets from different sites before any antibiotic; transthoracic echocardiography (TEE if TTE quality is inadequate) to identify valve vegetations; CBC (anaemia, leucocytosis); CRP/ESR; urinalysis (haematuria from immune-complex glomerulonephritis = minor Duke criterion); renal function. Empiric IV antibiotics must start immediately after cultures are drawn — do not wait for culture results in a patient with hemodynamic compromise.
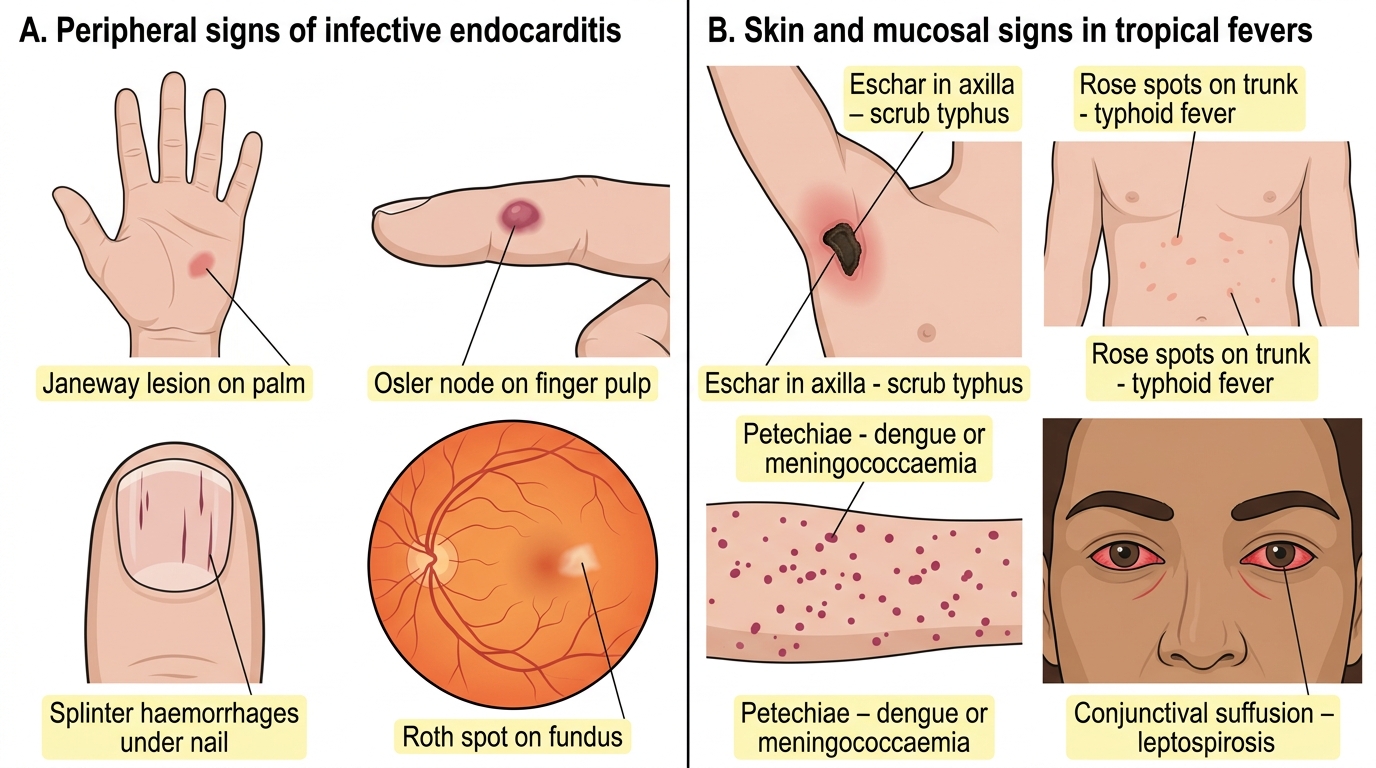
Bedside Signs in Infective Endocarditis and Tropical Fevers
SELF-CHECK
A 45-year-old with valvular heart disease has 3 weeks of fever, Janeway lesions, and Osler nodes. Three sets of blood cultures have been drawn. On auscultation, a new loud pansystolic murmur is heard at the apex. Chest X-ray shows pulmonary oedema. The NEXT most important step is:
A. Wait for blood culture results before initiating any treatment
B. Begin empiric IV antibiotics immediately after cultures are already drawn
C. Start oral amoxicillin-clavulanate and arrange outpatient echocardiography
D. Give IV diuretics alone to clear the pulmonary oedema and reassess
Reveal Answer
Answer: B. Begin empiric IV antibiotics immediately after cultures are already drawn
This is infective endocarditis with haemodynamic compromise — new severe mitral regurgitation causing acute pulmonary oedema. Blood cultures have already been drawn, so empiric IV antibiotics must be started immediately. The standard empiric regimen in native valve IE in India covers Streptococci and Staphylococci: IV benzylpenicillin + IV gentamicin, or IV vancomycin if MRSA is a concern. Waiting for culture results is inappropriate in haemodynamically compromised IE — mortality without antibiotics is extremely high. Oral antibiotics and outpatient management are not appropriate for severe IE with heart failure. Diuretics may be used adjunctively for pulmonary oedema but are not the primary intervention — antibiotics and urgent cardiology consultation for valve surgery are.
Self-Assessment: Clinical Evaluation Competency Check
This self-assessment section tests your command of the clinical evaluation framework developed in this module. For each clinical vignette below, identify the critical history finding or examination sign that directs the diagnosis, generate a three-tier differential diagnosis (most likely / must not miss / treatable), and identify the single most important first investigation. Then compare your answers with the analysis provided.
Case 1: A 40-year-old farmer from Uttar Pradesh has had fever for 12 days. The fever was measured by a local clinic as 40°C; at night he has drenching sweats. He also has generalised myalgia and a productive cough for the past 5 days. On examination: temperature 38.9°C, pulse 78 bpm (pulse rate seems low for this temperature), blood pressure 116/74 mmHg. Spleen palpable 4 cm below the left costal margin. No skin rash. Chest: dullness in the right lower zone with bronchial breathing.
Analysis: The most critical finding is relative bradycardia — a pulse of 78 bpm with a temperature of 38.9°C (expected HR would be approximately 100–105 bpm at this temperature). Relative bradycardia is a classic sign of enteric fever (Salmonella typhi). The splenomegaly is also consistent. However, the productive cough and dullness with bronchial breathing suggest concurrent right lower lobe pneumonia — either a complication of typhoid (pulmonary involvement occurs in 1–3% of enteric fever) or a coincidental community-acquired pneumonia. Three-tier differential: (1) Most likely = enteric fever with pulmonary complication; (2) Must not miss = falciparum malaria with secondary bacterial pneumonia (Uttar Pradesh, malaria zone — exclude with blood smear); (3) Treatable = community-acquired pneumonia alone (but relative bradycardia argues against pneumonia as the sole diagnosis). Key first investigation: blood cultures × 2 sets (typhoid diagnosis during first week, when sensitivity is highest — about 70–80%); plus malaria RDT/blood smear; plus chest X-ray.
Case 2: A 19-year-old woman has had fever for 3 weeks and bilateral knee and wrist arthritis. She has a butterfly-shaped facial rash and noted hair loss over the past month. She has lost 4 kg. No travel or occupational exposure history. On examination: temperature 38.6°C, malar erythema (butterfly rash), 2 cm oral ulcer on the buccal mucosa. Small bilateral pleural effusions on percussion. Tender wrists and knees with mild synovitis. No lymphadenopathy. Spleen not palpable.
Analysis: The critical combination is butterfly malar rash + arthritis + oral ulcer + pleural serositis + constitutional weight loss + prolonged fever in a young woman — this is the clinical presentation of systemic lupus erythematosus (SLE). The 2019 EULAR/ACR classification criteria for SLE are substantially met (constitutional fever, malar rash, oral ulcers, arthritis, serositis). Three-tier differential: (1) Most likely = SLE; (2) Must not miss = infectious endocarditis (fever + arthritis, but no cardiac murmur or embolic signs); disseminated TB (pleural effusion + constitutional, but malar rash not a TB feature); (3) Treatable = rheumatoid arthritis with pleuritis (but malar rash, oral ulcers, and young female argue for SLE over RA). Key investigation: ANA (high sensitivity screening — negative ANA makes SLE very unlikely); if ANA positive, proceed to anti-dsDNA (specific for SLE), complement (C3/C4 low in active SLE), CBC (cytopaenia is a classification criterion), urinalysis (proteinuria = lupus nephritis, which changes management urgency).
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
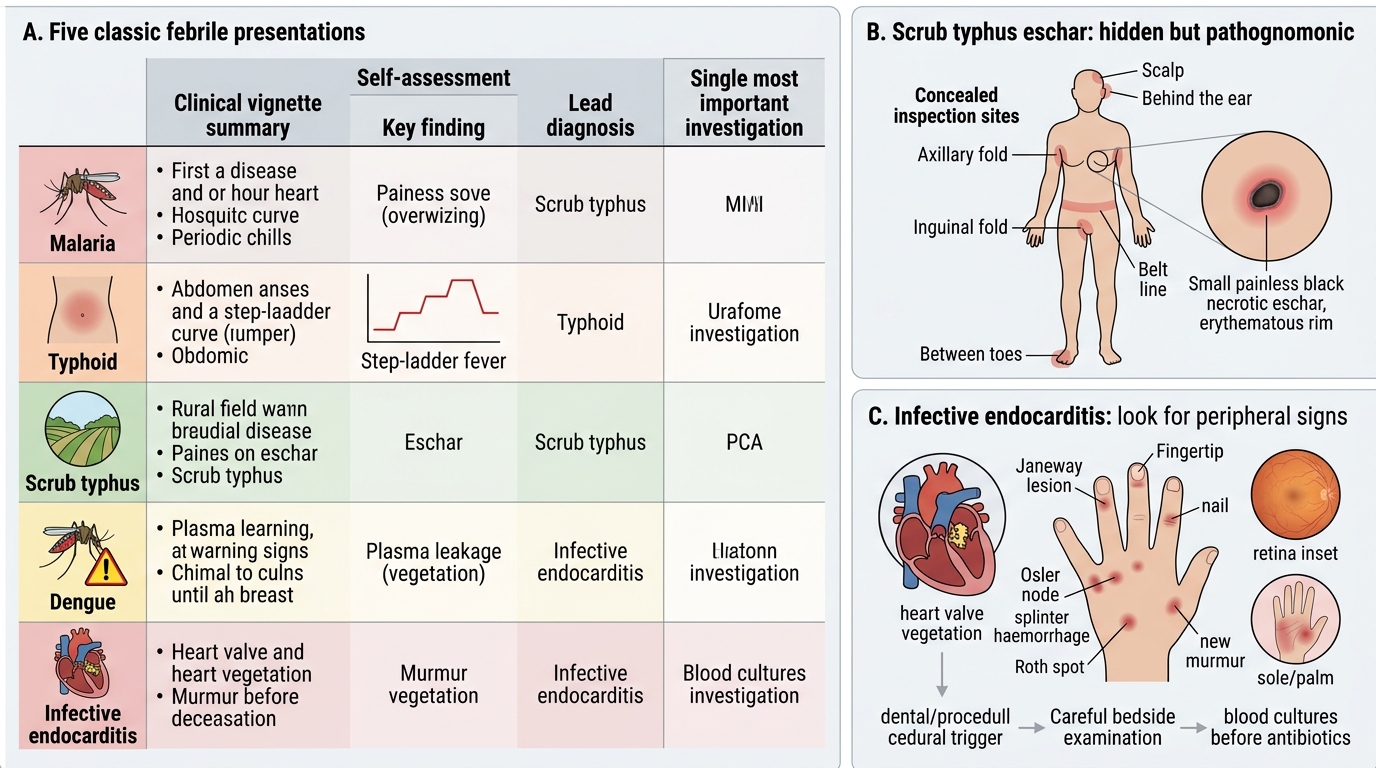
Five Classic Febrile Presentations: Diagnosis and Key Investigation
CLINICAL PEARL
The scrub typhus eschar is the most commonly missed bedside finding in febrile patients from rural and forested India. It is present in only 50–70% of Indian scrub typhus cases, but when present it is pathognomonic — no other diagnosis produces an eschar with this morphology in this setting. The trap is that it is small, painless, and located in concealed sites: axillary folds, inguinal folds, the scalp, behind the ears, between the toes, at the belt line, or under the breast. A systematic full skin inspection — not just a glance at the exposed skin — is the only way to find it. Similarly, the peripheral signs of infective endocarditis (Janeway lesions, Osler nodes, splinter haemorrhages, Roth spots) are individually low-sensitivity but collectively high-specificity when found together in a febrile patient with a murmur and a dental or procedural trigger. Both signs reward the examiner who takes deliberate time to look carefully.