Page 5 of 23
IM6.7-8 | HIV Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit a structured history in a patient with suspected or confirmed HIV, including risk factors, mode of transmission, STI history, nutritional status, and OI risk factors
- Document and present a focused HIV history that helps delineate the aetiology of the current presentation
- Generate a differential diagnosis for common HIV-related presentations and prioritise based on clinical features and CD4 context
INSTRUCTIONS
Clinical evaluation of a patient with HIV demands a structured and sensitive approach that combines thorough history-taking, a system-directed physical examination, and symptom-to-diagnosis reasoning anchored in CD4 count context. This module addresses the skills-level competencies IM6.7 and IM6.8 — eliciting a complete HIV history and generating a prioritised differential diagnosis — at the SH (Skill in History-taking and clinical reasoning) level.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 197 — History and Physical Examination in HIV Disease (textbook)
- API Textbook of Medicine, 10th ed., Section 13 — HIV Clinical Assessment (textbook)
- NACO Operational Guidelines for ART Programmes, 2022 — Clinical Assessment at ART Centre (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the resident on call in the medicine ward at a district hospital. A 38-year-old man is brought in by his wife with a 10-day history of progressive confusion, headache, and one episode of seizure. His wife says he was treated for 'chest infection' three months ago at another hospital, and she found a strip of co-trimoxazole tablets in his bag. On your initial approach, you notice oral candidiasis, wasting, and bilateral cervical lymphadenopathy. You need to take a complete history, perform a focused examination, and generate a working differential — but you have 15 minutes before the senior consultant arrives. How you gather information in the next quarter-hour will determine whether this man receives the right diagnosis and the right treatment tonight. The clinical evaluation skills you build in this module are what separate a competent diagnostician from a pattern-matcher.
WHY THIS MATTERS
HIV history-taking is a distinct clinical skill that goes beyond routine medicine history. It requires probing sensitive domains — sexual history, injecting drug use, blood transfusions, occupational exposures — in a non-judgemental, empathic manner, while simultaneously building a clinical picture that localises the probable site of opportunistic infection and estimates the degree of immunosuppression. Under NACO guidelines, clinical assessment at ART centres follows a structured template covering mode of exposure, prior HIV testing, WHO staging features, OI history, nutritional status, and comorbidities. For the final-year MBBS student, the SH-level competency (IM6.7–6.8) means you must demonstrate the skill, not merely describe it — this module trains you to ask the right questions in the right sequence, interpret the clinical cluster, and generate a ranked differential before investigations are available.
RECALL
Before proceeding, recall the structure of a standard medical history — presenting complaint, history of present illness (OLDCARTS: Onset, Location, Duration, Character, Aggravating/Alleviating factors, Radiation, Timing, Severity), past medical history, drug history, family history, social history, and systems review. In HIV history-taking, each of these standard components is enriched with HIV-specific content. The CD4 count and WHO clinical stage determine the prior probability of specific diagnoses — recall from the foundations module that CD4 <200 cells/µL predisposes to PCP, Toxoplasma, and Cryptococcus; CD4 <100 carries risk of cryptococcal meningitis; CD4 <50 is the threshold for disseminated MAC and CMV retinitis. Your history should attempt to estimate the likely CD4 range before the result is available, using clinical and historical clues as a proxy.
Clinical Indication and Relevance of HIV History
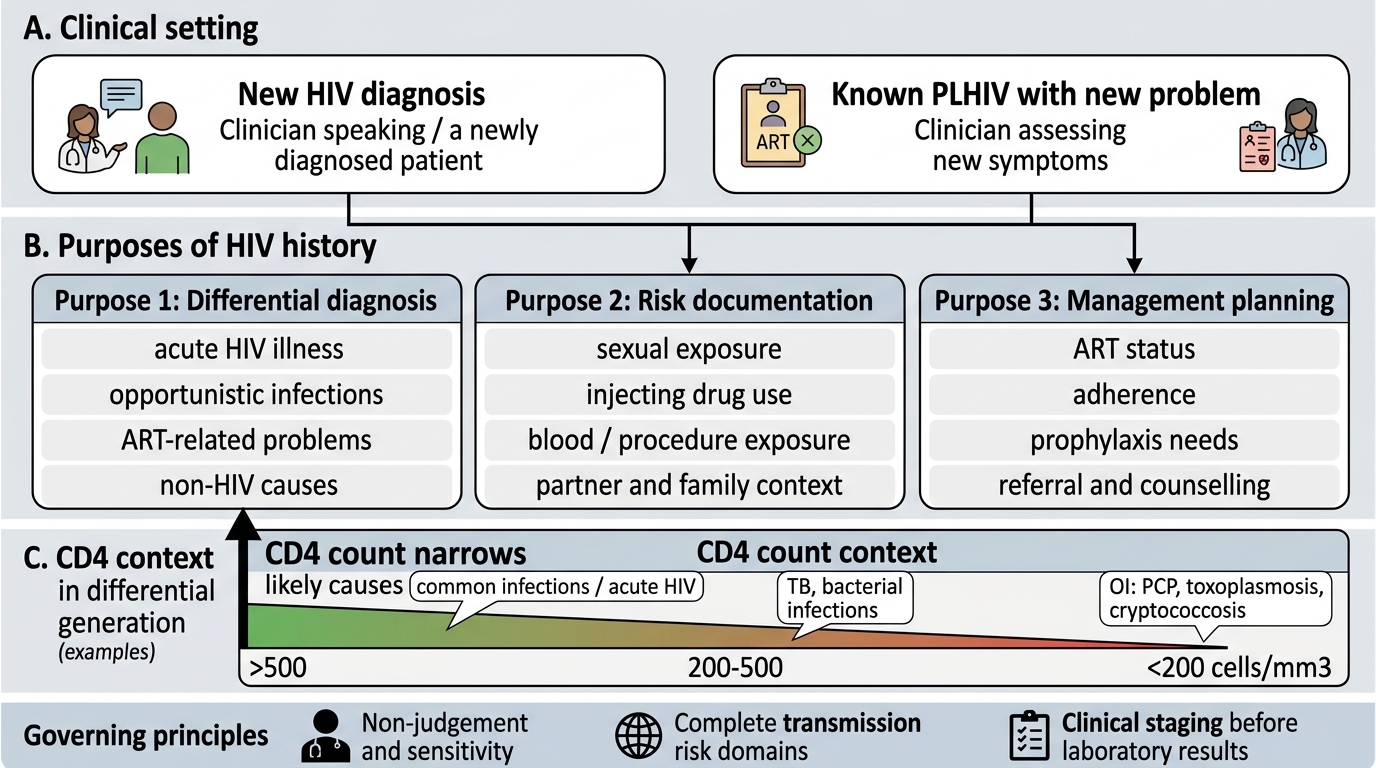
The HIV-focused history is indicated in two broad clinical settings: (1) first presentation for HIV testing or care — a newly diagnosed patient, a patient presenting for voluntary counselling and testing (VCT), or a patient in whom HIV is being considered as a new diagnosis; and (2) problem-oriented assessment of a known PLHIV — a patient already on the ART register who presents with a new symptom, OI complication, or treatment-related issue. The clinical indication for a thorough HIV history is essentially any patient with: unexplained prolonged fever, unexplained weight loss >10%, recurrent or severe infections, lymphadenopathy in multiple chains, oral candidiasis, oral hairy leucoplakia, unexplained cytopenias, herpes zoster in a young adult, or neurological symptoms in the presence of systemic illness. Additionally, provider-initiated testing and counselling (PITC) — the NACO recommendation that health providers should recommend HIV testing to all patients attending healthcare settings with conditions associated with HIV — means that HIV history and testing should be offered broadly, not only when the diagnosis seems obvious.
The relevance of a thorough history in the HIV context is threefold. First, the history directly informs the differential diagnosis — the specific presenting symptom combined with the estimated immune status generates a short list of likely diagnoses before investigations are ordered. Second, an accurate risk history documents the probable mode of transmission, informs partner notification, and guides public health responses. Third, thorough documentation of prior OIs, prior ART use, and adherence history informs current management — a patient who defaulted ART six months ago may have acquired resistance mutations that alter the choice of second-line regimen. The NACO clinical assessment form used at ART centres in India requires systematic documentation of all these elements.
Framework for HIV History-Taking
Governing Principles of HIV History-Taking
The HIV history is governed by three overarching principles that distinguish it from a standard medical history: non-judgement and sensitivity, completeness across all transmission risk domains, and systematic staging by clinical features before laboratory results. These principles operate simultaneously — the clinician must be thorough without being intrusive, sensitive without omitting essential information, and clinically analytical without losing sight of the whole patient.
Provided image
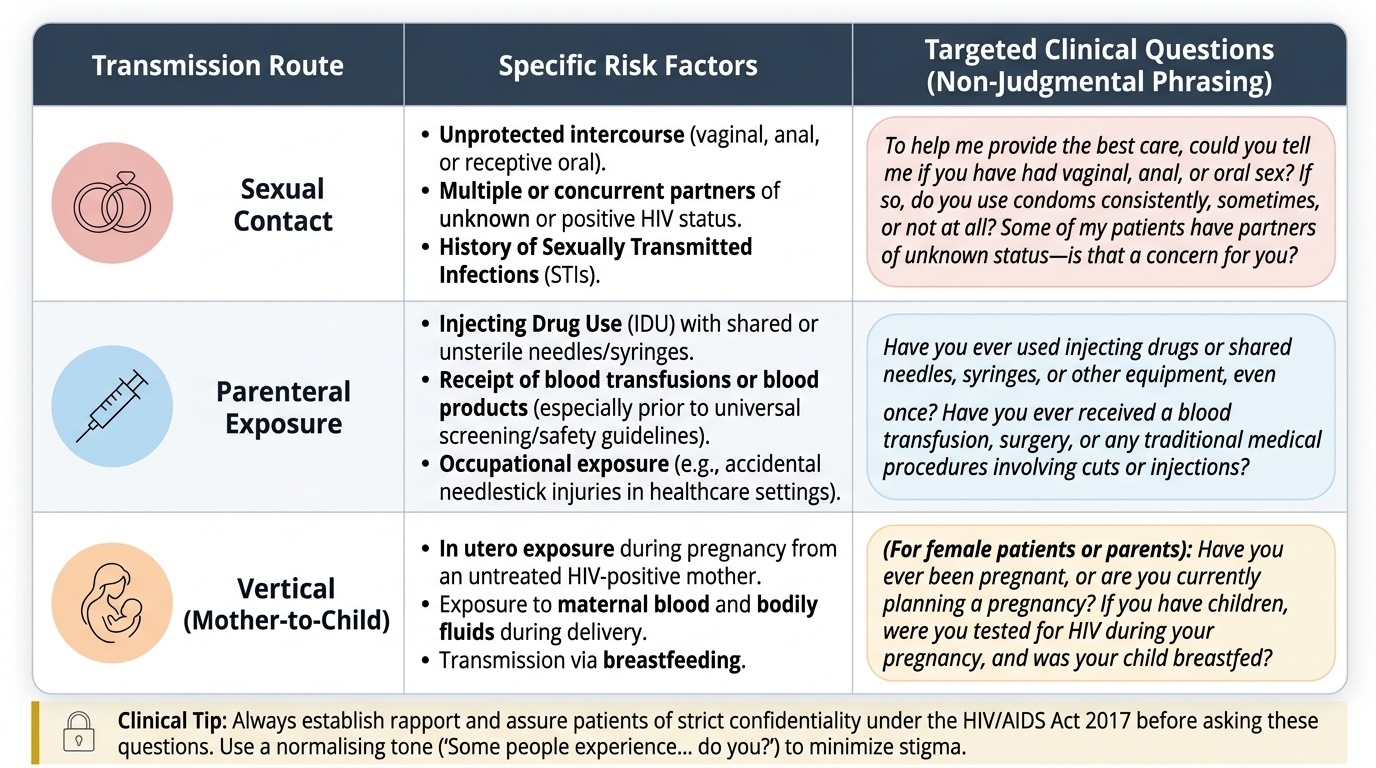
Non-judgement and sensitivity: Sexual history, injecting drug use, and other HIV risk behaviours are intensely personal and socially stigmatised in the Indian context. Patients who perceive that they will be judged or that their confidentiality will not be protected may withhold critical information. The clinician must establish rapport before asking sensitive questions, use neutral and normalising language ('Some people experience... do you?'), and assure confidentiality explicitly. Under NACO guidelines and the legal framework of HIV/AIDS Prevention and Control Act 2017 (India), patient confidentiality is legally protected; disclosure to third parties requires informed consent. A judgemental encounter does not merely fail the individual patient — it undermines trust in the entire healthcare system and contributes to delayed testing at the population level.
Completeness across all transmission risk domains: HIV is transmitted via four main routes: sexual contact (unprotected vaginal or anal intercourse with an infected partner); parenteral exposure (injecting drug use with shared needles; blood transfusions before universal screening; occupational needlestick injuries); vertical transmission (mother to child during pregnancy, delivery, or breastfeeding); and (rarely) organ transplantation. The history must explicitly probe each domain — it is not sufficient to assume a patient's mode of exposure based on appearance or social background.
Systematic staging by clinical features: The NACO clinical assessment template guides documentation of WHO staging features: weight loss, skin and mucosal lesions, lymphadenopathy, OI symptoms (respiratory, neurological, GI, ophthalmological), and functional status. This clinical staging forms the basis for treatment urgency and prophylaxis decisions before CD4 results are available.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
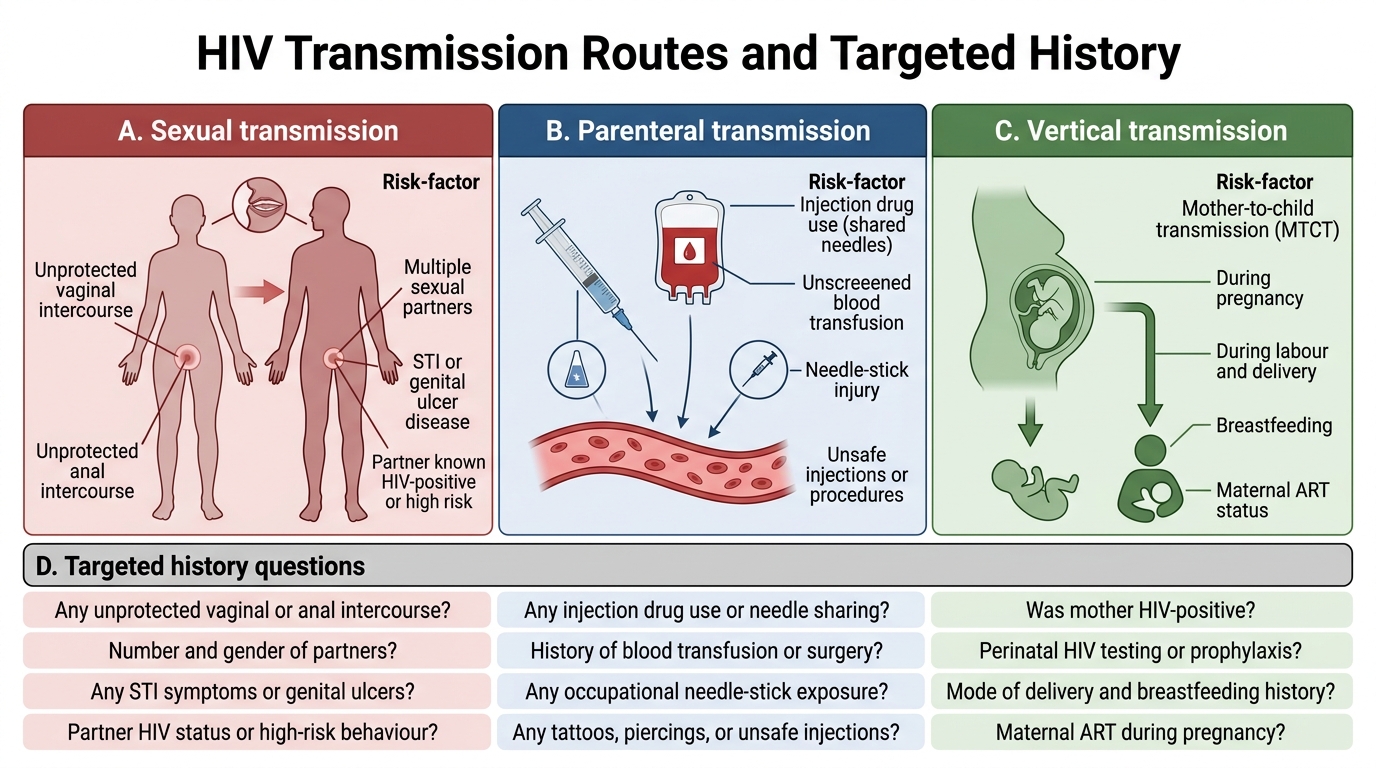
HIV Transmission Routes and Targeted History
The HIV History: Component-by-Component Technique
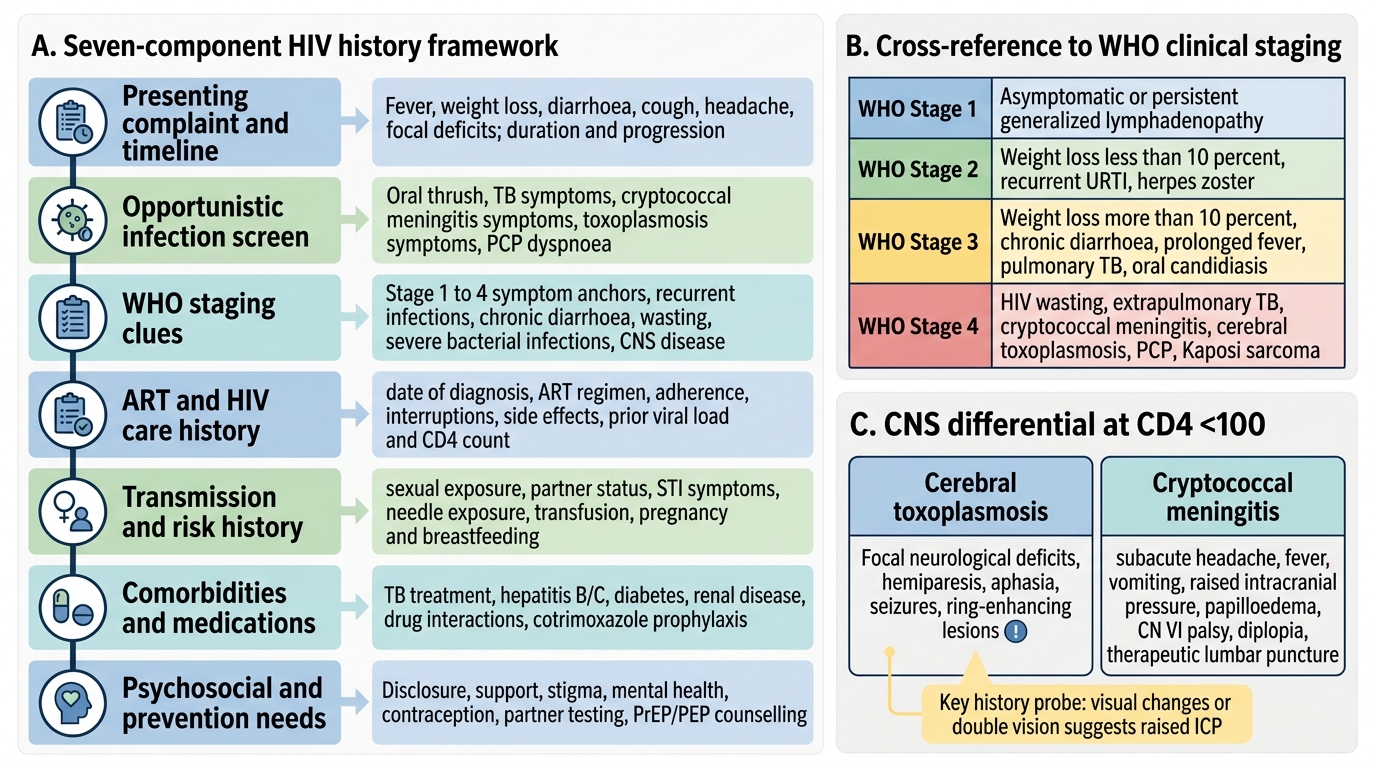
A complete HIV history proceeds systematically through the following components. Each component has standard history elements enriched with HIV-specific content. The goal is to elicit the information needed to stage the patient clinically, estimate immune status, generate a differential diagnosis for the presenting problem, and plan immediate management — all before laboratory results are available. Mastering this sequence is not a matter of rote memorisation but of understanding the clinical logic behind each question: why does knowing the date of HIV diagnosis matter (it tells you how long untreated immunosuppression has been accumulating), why does quantifying weight loss matter (>10% is WHO Stage 3 and mandates urgent investigation), and why does a history of prior OIs matter (recurrence of a treated OI suggests either inadequate treatment, drug resistance, or progressive immunosuppression). The structured format is a scaffold, but the skilled clinician adapts the order and depth of questioning based on the clinical urgency of the presentation.
1. Presenting complaint and history of present illness: Take the presenting complaint in the patient's own words, then characterise it fully using the standard OLDCARTS framework. For common HIV-presenting symptoms, specific additional questions are required:
- Respiratory symptoms (cough, dyspnoea): duration of onset — PCP has a subacute insidious onset over days to weeks (distinguishes it from typical bacterial pneumonia, which is acute); associated fever; exertional dyspnoea out of proportion to physical findings; sputum (absent in PCP, productive in bacterial or TB pneumonia).
- Neurological symptoms (headache, altered consciousness, seizures, focal deficit): duration; fever; any preceding OI or ART non-adherence; current CD4 estimate (headache + CD4 <100 = cryptococcal meningitis until proven otherwise; focal deficit + CD4 <100 = cerebral toxoplasmosis).
- Diarrhoea: Duration (>1 month = OI); blood in stool (Salmonella, Campylobacter, CMV colitis); watery voluminous without blood (Cryptosporidium, Microsporidiosis, Isospora); tenesmus.
- Constitutional symptoms: Weight loss (quantify in kg and %); fever — duration, pattern (PCP: sustained low-grade; MAC: high spiking); night sweats.
2. HIV-specific history elements:
- HIV diagnosis: Date of HIV diagnosis; mode of initial testing (VCT, PITC, antenatal); initial CD4 count and viral load if known; WHO staging at diagnosis.
- ART history: Current ART regimen; duration of therapy; adherence (estimate % doses taken, reason for missed doses); prior regimen changes and reason (toxicity, failure, simplification); prior resistance testing if done.
- OI history: Prior OIs — name, date, treatment received, outcome; history of TB (date, regimen, duration, completion); prior PCP, candidiasis, zoster; cryptosporidiosis or other diarrhoeal OIs.
- Prophylaxis history: Co-trimoxazole (current or past); IPT (isoniazid) — status and duration.
3. Sexual and transmission risk history:
- Sexual orientation and practices (non-judgemental framing); number of recent partners; consistent condom use; history of sexually transmitted infections (STIs — ulcers, discharge, dysuria); commercial sex work.
- Injecting drug use: substances, frequency, shared needle use.
- Blood transfusions: dates, indications (especially pre-1992 in India, before universal blood screening).
- Occupational exposure: healthcare worker (needlestick, mucous membrane exposure) — important for PEP history.
- Vertical transmission context (for women): Prior pregnancies and outcomes; HIV status of children; antenatal HIV testing history; PPTCT (Prevention of Parent-to-Child Transmission of HIV) — interventions received (ART during pregnancy, elective caesarean section, avoidance of breastfeeding, infant prophylaxis).
4. Past medical history: TB (dates, regimen); diabetes (immunosuppression, risk of TB and mucosal infections); hepatitis B and C co-infection (vertical transmission overlap; ART regimen selection — tenofovir active against HBV); liver disease; renal disease.
5. Drug history: Current ART regimen (note exact drug names — important for identifying DDIs); co-trimoxazole; fluconazole; any herbal or alternative medicines (risk of DDIs); drug allergies (critical — sulfa allergy affects co-trimoxazole and TMP-SMX use).
6. Social history and nutritional status: Occupation; family support system; nutritional history (anorexia, weight loss, estimate BMI); housing; food security (relevant for adherence and nutritional OIs); alcohol and recreational drug use; stigma and disclosure status (who knows about the diagnosis).
7. Functional status: WHO performance scale (0 = normal to 4 = bedridden >50% of waking hours) — correlates with WHO clinical stage and informs urgency of intervention.
Structured HIV History-Taking Framework
SELF-CHECK
During an HIV history, a 29-year-old woman with CD4 38 cells/µL reports 3 weeks of progressive headache, low-grade fever, and one episode of vomiting. She has minimal neck stiffness. Which question in the history of present illness would MOST help you distinguish cerebral toxoplasmosis from cryptococcal meningitis at this stage?
A. Is there any family history of neurological disease?
B. Have you noticed any visual changes or double vision (CN VI palsy) suggesting raised ICP?
C. Is the headache throbbing or constant?
D. Have you ever had a blood transfusion?
Reveal Answer
Answer: B. Have you noticed any visual changes or double vision (CN VI palsy) suggesting raised ICP?
At CD4 <100, the main differentials for meningitis/CNS disease are cerebral toxoplasmosis (focal neurological deficits — hemiparesis, aphasia, seizures) and cryptococcal meningitis (subacute meningitis with raised ICP — papilloedema, CN VI palsy, altered consciousness). Asking about visual changes and diplopia (CN VI palsy from raised ICP) specifically points toward cryptococcal meningitis with elevated ICP — a critical finding that changes immediate management (therapeutic LP). Toxoplasmosis more typically causes focal deficits (weakness, aphasia) rather than raised ICP signs. Headache character and family history do not help. Transfusion history is relevant to risk assessment but not to this differential.