Page 6 of 19
IM5.8-10 | Liver Disease Clinical Evaluation — SDL Guide (Part 2)
Interpreting Findings and Generating a Differential Diagnosis
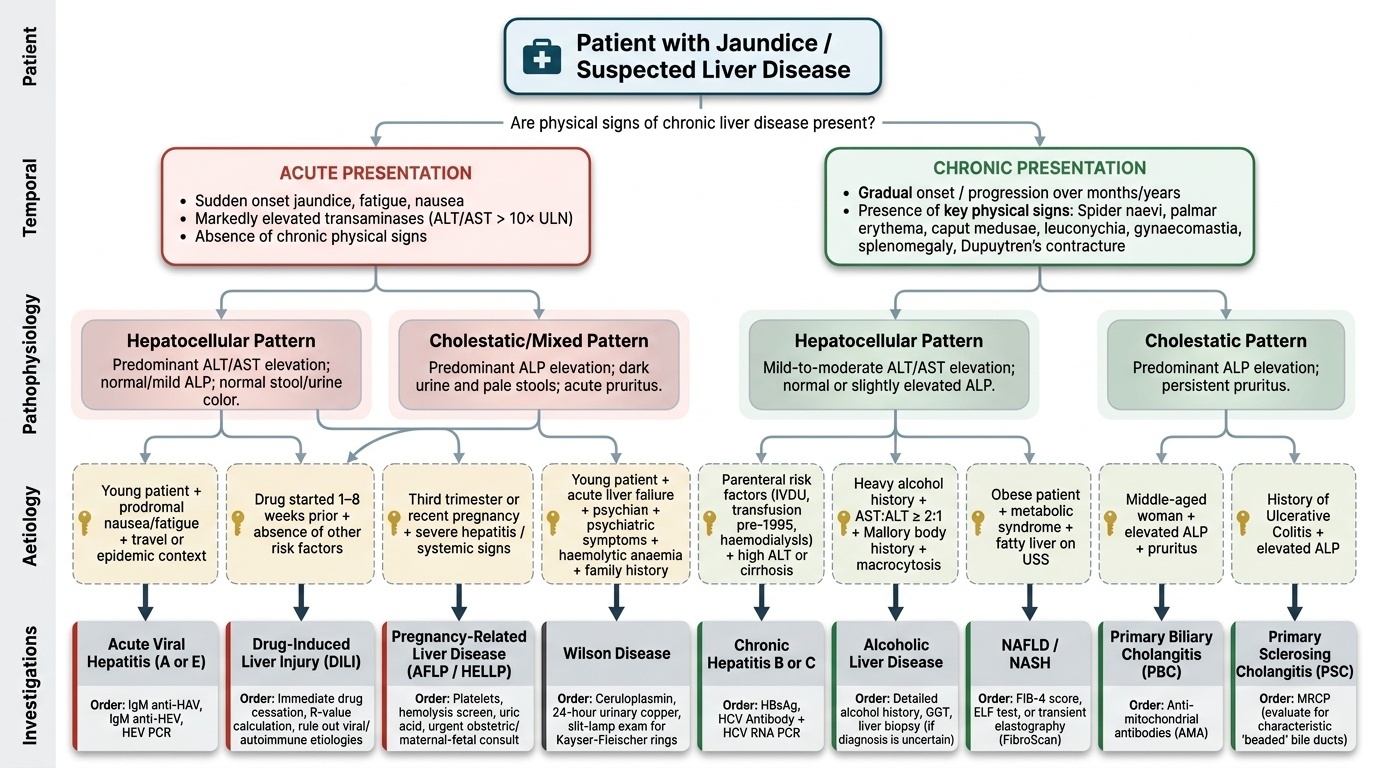
Generating a prioritised differential diagnosis for liver disease requires the clinician to integrate the clinical pattern from the history and examination into a structured shortlist, assigning probabilities based on the most informative discriminating features. This is not a mechanical process of listing all possible liver diseases; it is a Bayesian reasoning process in which some features dramatically raise or lower the probability of specific diagnoses. A clear framework is to ask three questions in sequence: (1) Is this acute or chronic? (2) Is the pattern hepatocellular or cholestatic? (3) What is the most likely aetiology given the epidemiological context and specific features?
Provided image
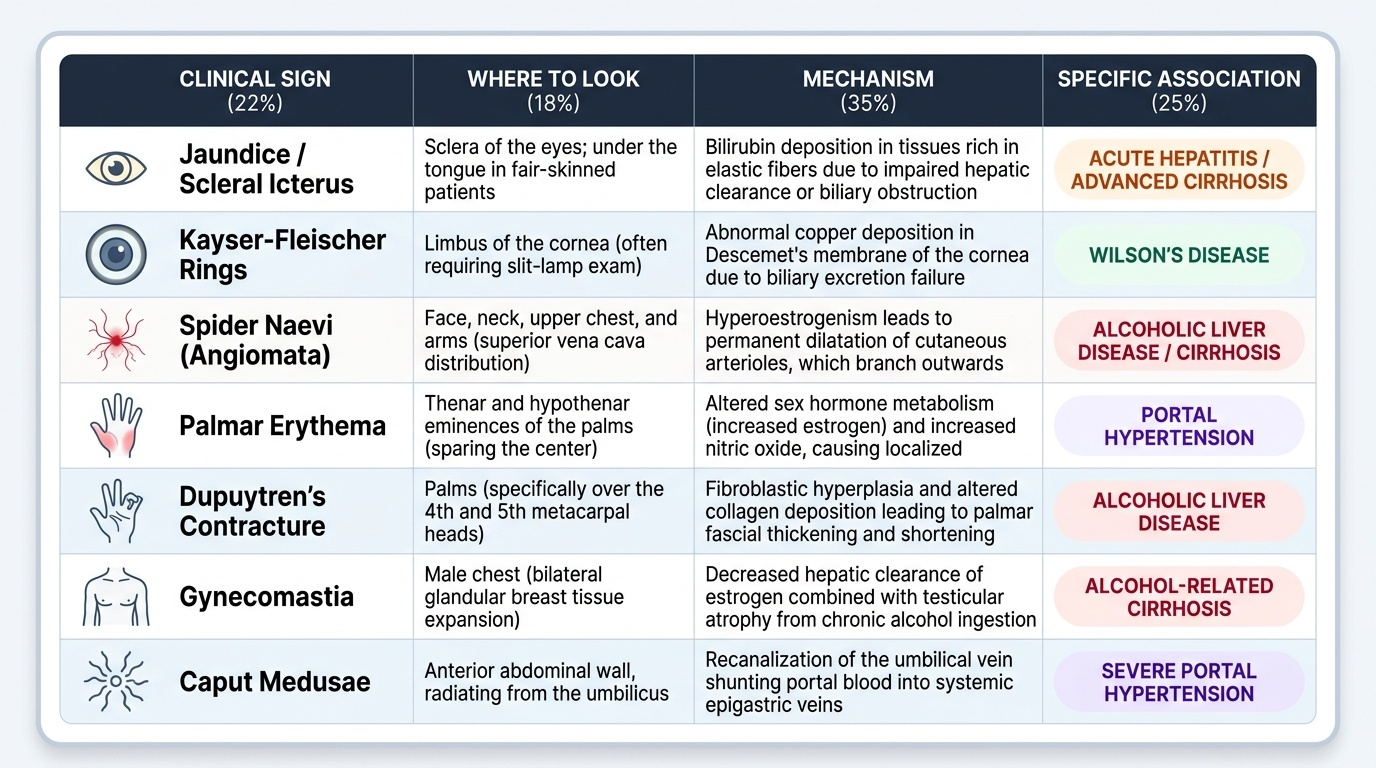
Acute vs chronic: Chronic liver disease is suggested by the presence of physical signs that develop over months to years — spider naevi, palmar erythema, caput medusae, leuconychia, gynaecomastia, splenomegaly, Dupuytren's contracture. These signs imply long-standing hepatic synthetic dysfunction and portal hypertension, and they argue against a purely acute presentation. In contrast, a previously well patient with sudden jaundice, nausea, profound fatigue, and markedly elevated ALT (>10× ULN) without any chronic liver disease signs suggests acute hepatitis — viral, drug-induced, or ischaemic.
Clinical feature clusters that point to specific aetiologies:
| Clinical pattern | Most likely diagnoses to consider |
|---|---|
| Young patient, acute jaundice, high ALT, prodromal nausea/fatigue, epidemic context or travel | Acute viral hepatitis A or E |
| Parenteral risk factors (IVDU, transfusion pre-1995, haemodialysis) + high ALT or cirrhosis | Chronic HBV or HCV |
| Heavy alcohol history + AST:ALT >2:1 + Mallory body history + macrocytosis | Alcoholic liver disease |
| Obese patient, metabolic syndrome, fatty liver on USS, gradual ALT elevation | NAFLD/NASH |
| Young patient, acute liver failure + psychiatric symptoms + haemolytic anaemia + family history | Wilson disease |
| Middle-aged woman + elevated ALP + positive AMA + pruritus | Primary biliary cholangitis |
| Ulcerative colitis history + elevated ALP + beaded bile ducts on MRCP | Primary sclerosing cholangitis |
| Drug started 1–8 weeks before jaundice + absence of other risk factors | Drug-induced liver injury (DILI) |
| Recent pregnancy or third trimester + severe hepatitis | Acute fatty liver of pregnancy / HELLP / HEV |
| RUQ pain + fever + jaundice (Charcot's triad) + elevated ALP | Ascending cholangitis from choledocholithiasis |
| Hepatomegaly + raised JVP + peripheral oedema | Congestive hepatopathy (right heart failure, Budd-Chiari) |
The prioritisation within the differential is guided by three principles: commonest first (in India: viral hepatitis B and C, alcoholic liver disease, and NAFLD account for >80% of chronic liver disease); most dangerous first (acute liver failure, ascending cholangitis, and hepatocellular carcinoma are time-critical); and most treatable first (Wilson disease, autoimmune hepatitis, biliary obstruction, and DILI are all potentially reversible with specific intervention, so they must not be missed).
The clinical pattern for each diagnosis should be committed to memory as a gestalt, not as an isolated sign. For example, alcoholic liver disease does not present merely with AST:ALT >2:1 — it presents with that ratio in a patient who has a quantified alcohol history, macrocytosis, parotid enlargement, Dupuytren's contracture, and possibly peripheral neuropathy. Every clinical sign corroborates or challenges the leading hypothesis; a good clinician reasons through a 'story' that fits all the findings, rather than anchoring on a single sign.
SELF-CHECK
A 50-year-old man presents with progressive jaundice over 6 weeks. He has pale stools, dark urine, and severe pruritus. Examination shows jaundice but no spider naevi, no caput medusae, no splenomegaly. Liver is slightly enlarged and smooth. ALP is 8× ULN; ALT is 2× ULN; bilirubin is 9 mg/dL (mainly direct). What is the most likely diagnostic category?
A. Acute viral hepatitis with intrahepatic cholestasis
B. Decompensated alcoholic cirrhosis with ascites
C. Extrahepatic biliary obstruction (cholestatic pattern without chronic liver disease signs)
D. Autoimmune hepatitis with hepatocellular predominance
Reveal Answer
Answer: C. Extrahepatic biliary obstruction (cholestatic pattern without chronic liver disease signs)
The pattern here is clearly cholestatic: predominantly elevated ALP (8× ULN), mild transaminase rise, conjugated (direct) hyperbilirubinaemia, pale stools, dark urine, and pruritus. The absence of any chronic liver disease signs (no spider naevi, no caput medusae, no splenomegaly) argues against established cirrhosis. Progressive obstructive jaundice over 6 weeks in a 50-year-old man raises concern for extrahepatic obstruction — pancreatic head carcinoma, cholangiocarcinoma, or choledocholithiasis. The next investigation is abdominal ultrasound (to check for bile duct dilatation). Acute viral hepatitis would show predominantly elevated transaminases (hepatocellular pattern). Decompensated cirrhosis would have chronic liver disease signs.
Applied Practice: Integrating History and Examination
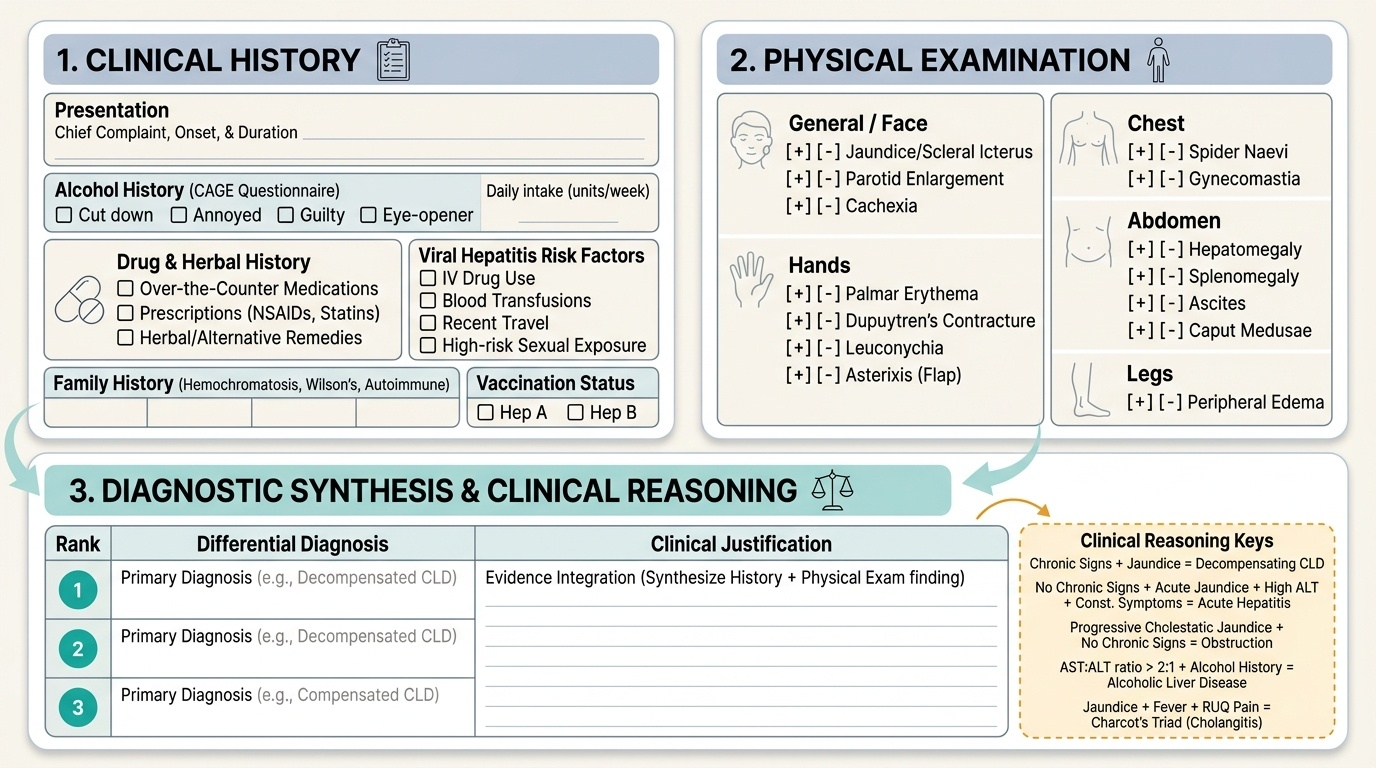
The integration of history and physical examination findings into a coherent clinical assessment is the practical expression of the IM5.8–5.10 competencies. In clinical practice, the history and examination are not performed in isolation — they are performed as an iterative, hypothesis-driven process in which findings from the history generate hypotheses that are confirmed or refined by the examination. For example, a history of heavy alcohol use makes you specifically look for palmar erythema, Dupuytren's contracture, parotid enlargement, and peripheral neuropathy — findings that would not be sought as urgently in a patient presenting with isolated jaundice without an alcohol history. Conversely, the presence of spider naevi and splenomegaly on examination refines a jaundiced patient's differential toward chronic liver disease, even if the history did not elicit an obvious cause.
Provided image
Key integration rules that summarise high-yield clinical reasoning for liver disease:
- Chronic liver disease signs (spider naevi, palmar erythema, caput medusae, splenomegaly, leuconychia, Dupuytren's) + jaundice = chronic liver disease decompensating — the workup targets aetiology of the underlying chronic disease plus precipitant of the acute decompensation.
- No chronic liver disease signs + acute jaundice + high ALT + constitutional symptoms = acute hepatitis — target viral serology and drug/herbal history.
- Progressive cholestatic jaundice (pale stools, dark urine, elevated ALP, pruritus) + no chronic liver disease signs = obstruction until proven otherwise — ultrasound for duct dilatation first.
- AST:ALT ratio >2:1 in a patient with heavy alcohol history = alcoholic liver disease — the ratio narrows the differential significantly (ratio <2 in viral hepatitis and NAFLD).
- Jaundice + fever + RUQ pain = Charcot's triad = ascending cholangitis — a time-sensitive diagnosis requiring urgent antibiotics and biliary decompression.
- Asterixis + confusion in a known cirrhotic = hepatic encephalopathy — look immediately for a precipitant (GI bleed, infection, dehydration, constipation, medication).
Documenting the history and examination in a structured liver disease format — aetiological risk factors enumerated, examination findings recorded positively and negatively for each category — ensures that nothing is missed and that the clinical assessment is reproducible and auditable. The value of a well-documented liver disease assessment extends beyond the initial consultation: it establishes a baseline against which future decompensation can be recognised and quantified.
Self-Assessment: Clinical Evaluation Scenarios
The following clinical scenarios are designed to test your ability to apply the structured history and examination framework to liver disease presentations, as required at the IM5.8–IM5.10 competency level. For each scenario, identify the key discriminating findings in the history and examination, generate a prioritised differential diagnosis, and state what single most important investigation you would order first. This mirrors the cognitive process expected in a final-year clinical examination or an OSCE station. Working through these scenarios actively — before reading the analysis — is far more valuable than passively reading the answers, because the learning goal is not to recognise the right answer among four options but to construct the reasoning chain from scratch, as you would at the bedside. Each scenario has been designed to include one or two high-yield discriminating features that narrow the differential, and the analysis explains why those features are pivotal. After completing all three scenarios, you should be able to identify the aetiology of common liver presentations from clinical features alone, with the investigation serving to confirm rather than to generate your hypothesis.
Provided image
Scenario A — History-taking emphasis: A 38-year-old man presents with jaundice and is asked about his history. He says he has been drinking 6–8 pegs of whisky daily for 8 years, his father also had liver problems, and he has been taking an Ayurvedic preparation for 'general health' for 3 months. He has no history of blood transfusion and has been vaccinated for hepatitis B. There is no travel history of note.
Assessment: Multiple aetiological risk factors are present. (1) Alcohol use at ~84–112 g ethanol/day for 8 years is well above the hepatotoxic threshold — alcoholic liver disease is the leading hypothesis. (2) Paternal liver disease raises hereditary liver disease (hereditary haemochromatosis, Wilson disease) — family history is positive. (3) Ayurvedic preparation could be causing DILI — drug history is positive. (4) HBV vaccination makes HBV less likely, but HCV risk factors are absent. Priorities: quantify alcohol, characterise Ayurvedic preparation and duration, ask about father's specific liver diagnosis. Examination focus: look for signs of chronic ALD (palmar erythema, Dupuytren's, parotid enlargement, peripheral neuropathy) and signs of haemochromatosis (skin pigmentation, arthropathy). First investigation: LFTs with AST:ALT ratio — if >2:1, supports ALD; RUCAM assessment for the Ayurvedic preparation; check iron studies (ferritin/transferrin saturation) for haemochromatosis.
Scenario B — Examination emphasis: A 58-year-old woman is referred with elevated ALP and bilirubin. On examination: icteric sclerae, xanthelasma, no spider naevi, no caput medusae, liver is smooth and enlarged, no splenomegaly, no ascites, no peripheral oedema. She is moderately itchy. No alcohol history, no relevant drug history.
Assessment: The examination pattern — cholestatic jaundice (xanthelasma from prolonged cholestasis + hypercholesterolaemia, pruritus, elevated ALP/bilirubin) without chronic liver disease signs or portal hypertension features — in a middle-aged woman with no obvious obstructive symptoms or alcohol history strongly suggests primary biliary cholangitis (PBC). Key confirmatory investigation: anti-mitochondrial antibody (AMA) — present in >95% of PBC cases. Secondary confirmation: serum ALP subtype (liver-specific ALP elevated in biliary disease). Ultrasound to exclude extrahepatic obstruction.
Scenario C — Differential diagnosis emphasis: A 26-year-old man presents with acute jaundice, confusion, haemolytic anaemia, and a serum caeruloplasmin of 12 mg/dL (low normal 20–40 mg/dL). His AST is 320 IU/L and ALT is 180 IU/L (AST:ALT >1.5). He has no alcohol history and no viral hepatitis risk factors.
Assessment: The combination of acute liver failure + haemolytic anaemia + neuropsychiatric symptoms + low caeruloplasmin in a young patient = Wilson disease until proven otherwise. Note the AST:ALT ratio >1.5 in a young patient without alcohol history should trigger Wilson disease consideration (Wilson disease can mimic alcoholic hepatitis biochemically). Diagnostic steps: serum caeruloplasmin + 24-hour urine copper + slit-lamp examination for Kayser-Fleischer rings. Liver biopsy for quantitative copper if diagnosis uncertain. Treatment: d-penicillamine or trientine (copper chelation); liver transplantation if acute liver failure.
CLINICAL PEARL
The AST:ALT ratio is one of the most clinically useful bedside calculations in hepatology — but only when the absolute values are elevated, because the ratio loses meaning at normal or near-normal levels. Ratio >2:1 in the context of heavy alcohol history = alcoholic liver disease (mitochondrial injury reduces ALT activity preferentially; pyridoxal-5'-phosphate depletion also preferentially reduces ALT). Ratio <2 in viral hepatitis — even HBV or HCV with cirrhosis — because viral injury causes balanced transaminase elevation. A ratio >3:1 with alcohol history makes viral hepatitis very unlikely. This single ratio can narrow a broad jaundice differential at the bedside before any serology is ordered.
A second pearl: do not let the absence of a detectable liver edge on palpation lead you to conclude no hepatomegaly. Percussion of the liver span (normal 6–12 cm in the mid-clavicular line) is mandatory — a cirrhotic, contracted liver may not be palpable below the costal margin yet the organ is abnormal. Conversely, a liver edge palpable 5–6 cm below the costal margin with a normal percussion span may be a Riedel's lobe (a normal anatomical variant of the right lobe) — not pathological hepatomegaly.