Page 6 of 23
IM6.7-8 | HIV Clinical Evaluation — SDL Guide (Part 2)
Physical Examination in HIV: The Directed Approach
A focused physical examination in the HIV patient follows the presenting complaint but must always include a set of HIV-specific assessment elements regardless of the presenting problem, because new OIs and disease progression can be clinically silent. The examination aims to document: WHO staging indicators, evidence of specific OIs, nutritional status, functional capacity, and systemic complications of HIV or its treatment. The value of a thorough HIV examination extends beyond the presenting symptom — a patient who presents with diarrhoea may have unrecognised oral candidiasis that upgrades the WHO stage, or a retinal lesion that changes management priorities entirely. Every encounter is therefore an opportunity for a complete HIV staging examination, not merely a problem-focused review. In the district hospital setting where laboratory resources may be delayed, the examination findings — particularly SpO₂, fundoscopy, lymph node character, and oral cavity — may be the only data available to guide urgent decisions about investigations and empirical treatment. The systematic approach below ensures no high-yield finding is missed.
General appearance and vitals: Document weight (compare with prior records for weight loss trajectory), BMI, temperature (fever pattern, e.g. sustained in PCP, high spiking in MAC/TB), blood pressure, heart rate, and SpO₂ (hypoxia disproportionate to respiratory symptoms = PCP until proven otherwise). WHO performance scale should be estimated.
Head, eyes, ears, nose, throat (HEENT):
- Oral cavity: Inspect for oral candidiasis (white pseudomembranous plaques or erythematous patches — scrape to determine if removable); oral hairy leucoplakia (white lateral tongue streaks, non-removable); Kaposi sarcoma (violaceous lesions on hard palate); aphthous ulcers; angular cheilitis; gingivitis.
- Eyes: Fundoscopy for CMV retinitis in patients with CD4 <50 (characteristic 'pizza-pie' appearance — haemorrhages and exudates along vessels; 'scrambled eggs and ketchup' pattern); papiloedema (raised ICP in cryptococcal meningitis); cotton-wool spots (HIV microangiopathy or CMV).
- Sinuses: Tenderness (recurrent bacterial sinusitis, WHO Stage 2).
Lymph nodes: Persistent generalised lymphadenopathy (PGL) is defined as lymphadenopathy in two or more extra-inguinal sites lasting >3 months without an identifiable cause — it is a WHO Stage 1 feature. Assess size, consistency (soft-rubbery = reactive; firm-matted = TB lymphadenitis; hard = lymphoma), tenderness, and skin changes (fluctuance = suppurative TB lymphadenitis; overlying skin changes = atypical mycobacterial).
Respiratory: Auscultate for crackles (PCP: sparse crackles or clear chest early, despite profound hypoxia — the disproportionate hypoxia is the clue), bronchial breathing (TB consolidation), wheeze, or pleural rub. SpO₂ at rest and on exertion (a >3% desaturation on exertion suggests PCP even when resting SpO₂ is normal).
Neurological: Level of consciousness (GCS), meningism (Kernig and Brudzinski signs — note these may be negative in cryptococcal meningitis due to immune paresis), focal deficits (hemiparesis, aphasia, cranial nerve palsies), cerebellar signs, fundoscopy (papilloedema). Motor neurone signs (HIV myelopathy) vs peripheral sensory neuropathy (HIV or ART — NNRTI: efavirenz; d4T/ddI: now obsolete but still seen in legacy regimens — cause distal symmetric polyneuropathy).
Skin: Complete skin inspection for Kaposi sarcoma, molluscum contagiosum, pruritic papular eruption, seborrhoeic dermatitis, herpes zoster scars, and drug eruptions.
Abdomen: Hepatosplenomegaly (disseminated TB, MAC, lymphoma, viral hepatitis); tenderness (Cryptosporidium colitis, CMV colitis); masses.
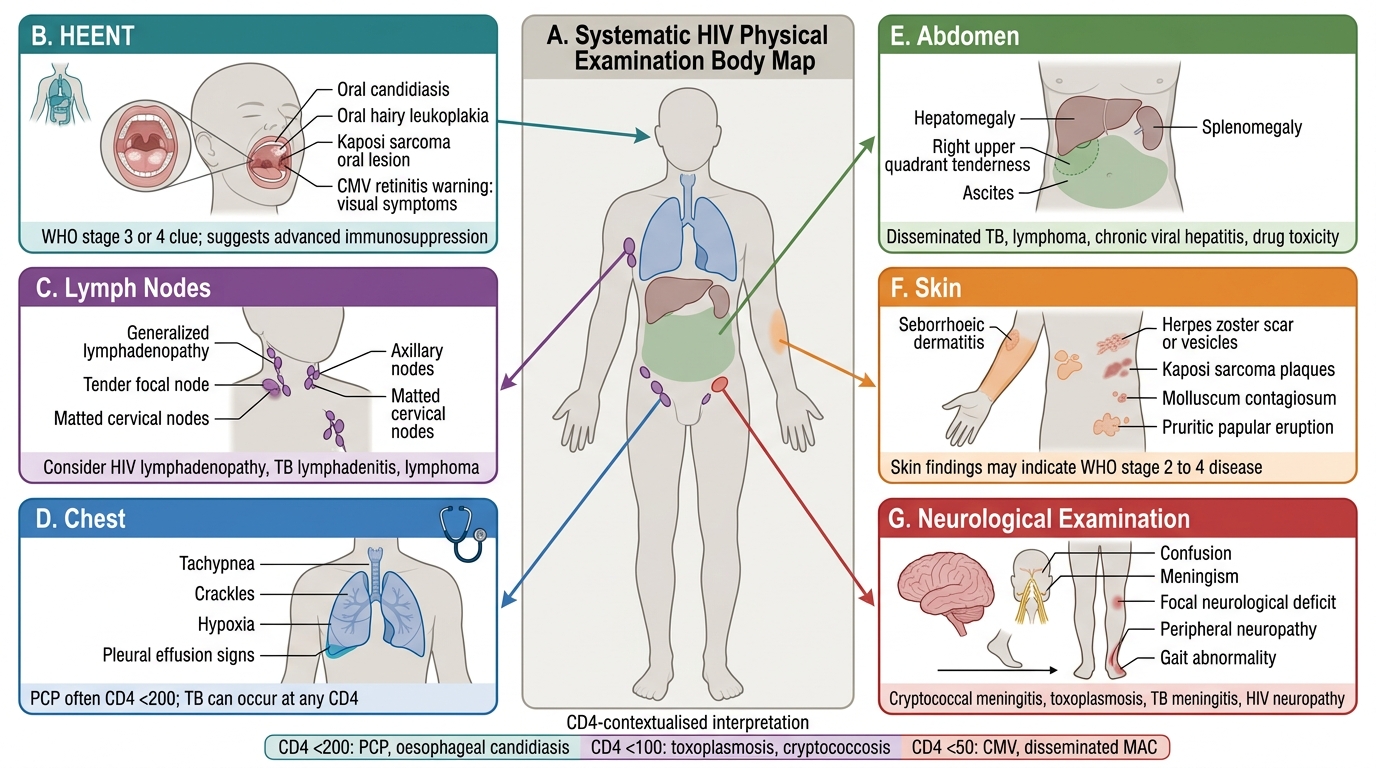
Systematic HIV Physical Examination Body Map
Generating the Differential Diagnosis: Symptom-CD4 Reasoning
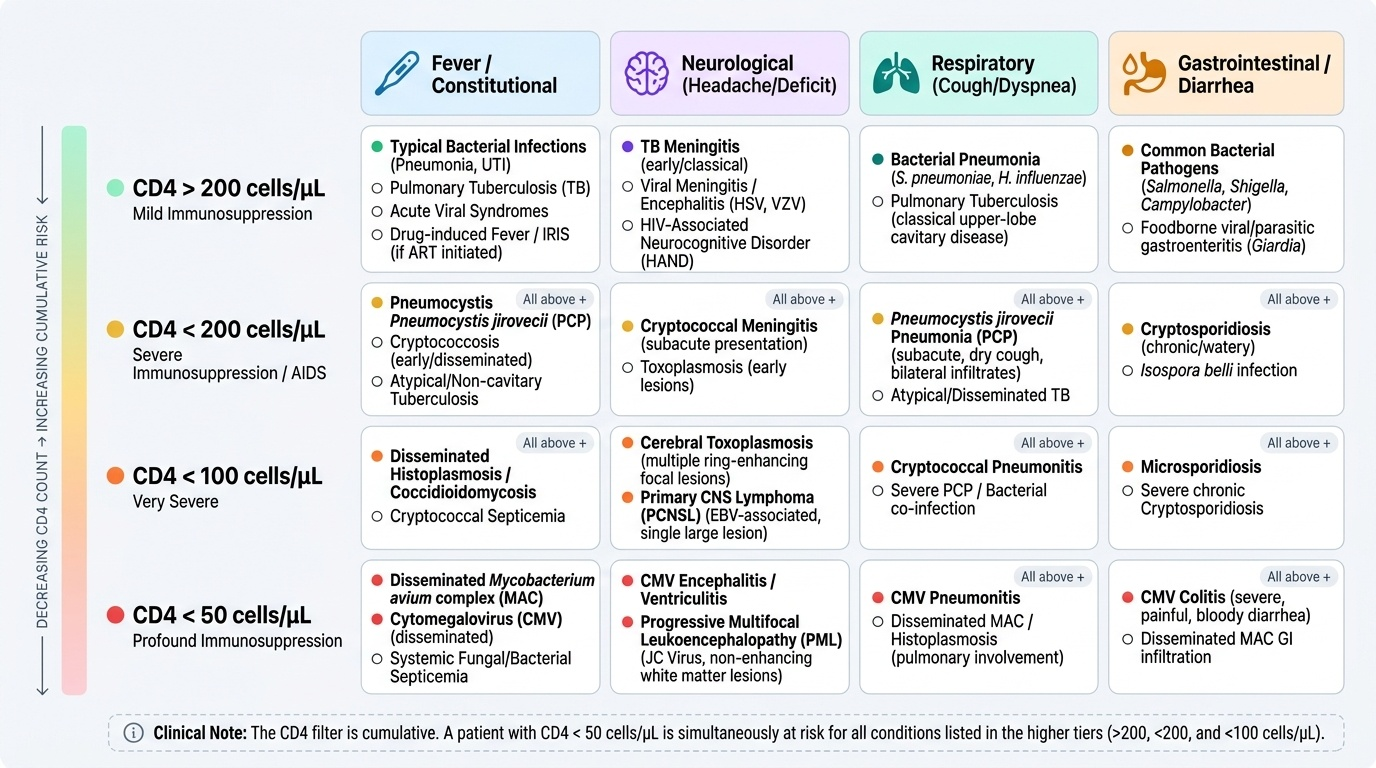
Generating a differential diagnosis in HIV requires integrating two sources of information: the clinical presentation (symptom complex, examination findings, disease course) and the immunological context (estimated or known CD4 count and WHO stage). The CD4 count functions as a prior probability modifier — it tells you which OIs are biologically possible at this level of immunosuppression and re-ranks a generic differential into an HIV-specific, CD4-contextualised list. A clinician who can mentally apply the CD4 threshold model to every presenting symptom is practising HIV medicine at the SH level.
Provided image
The practical approach to generating an HIV differential is a two-step process. Step 1 — Generate the generic differential for the presenting symptom using standard medical reasoning (e.g., 'subacute meningitis: bacterial, viral, TB, cryptococcal, lymphomatous, drug-induced'). Step 2 — Apply the CD4 filter to re-rank the list: conditions that occur predominantly at CD4 <100 move to the top in a patient with a CD4 in that range; conditions that are equally common in immunocompetent individuals remain in the differential but are contextually re-weighted.
Four high-yield HIV differential diagnosis frameworks for common presentations:
A. Fever in HIV:
- CD4 >200: Bacterial pneumonia, sinusitis, urinary tract infection, TB, drug fever, viral infections, IRIS (if recently started ART)
- CD4 <200: Above + PCP, Cryptococcus, atypical TB, Toxoplasma, Salmonella bacteraemia
- CD4 <50: Above + disseminated MAC (fever of unknown origin, anaemia, weight loss), disseminated CMV, fungaemia (Aspergillus, Histoplasma — geographic)
B. Neurological symptoms (headache, altered consciousness, focal deficit):
- CD4 <200: TB meningitis, viral encephalitis, HIV encephalopathy
- CD4 <100: Cryptococcal meningitis (subacute, raised ICP, minimal meningism), cerebral toxoplasmosis (focal deficit, multiple ring-enhancing lesions), primary CNS lymphoma (single large ring-enhancing lesion, EBV)
- CD4 <50: CMV encephalitis (periventricular enhancement), progressive multifocal leucoencephalopathy / PML (JC virus, white matter lesions)
C. Respiratory symptoms (dyspnoea, cough):
- CD4 >200: Bacterial pneumonia (acute, productive, lobar), TB (any stage, particularly risk)
- CD4 <200: PCP (subacute, insidious, bilateral ground-glass, elevated LDH), bacterial pneumonia, pulmonary TB (atypical CXR, miliary)
- CD4 <100: Pulmonary Kaposi sarcoma (nodular + pleural effusion), pulmonary MAC, pulmonary cryptococcosis
D. Diarrhoea:
- CD4 >200: Bacterial (Salmonella, Campylobacter, E. coli), viral gastroenteritis, drug-induced (ART side effect: lopinavir/r)
- CD4 <200: Cryptosporidium (watery, voluminous, no blood — 'rice water' diarrhoea reminiscent of cholera; resistant to most antibiotics), Isospora belli, Microsporidiosis, CMV colitis
- CD4 <50: Disseminated MAC (diarrhoea + systemic: fever, anaemia, hepatosplenomegaly, markedly elevated alkaline phosphatase)
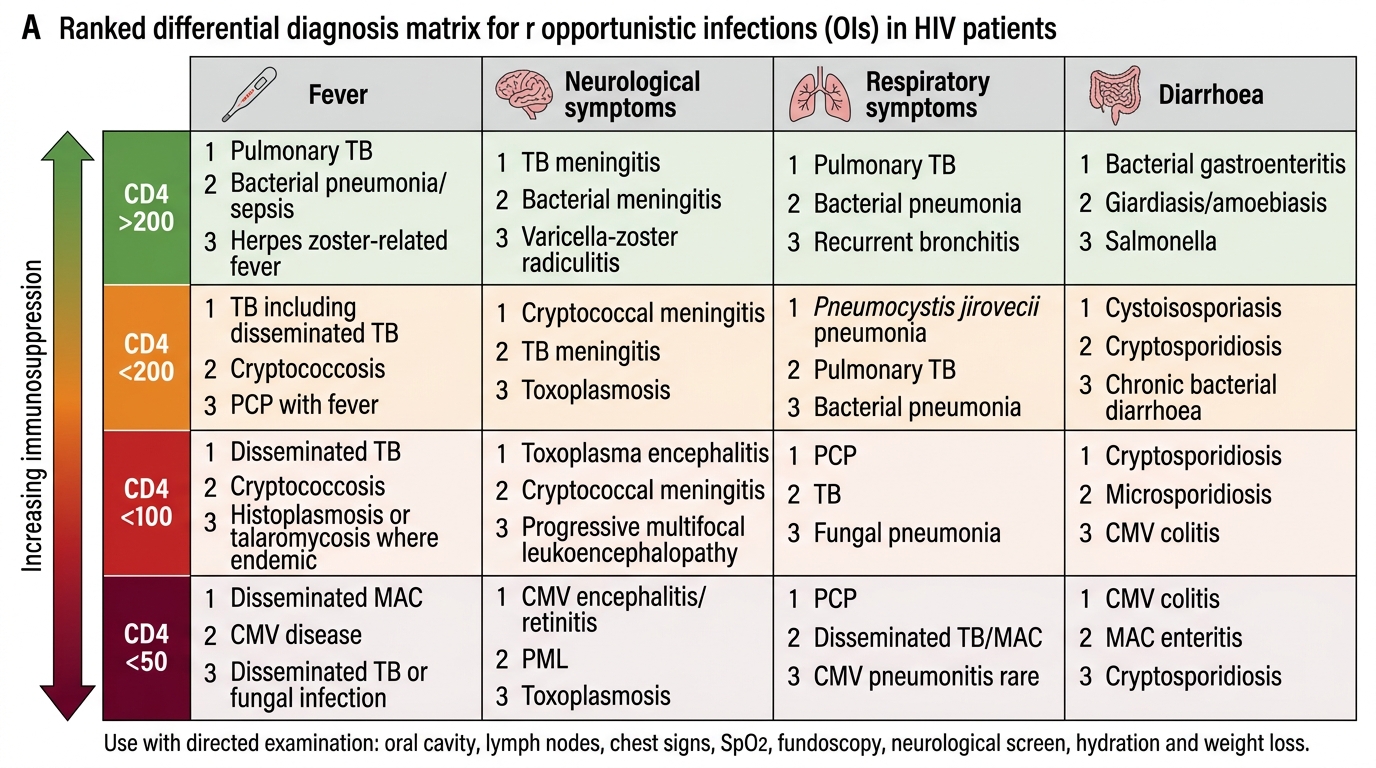
HIV Opportunistic Infection Differential by CD4 Count
SELF-CHECK
A 42-year-old known HIV patient on ART presents with 8 weeks of profuse watery diarrhoea (10–12 episodes/day), marked weight loss, and abdominal cramps. He has no blood in the stool. His CD4 count is 32 cells/µL. Stool culture for common bacteria is negative. Which organism tops the differential diagnosis?
A. Salmonella typhi
B. Entamoeba histolytica
C. Cryptosporidium parvum
D. Clostridium difficile
Reveal Answer
Answer: C. Cryptosporidium parvum
Cryptosporidium parvum is the leading cause of profuse, watery (secretory), non-bloody diarrhoea in HIV patients with CD4 <200 cells/µL — particularly at CD4 <50 as in this case. It causes voluminous rice-water-like diarrhoea without blood (unlike CMV colitis or Salmonella which can cause bloody diarrhoea). Standard stool bacterial cultures are negative. Diagnosis is by modified acid-fast stain or PCR of stool. Salmonella typhi causes typhoid fever with relative bradycardia and systemic features, not predominantly secretory diarrhoea. Amoebiasis causes bloody dysentery. C. difficile is associated with antibiotic use and causes bloody or non-bloody diarrhoea but is less characteristic at this CD4 level in the absence of recent antibiotics.
Applied Practice: The Structured HIV Consultation
The structured HIV consultation integrates history, examination, and differential diagnosis generation into a coherent clinical encounter. In the Indian district hospital or ART centre context, the consultation must be completed efficiently, often under time pressure, while maintaining sensitivity and accuracy. The following is the structured sequence that combines all the components into an applied clinical workflow.
Opening the consultation: Greet the patient by name, introduce yourself and your role, confirm confidentiality, and explain the purpose of the consultation. If a translator or family member is present, clarify who will receive information (patient's right to privacy vs family involvement) per the patient's preference. Confirm that the patient is comfortable and able to communicate.
Presenting complaint and system review: Begin with the patient's own words ('What brings you to the hospital today?'), then use focused questions to characterise the complaint fully. Simultaneously conduct a brief review of systems — asking about fever, weight loss, respiratory symptoms, neurological symptoms, skin or oral changes, and GI symptoms — to uncover additional OI clues that the patient may not have volunteered. Note that patients with profound immunosuppression may have blunted systemic symptoms — a low-grade fever with a CD4 of 30 can represent MAC or CMV disease, even though the patient reports feeling 'slightly unwell'.
ART adherence history: This is one of the most critical elements of the follow-up consultation. Use non-judgemental, open-ended framing: 'Taking HIV medicines every day can be very difficult — can you tell me how you've been managing?' Then probe for specific missed doses in the last week and last month (the '3-day recall' and '30-day recall'), reasons for missing (side effects, pill burden, stigma, pill unavailability, work schedule), and any periods of complete treatment interruption. Poor adherence is the single most common cause of virological failure and drug resistance acquisition.
Integrated documentation: After taking the history and completing the examination, document findings in the NACO-format clinical record, including: WHO stage at presentation, current ART regimen and adherence assessment, OI history, prophylaxis status, relevant comorbidities, and the differential diagnosis with the most likely diagnosis at the top. This document becomes the clinical basis for investigations ordered and treatment decisions made.
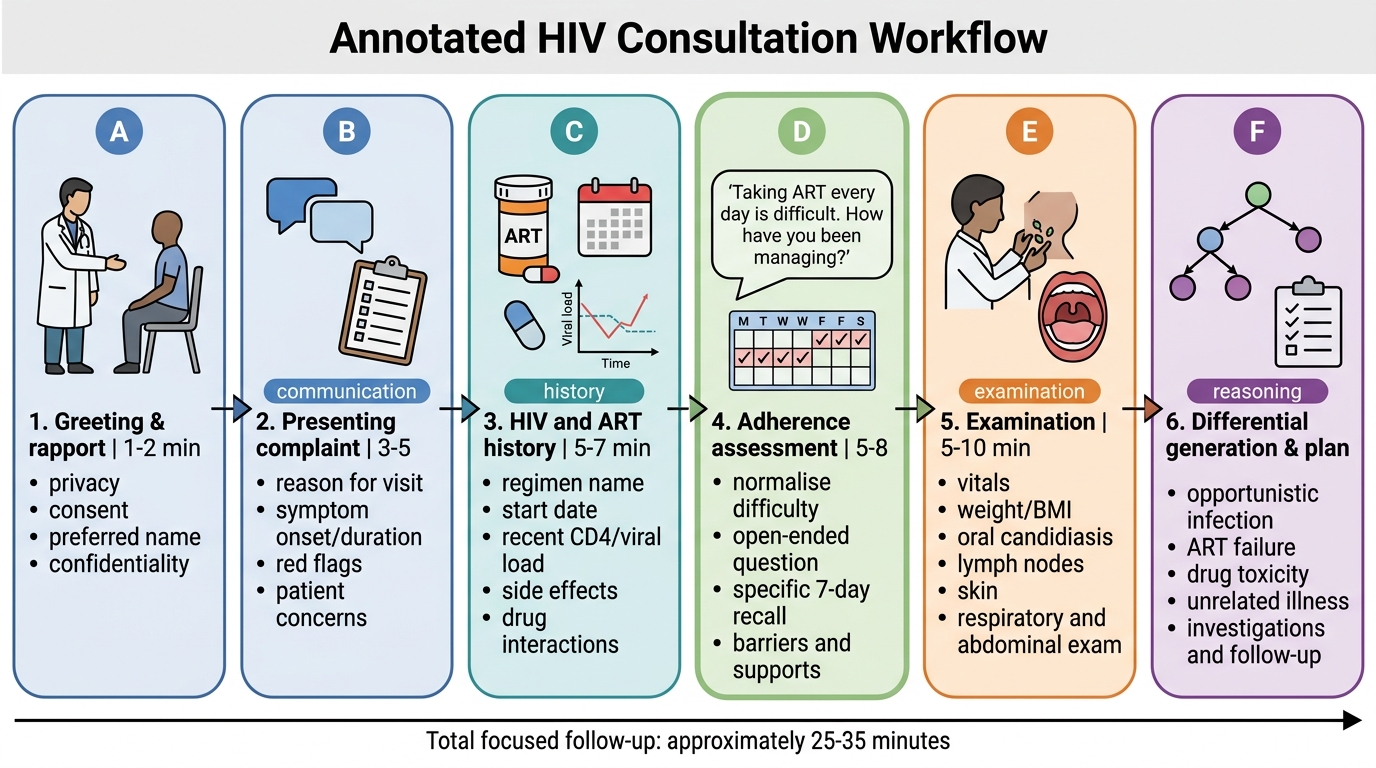
HIV Consultation Workflow
SELF-CHECK
A 31-year-old woman with HIV on ART for 2 years presents for a routine follow-up. You want to assess ART adherence. Which questioning approach is MOST likely to elicit accurate information about missed doses?
A. 'You've been taking your medicines every day, haven't you?'
B. 'Why did you miss your medicines last week?'
C. 'Taking HIV medicines every day is difficult. Can you tell me how you've been managing? Which days last week did you miss any dose?'
D. 'Your viral load is detectable — have you been non-compliant?'
Reveal Answer
Answer: C. 'Taking HIV medicines every day is difficult. Can you tell me how you've been managing? Which days last week did you miss any dose?'
Non-judgemental, normalising, open-ended framing ('Taking HIV medicines every day is difficult') reduces shame and defensiveness, increasing the likelihood that the patient will honestly disclose missed doses. This approach then transitions to specific recall questions ('which days last week') for accuracy. Option A is a leading question that implies the expected answer 'yes' and discourages disclosure of missed doses. Option B presupposes non-adherence, which is judgemental. Option D is accusatory and will almost certainly cause the patient to become defensive and withhold information, damaging the therapeutic relationship.