Page 5 of 19
IM5.8-10 | Liver Disease Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a complete, structured history for a patient with liver disease, covering the six key domains: presentation, alcohol history, drug/herbal history, viral hepatitis risk factors, family history, and sexual/social history
- Perform a systematic, head-to-toe physical examination identifying the signs of chronic liver disease and portal hypertension in their correct anatomical context
- Explain the mechanisms underlying key clinical signs of chronic liver disease including spider naevi, palmar erythema, caput medusae, leuconychia, gynaecomastia, and asterixis
- Generate a prioritised differential diagnosis for liver disease using a three-question framework: acute vs chronic, hepatocellular vs cholestatic, aetiological cluster
- Apply the AST:ALT ratio and clinical pattern clustering to discriminate between alcoholic liver disease, viral hepatitis, obstructive jaundice, and rarer causes
INSTRUCTIONS
This is a skills-focused module. As you read, visualise performing the examination manoeuvres described and mentally rehearse the clinical reasoning process. The competency assessed here is SH (Skill and Habit) — you are expected to be able to perform these assessments fluently at the bedside, not merely describe them.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 328 — Approach to the Patient with Liver Disease (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 22 — Clinical Evaluation of Liver Disease (textbook)
- API Textbook of Medicine, 10th ed. — Clinical Approach to Jaundice (textbook)
- Macleod's Clinical Examination, 14th ed. — The Abdomen (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the junior doctor on the general medicine ward when a 44-year-old man named Arvind is admitted with jaundice and abdominal swelling. The referral note says only 'abnormal liver function tests.' Standing at the bedside, you have no investigation results yet — only the patient in front of you and the history he will give you. Within the next fifteen minutes you must elicit a history that distinguishes alcohol-related liver disease from viral hepatitis from a drug reaction from an obstructive cause; identify which features suggest chronicity rather than acuity; recognise signs that indicate imminent decompensation; and generate a prioritised differential diagnosis before you ever order a test. This is what clinical evaluation of liver disease means at the final-year level — not a list of signs to memorise, but a structured, purposeful examination that reads the liver's story from the patient's body.
WHY THIS MATTERS
The clinical evaluation — history and physical examination — remains the highest-yield investigation in hepatology, not any laboratory or imaging test. A carefully taken history will correctly identify the aetiology in over 60% of cases of liver disease before a single investigation is ordered. The physical examination identifies signs of chronic liver disease and portal hypertension that are both diagnostically informative and prognostically important. The NMC competencies IM5.8 and IM5.9 are at the SH (Skill and Habit) level — meaning that eliciting a liver disease history and performing a systematic examination are expected practical skills, not just knowledge items. IM5.10, generating a prioritised differential diagnosis from clinical features, is KH/SH — bridging knowledge and skill.
RECALL
Before proceeding, activate your knowledge of the relevant anatomy and physiology. The liver occupies the right hypochondrium and epigastrium; its inferior border normally lies at or just below the right costal margin in the mid-clavicular line; the span by percussion is 6–12 cm (dull to percussion across the liver). The portal vein drains blood from the spleen, stomach, and intestines into the hepatic sinusoids; portal hypertension at ≥12 mmHg (HVPG) drives the formation of portosystemic collaterals. The liver's synthetic function is reflected by albumin, INR, and glucose; its canalicular integrity by ALP and GGT; and its hepatocyte mass by ALT and AST. The reticuloendothelial system processes bilirubin, so haemolysis causes pre-hepatic jaundice while parenchymal and obstructive diseases cause direct hyperbilirubinaemia. Recall also the concept of acute versus chronic liver disease: chronic liver disease manifests physical signs (spider naevi, leuconychia, palmar erythema, caput medusae, splenomegaly) that develop over months to years and are absent in acute presentations.
Eliciting the Liver Disease History
The clinical indication for a thorough, structured liver disease history arises whenever a patient presents with jaundice, right upper quadrant pain or discomfort, abdominal swelling (ascites), unexplained fatigue, abnormal liver function tests discovered incidentally, or known risk factors for liver disease (alcohol use, viral hepatitis exposure, hepatotoxic drug use). The importance of getting the history right before ordering tests cannot be overstated: a complete hepatology history identifies the most likely aetiology, determines the urgency of investigation, and identifies potential reversible precipitants of decompensation.
The liver disease history must systematically cover six domains, each addressing a different potential aetiology:
1. Current clinical presentation: Onset and duration of symptoms — was the jaundice sudden (acute viral hepatitis, biliary obstruction, drug reaction) or gradual (chronic hepatitis, cirrhosis)? Is there pain — biliary colic (severe, episodic RUQ pain after fatty meals) suggests gallstone disease; dull RUQ ache suggests hepatomegaly or hepatic capsule distension; epigastric pain radiating to the back raises concern for pancreatitis (which may cause obstructive jaundice). Are there constitutional symptoms — fever suggests acute infection (viral hepatitis, ascending cholangitis, liver abscess); weight loss and anorexia are non-specific but concerning for malignancy or advanced cirrhosis. Is there pruritus — suggests cholestasis (bile salt retention); does it precede the jaundice (as in primary biliary cholangitis where itching can precede jaundice by years)? Is there altered consciousness — hepatic encephalopathy must be considered whenever confusion or behavioural change accompanies liver disease. Stool and urine colour changes: pale stools + dark urine = obstructive (conjugated) hyperbilirubinaemia; normal stool colour = pre-hepatic (unconjugated) or pure hepatocellular without cholestasis.
2. Alcohol history: This must be asked with explicit, non-judgemental questions. Quantify intake in standard drinks per day and per week; calculate the duration of drinking and pattern (daily vs binge). The CAGE questionnaire (Cut down/Annoyed/Guilty/Eye-opener) is a validated brief screening tool. A history of alcohol-related blackouts, withdrawal seizures, or previous alcohol-related hospital admissions points to significant dependency. The typical hepatotoxic threshold is approximately 20 g/day (2 standard drinks) in women and 40 g/day (4 standard drinks) in men sustained over years, though individual susceptibility varies. Indian unit conversion: one standard drink ≈ 14 g ethanol ≈ 30 mL of 40% spirits OR 300 mL of 5% beer.
3. Drug history (including herbal and traditional medicines): This is the most commonly underexplored domain in DILI. Ask explicitly about every prescribed drug, all over-the-counter medications (particularly paracetamol — the most common intrinsic hepatotoxin), anabolic steroids (common cause of cholestatic DILI in young males, bodybuilders), and especially Ayurvedic and traditional herbal preparations — patients often omit these because they perceive them as harmless. For each hepatotoxic drug suspect, establish the latency from drug start to symptom onset; whether the drug was stopped (dechallenge); and whether symptoms improved with stopping.
4. Viral hepatitis risk factors and vaccination history: Parenteral exposures — intravenous drug use (needle-sharing), blood transfusion before 1995 (pre-screening era in India), haemodialysis, tattooing/body piercing with unsterile equipment, healthcare worker needle-stick injuries. Sexual history — multiple partners, unprotected intercourse (HBV and to a lesser extent HCV are sexually transmitted). Perinatal history — maternal HBV carrier status (HBV vertical transmission). Household contacts with known hepatitis. Travel to or residence in endemic areas (HAV, HEV waterborne outbreaks). Vaccination history is critical — documented HBV vaccination (3-dose series) makes HBV transmission very unlikely; absence of HAV vaccination in a patient who has not had previous HAV infection increases risk.
5. Family history: Hereditary liver diseases require active consideration in younger patients or those without an obvious acquired cause. Ask about: Wilson disease (autosomal recessive copper overload — consanguinity, neuropsychiatric symptoms, haemolytic anaemia in siblings), hereditary haemochromatosis (autosomal recessive iron overload — diabetes, arthritis, skin pigmentation, cardiomyopathy in first-degree relatives), alpha-1 antitrypsin deficiency (lung disease + liver disease in the family), autoimmune hepatitis (female predominance, associated autoimmune conditions in family).
6. Sexual and social history: As noted under viral hepatitis risk factors; additionally, men who have sex with men (MSM) are at higher risk for HBV and HAV. Occupation may be relevant (healthcare workers, farmers with HEV risk from pig farming).
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
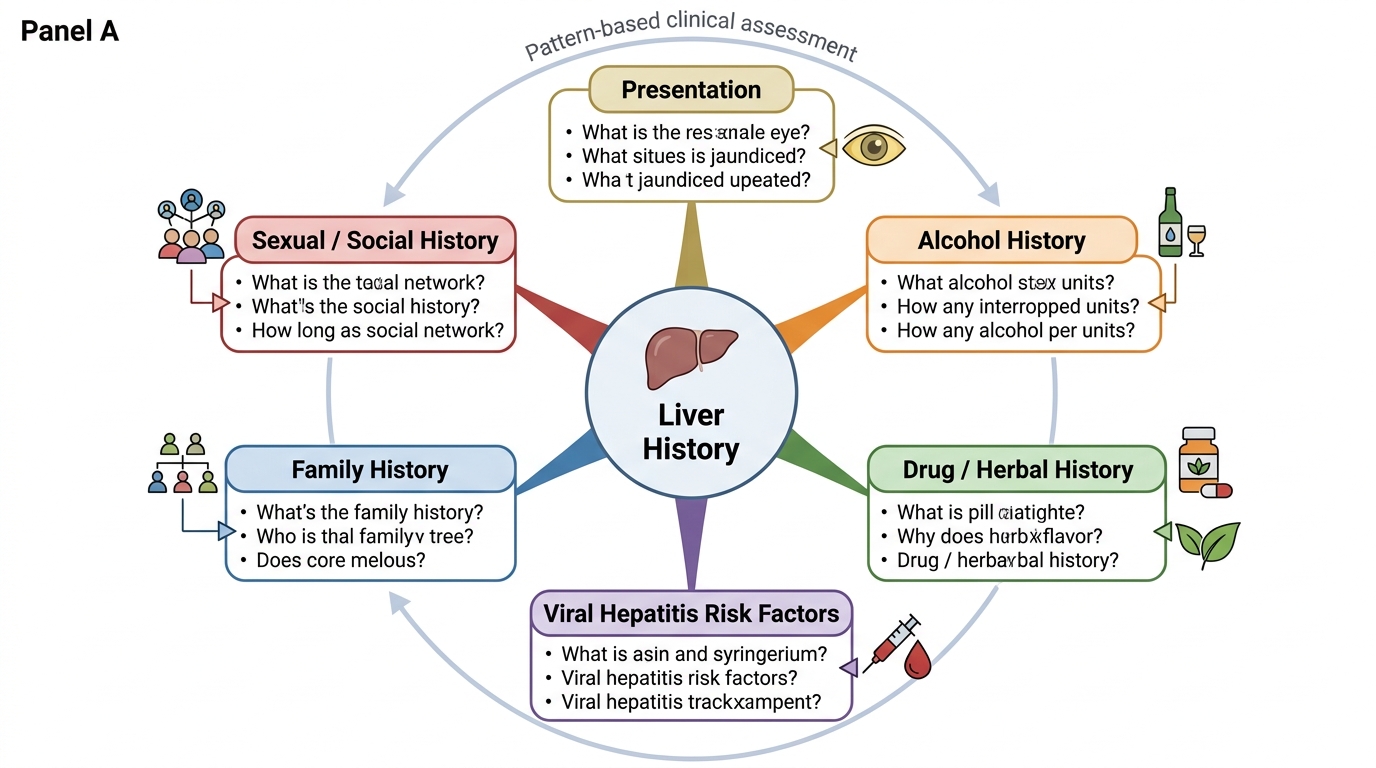
Structured Liver Disease History Framework
Governing Principles of Clinical Liver Assessment
Two governing principles underpin every clinical encounter with a patient with liver disease, and understanding them transforms the history and examination from a checklist activity into a purposeful diagnostic exercise. First, clinical evaluation in liver disease is inherently pattern-based: no single symptom, sign, or test result is pathognomonic; rather, it is the clustering of findings — a constellation of history elements, examination signs, and simple biochemical patterns — that produces a diagnostic gestalt. The skilled clinician recognises these constellations the way a physician recognises a face: not by analysing each feature in isolation, but by appraising the pattern as a whole. This means that the history and examination must be recorded completely, with positive and negative findings explicitly noted, so that the pattern can be evaluated in full rather than piece by piece.
The second governing principle is that liver disease has two fundamentally distinct presentations that require different clinical approaches: acute liver disease (in which the examination is likely to show only jaundice and tender hepatomegaly, because the chronic signs have not had time to develop) versus chronic liver disease (in which the examination is dominated by the signs of hepatic synthetic failure and portal hypertension — the cutaneous stigmata, splenomegaly, and ascites that develop over months to years of progressive disease). The distinction between acute and chronic is clinically crucial because it changes both the urgency of investigation (acute liver failure is a medical emergency with a specific management pathway) and the depth of the aetiological workup (chronic liver disease warrants a full screen for reversible causes even when the aetiology seems obvious).
A third operational principle governs the sequence of the clinical assessment: history before examination, examination before investigation. The history establishes the prior probability of specific aetiologies; the examination refines that probability by confirming or refuting the expected physical correlates; and only then should targeted investigations be ordered. In practice, investigations often run in parallel with clinical evaluation — but the mental model of sequential hypothesis-testing prevents the cognitive error of ordering a broad investigation panel before thinking, then using the results as a substitute for clinical reasoning. The clinician who first thinks 'what is most likely here, and what would I expect to find if I were right?' is far less likely to be misled by incidental abnormal results on an undirected panel.
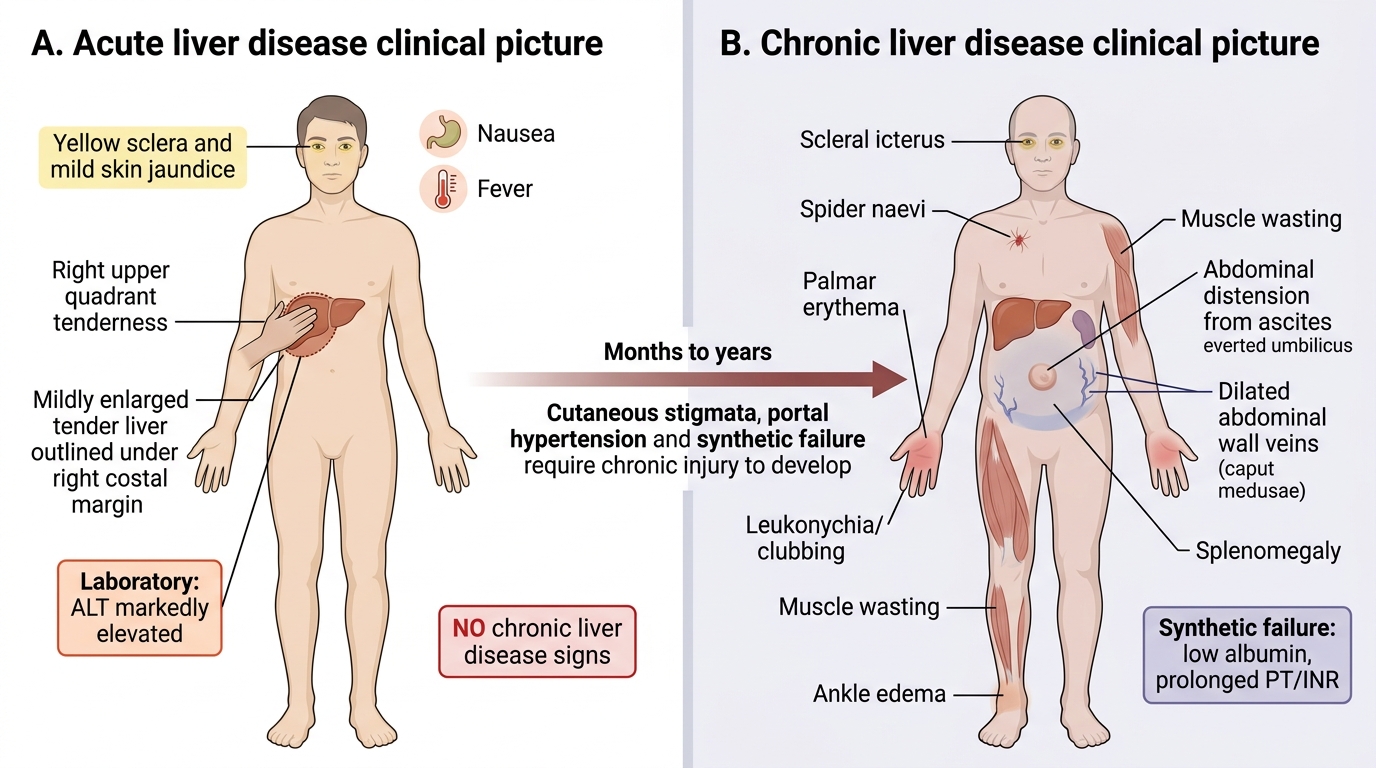
Acute vs Chronic Liver Disease: Clinical Picture
Systematic Physical Examination for Liver Disease
The physical examination of a patient with liver disease is a complete, head-to-toe assessment, not simply an abdominal examination. Many of the most diagnostically significant signs of chronic liver disease are found on the hands, face, chest wall, and skin — and they must be actively sought. A systematic approach ensures that no sign is missed. The examination follows the standard sequence: general observation → hands/nails → face → chest wall → abdomen → lower limbs. This structure is described below in the order you should follow at the bedside.
General observation: Before touching the patient, observe from the end of the bed. Is the patient jaundiced (icteric sclerae are the most sensitive visible indicator; skin jaundice is less sensitive)? Is there obvious abdominal distension (ascites — flanks are full, umbilicus is everted)? Is there muscle wasting (temporal, thenar, interosseous — sarcopenia in cirrhosis)? Is there asterixis (ask the patient to extend arms with hands dorsiflexed — the 'stop traffic' sign; involuntary flapping = hepatic encephalopathy grade II)?
Hands and nails: Examine in the following sequence:
- Leuconychia (white nails): associated with hypoalbuminaemia from cirrhosis; Terry's nails (distal brown band) also described.
- Clubbing of fingernails: occurs in cirrhosis, hepatopulmonary syndrome, and primary biliary cholangitis.
- Palmar erythema (erythema of the thenar and hypothenar eminences, sparing the central palm): caused by hyperoestrogenaemia due to failed hepatic oestrogen inactivation — a marker of chronic liver disease.
- Dupuytren's contracture (fibrosis of the palmar fascia causing ring/little finger flexion): associated with alcoholic liver disease (though also idiopathic and heritable).
- Flapping tremor (asterixis): as described — bilateral, arrhythmic, non-rhythmic brief lapses of wrist extension; may be detected at the hands.
Face: Inspect the sclerae for jaundice (yellow discolouration — scleral icterus is visible when bilirubin exceeds ~2.5–3 mg/dL). Look for parotid enlargement (bilateral painless enlargement in alcoholic liver disease and in Sjögren syndrome associated with primary biliary cholangitis). Inspect the periorbital skin for xanthelasma (yellow lipid deposits at the eyelid margins — associated with prolonged cholestasis and hypercholesterolaemia in PBC). Kayser-Fleischer rings (golden-brown deposits at the corneal periphery in Descemet's membrane — pathognomonic for Wilson disease when identified by slit-lamp examination).
Chest wall and trunk: Spider naevi (telangiectases): a central arteriole from which small vessels radiate, typically found in the distribution of the superior vena cava (chest wall above the nipple line, neck, arms, face). Present in up to 5 spider naevi in healthy individuals; >5 strongly suggests chronic liver disease. They represent cutaneous arteriovenous dilatations driven by elevated oestrogenic tone. Gynaecomastia (breast tissue development in males): also from hyperoestrogenaemia; bilateral, rubbery breast tissue. Loss of axillary and pubic hair (hypogonadism from pituitary-gonadal axis disruption in cirrhosis).
Abdomen: Inspect first — visible dilated veins on the abdominal wall (caput medusae) running from the umbilicus outward indicate reversal of flow in the paraumbilical veins — a sign of portal hypertension; blood flow direction (away from umbilicus in portal hypertension) distinguishes it from inferior vena cava obstruction (blood flows upward to the thorax). Visible peristalsis suggests bowel obstruction. Then:
- Percussion: percuss for hepatic span in the mid-clavicular line (normal 6–12 cm; dullness above and below; if liver not palpable, percuss to map borders); percuss for shifting dullness — place patient supine, percuss from umbilicus outward to the flank; if dull, ask patient to roll toward the opposite side; if dullness shifts to the lower flank = shifting dullness = ascites (≥500 mL needed for clinical detection).
- Fluid thrill: ask an assistant to press vertically on the midline abdomen to prevent fat-wave transmission; flick one flank and feel for an impulse on the opposite flank — positive in large-volume ascites.
- Palpation: palpate the liver starting from the right iliac fossa moving upward; hepatomegaly = liver palpable below the right costal margin. Note the lower border texture — smooth suggests fatty liver, hepatitis, or congestive hepatomegaly; irregular/nodular suggests cirrhosis or metastatic disease. Tenderness in the right hypochondrium suggests acute hepatitis or cholecystitis. The spleen is normally not palpable — splenomegaly in the context of chronic liver disease indicates portal hypertension. Ballotte the kidneys for polycystic disease (associated with autosomal dominant polycystic kidney disease + liver cysts).
Lower limbs: Pitting oedema of the ankles and pretibial region: result of hypoalbuminaemia (reduced oncotic pressure) and sodium/water retention (RAAS activation) in cirrhosis. Distinguish from cardiac or renal oedema by examining the JVP and asking about dyspnoea. Muscle wasting of the quadriceps and calves = sarcopenia of cirrhosis. Look for peripheral neuropathy (loss of vibration sense, symmetrical glove-and-stocking sensory loss) in alcoholic liver disease (alcoholic peripheral neuropathy — thiamine and other B vitamin deficiency).
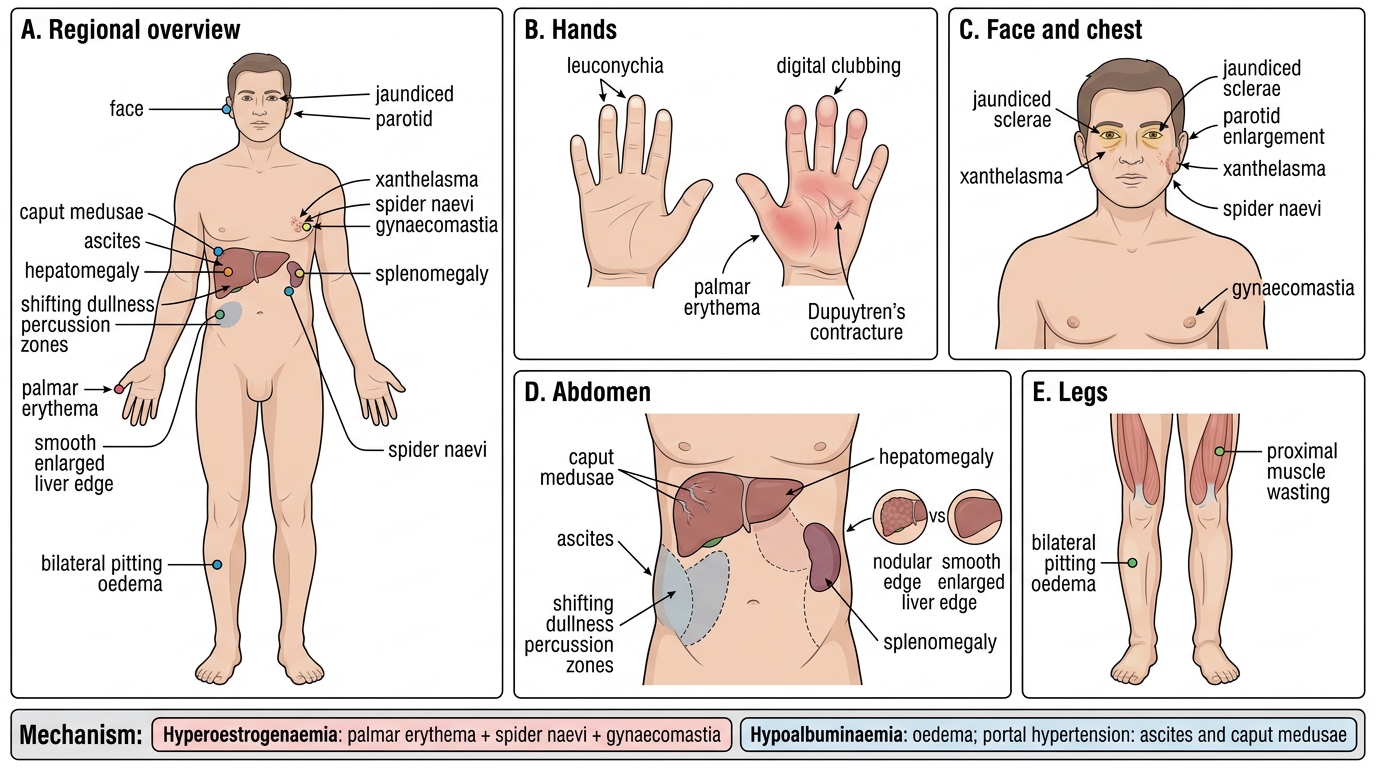
Physical Signs of Chronic Liver Disease
SELF-CHECK
A 42-year-old man with heavy alcohol use has palmar erythema, 6 spider naevi on his chest wall, and gynaecomastia. What is the unifying mechanism underlying all three of these signs?
A. Portal hypertension causing increased splanchnic blood flow
B. Hyperoestrogenaemia from impaired hepatic oestrogen metabolism
C. Hypoalbuminaemia causing peripheral vasodilatation
D. Kupffer cell activation releasing TNF-alpha
Reveal Answer
Answer: B. Hyperoestrogenaemia from impaired hepatic oestrogen metabolism
Palmar erythema, spider naevi, and gynaecomastia are all driven by the same mechanism: impaired hepatic inactivation of oestrogens in chronic liver disease leads to hyperoestrogenaemia. Elevated oestrogen causes peripheral arteriolar vasodilatation (palmar erythema and spider naevi — the central arteriole of a spider naevus is a dilated arteriole) and stimulates breast glandular tissue (gynaecomastia). Portal hypertension causes variceal formation and ascites but not these cutaneous signs. Hypoalbuminaemia causes oedema. TNF-alpha is relevant to alcoholic hepatitis pathogenesis but not these cutaneous signs.