Page 1 of 23
IM6.1-6 | HIV Foundations and Opportunistic Disease — SDL Guide
Learning Objectives
- Describe the symptoms and signs of acute HIV seroconversion illness
- Define and classify HIV/AIDS using CDC criteria and WHO clinical staging
- Explain the relationship between CD4 count and risk of specific opportunistic infections
- Describe the pathogenesis, clinical features, and outcomes of common HIV-related opportunistic infections
- Describe the pathogenesis and clinical features of HIV-related malignancies
- Describe HIV-related skin and oral lesions and their diagnostic significance
INSTRUCTIONS
HIV/AIDS remains one of the most consequential infectious diseases in clinical medicine, demanding mastery of virology, immunology, and a broad spectrum of opportunistic infections. This module covers the natural history from acute seroconversion through AIDS-defining illness, the CD4-count threshold model that governs prophylaxis and treatment decisions, and the major opportunistic infections and malignancies that define advanced disease. The competencies addressed span knowledge and clinical reasoning at the KH (apply to scenarios) level.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 197 — Human Immunodeficiency Virus Disease (textbook)
- API Textbook of Medicine, 10th ed., Section 13 — HIV/AIDS (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 13 — HIV Infection (textbook)
- NACO — National AIDS Control Organisation, India: Operational Guidelines for ART Programmes, 2022 (guideline)
- WHO Clinical Staging of HIV Disease in Adults, 2007 (revised criteria) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rajan is 32 years old, a truck driver from Tamil Nadu, when he presents to a district hospital with two weeks of high-grade fever, sore throat, and a widespread maculopapular rash. He recalls a similar illness five years ago but recovered spontaneously. Today, examination reveals generalised lymphadenopathy, oral ulcers, and an erythematous rash on the trunk and palms. A monospot test is negative. He is worked up for typhoid, dengue, and secondary syphilis — all negative. Three days later, in the outpatient clinic, a colleague mentions that she saw a 26-year-old woman with Pneumocystis jirovecii pneumonia, bilateral interstitial infiltrates, and a CD4 count of 48 cells/µL, with no prior HIV diagnosis. Rajan's presentation and this woman's severe opportunistic infection sit at opposite ends of the same disease spectrum. Understanding HIV — from the moment of viral entry, through the immunological collapse that permits opportunistic infections, to the constellation of AIDS-defining illnesses — is not optional for any clinician practising in India today.
WHY THIS MATTERS
India has approximately 2.4 million people living with HIV (PLHIV), the third-largest burden globally, concentrated in high-prevalence states (Tamil Nadu, Maharashtra, Andhra Pradesh, Karnataka, Telangana, Manipur). NACO (National AIDS Control Organisation) coordinates the national response under the National AIDS Control Programme (NACP), providing free antiretroviral therapy (ART) to all diagnosed PLHIV regardless of CD4 count — a policy called 'Treat All.' For the final-year MBBS student, HIV/AIDS is tested in Medicine exit examinations, features in USMLE-style clinical reasoning questions, and demands competency at the KH (apply-to-scenarios) level: you must recognise acute seroconversion, interpret CD4 thresholds, diagnose opportunistic infections from clinical and laboratory clues, and apply prophylaxis and ART principles. Missed HIV diagnosis is a preventable cause of late-stage AIDS in India.
RECALL
Before proceeding, activate your prior knowledge. HIV (Human Immunodeficiency Virus) is an RNA retrovirus belonging to the Lentivirus genus, enveloped, with two types: HIV-1 (global, multiple clades/subtypes) and HIV-2 (predominantly West Africa, lower virulence, slower progression). The virus requires CD4+ T lymphocytes (also called T-helper cells), macrophages, and dendritic cells as host targets — all of which carry the CD4 receptor and a co-receptor (CCR5 or CXCR4) on their surface. Recall from basic immunology that CD4+ T cells are the orchestrators of adaptive immunity — they activate cytotoxic T cells, stimulate B-cell antibody production, and recruit macrophages. When HIV progressively depletes CD4+ T cells, the entire adaptive immune response collapses, leaving the patient vulnerable to infections and malignancies that healthy immunity would suppress. The normal CD4 count in adults is approximately 500–1500 cells/µL; an AIDS-defining level is below 200 cells/µL.
Acute HIV Seroconversion and Clinical Presentation
Acute HIV infection (also termed primary HIV infection or acute retroviral syndrome) occurs approximately 2–4 weeks after initial viral transmission. It is the period of intense viral replication before the host mounts an adaptive immune response, and it is characterised by very high plasma viral loads and a transient but sometimes dramatic dip in CD4 count. Recognising this syndrome is clinically vital because standard HIV antibody tests may still be negative at this stage — the so-called window period — while the patient is actually highly infectious, with viral loads sometimes exceeding 10⁷ copies/mL.
The clinical syndrome of acute seroconversion mimics infectious mononucleosis so closely that it is sometimes called a mononucleosis-like illness or flu-like illness. The cardinal features include: high-grade fever (present in >80% of cases), pharyngitis and sore throat, generalised maculopapular rash (characteristically affecting the trunk, face, and palms — a distinctive feature absent in classical glandular fever), profound fatigue, generalised lymphadenopathy, myalgia, arthralgia, and painful oral and genital ulcers. Neurological manifestations occur in a minority: aseptic meningitis, encephalitis, facial palsy, and peripheral neuropathy have all been described. Gastrointestinal symptoms — nausea, diarrhoea, and abdominal pain — are common. The illness typically lasts 2–4 weeks and resolves spontaneously, and most patients (60–80%) experience some or all of these features, though many never seek medical attention or are diagnosed with an intercurrent viral illness.
The diagnostic clue in Rajan's case is the combination of pharyngitis, generalised lymphadenopathy, oral ulcers, and a rash involving the palms — a pattern atypical for Epstein-Barr virus mononucleosis (which does not typically cause oral ulcers or palmar rash) and which should trigger HIV testing regardless of the stated risk history. The fourth-generation HIV Ag/Ab combination assay (detects both p24 antigen and anti-HIV antibodies) can detect infection 18–45 days after exposure and is the preferred initial test because it closes the window period significantly compared with second- or third-generation antibody-only tests. If the fourth-generation assay is negative but clinical suspicion is high, HIV RNA quantitative PCR (viral load) should be ordered, as it becomes detectable within 10–12 days of infection.
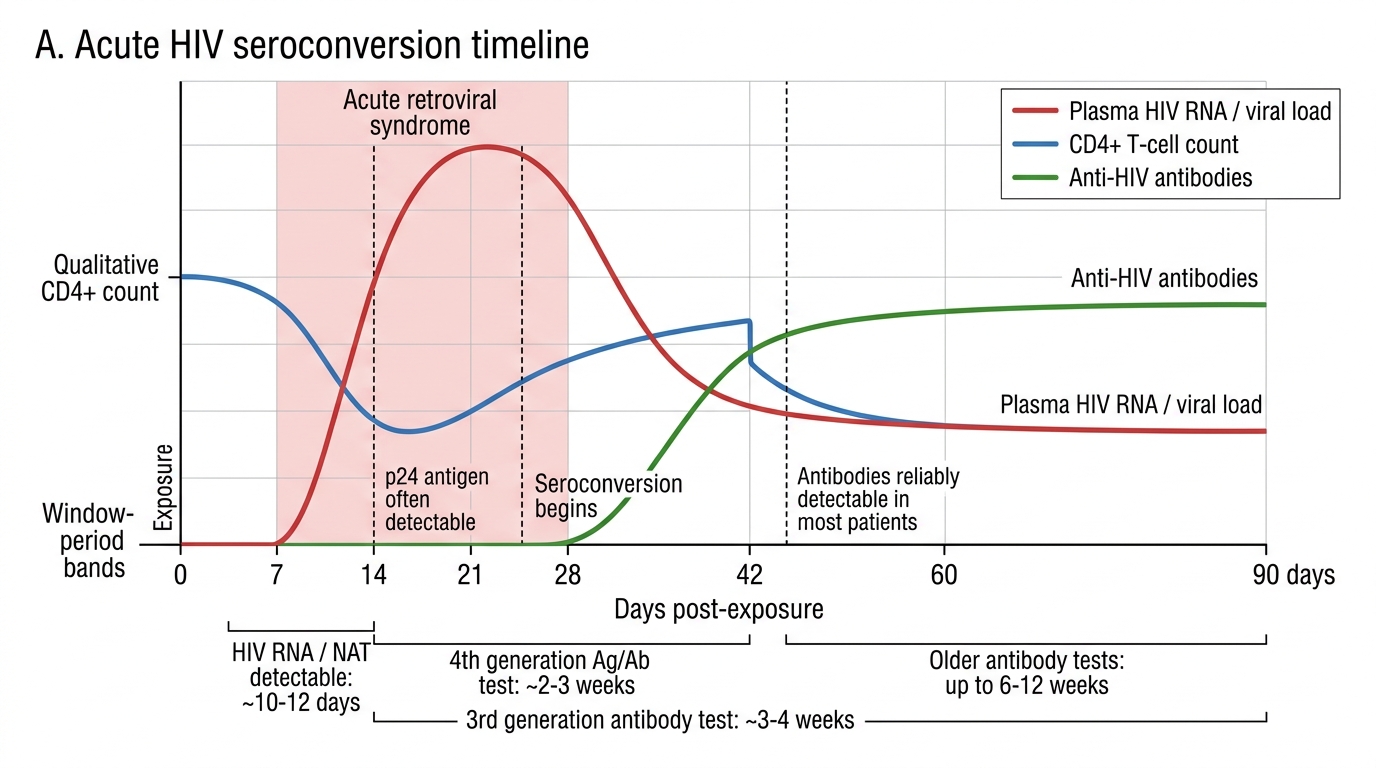
Acute HIV Seroconversion Timeline
After the acute illness resolves, the infection enters a clinical latency phase (also called asymptomatic HIV infection). Viral replication continues at lower levels in lymphoid tissue, CD4 cells are progressively depleted at an average rate of 50–100 cells/µL per year, and the viral load reaches a set point that predicts the pace of progression. This phase lasts an average of 8–10 years without ART; some individuals (termed long-term non-progressors or elite controllers) maintain normal CD4 counts for 20+ years without treatment, though this is rare. Without ART, most individuals progress to AIDS within a decade.
CDC Classification and WHO Clinical Staging of HIV/AIDS
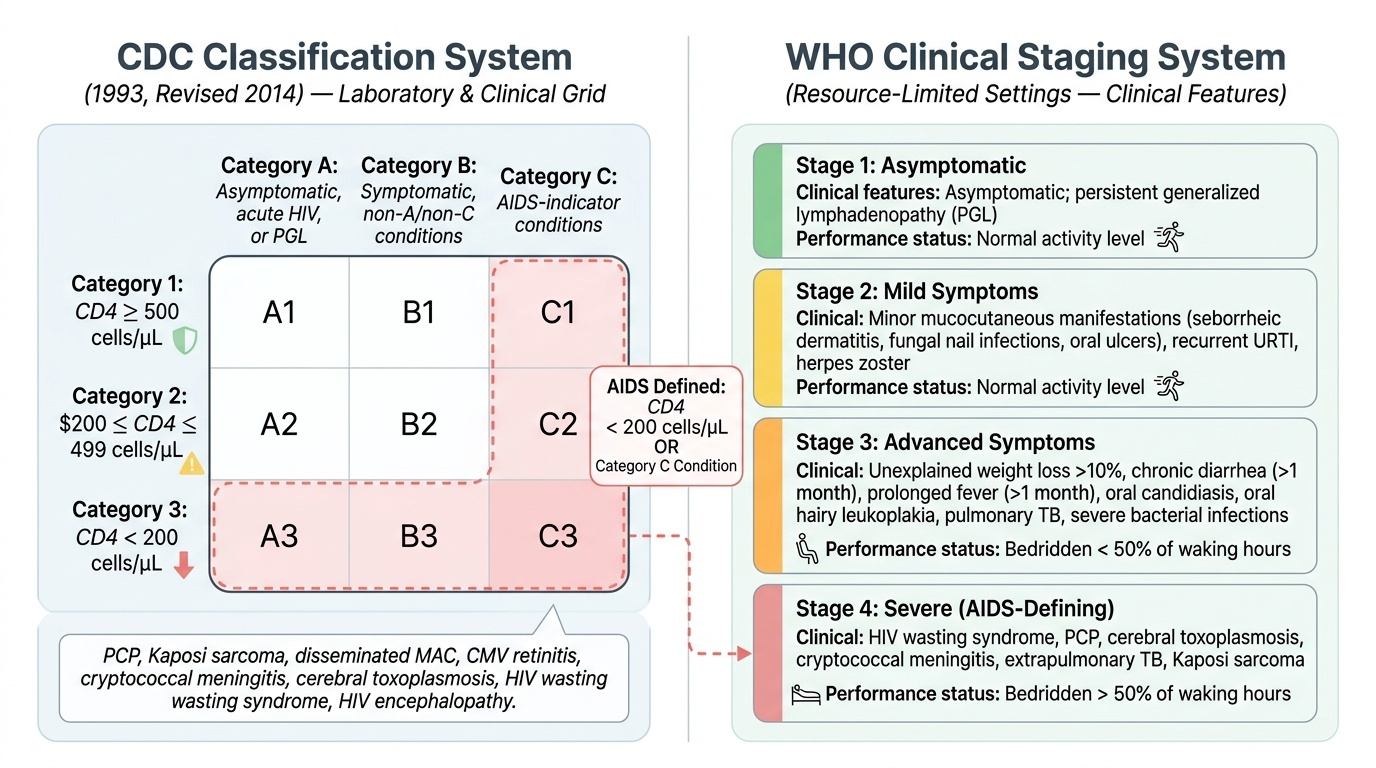
Two parallel classification systems are used internationally: the CDC (US Centers for Disease Control) classification system, which is laboratory-driven and is the standard for defining AIDS in research and epidemiological contexts; and the WHO Clinical Staging system, which is used in resource-limited settings where CD4 counting may not always be available and is applied across the NACO/NACP framework in India.
Provided image
CDC Classification (1993, revised 2014): The CDC system uses a 3×3 grid based on CD4 category (1: ≥500, 2: 200–499, 3: <200 cells/µL) and clinical category (A: asymptomatic/acute HIV/persistent generalised lymphadenopathy; B: symptomatic, not A or C; C: AIDS-indicator conditions). AIDS is defined by either a CD4 count <200 cells/µL (regardless of symptoms) OR the presence of any of the CDC Category C conditions (AIDS-defining illnesses) regardless of CD4 count. Category C includes 26 AIDS-defining conditions: Pneumocystis jirovecii pneumonia (PCP), Kaposi sarcoma, disseminated Mycobacterium avium complex (MAC), cytomegalovirus (CMV) retinitis, cryptococcal meningitis, cerebral toxoplasmosis, HIV wasting syndrome, HIV encephalopathy, recurrent bacterial pneumonia (≥2/year), and others.
WHO Clinical Staging (4 stages): The WHO system stages HIV disease based on clinical features alone:
- Stage 1: Asymptomatic; persistent generalised lymphadenopathy only. Performance scale: asymptomatic, normal activity.
- Stage 2: Minor mucocutaneous manifestations (seborrhoeic dermatitis, prurigo, fungal nail infections, oral ulcers, angular cheilitis), recurrent upper respiratory tract infections, herpes zoster. Performance: symptomatic, normal activity.
- Stage 3: Weight loss >10% body weight, unexplained chronic diarrhoea >1 month, unexplained prolonged fever >1 month, oral candidiasis (thrush), oral hairy leucoplakia, pulmonary TB, severe bacterial infections (pneumonia, pyomyositis). Performance: bedridden <50% of waking hours.
- Stage 4 (AIDS-defining): HIV wasting syndrome; Pneumocystis jirovecii pneumonia; cerebral toxoplasmosis; cryptococcal meningitis; disseminated non-tuberculous mycobacteria; CMV retinitis; extrapulmonary TB; Kaposi sarcoma; HIV encephalopathy; disseminated endemic mycosis (histoplasmosis, coccidioidomycosis); recurrent Salmonella septicaemia; Cryptosporidium chronic diarrhoea >1 month; invasive cervical cancer; disseminated herpes simplex. Performance: bedridden >50% of waking hours in last month.
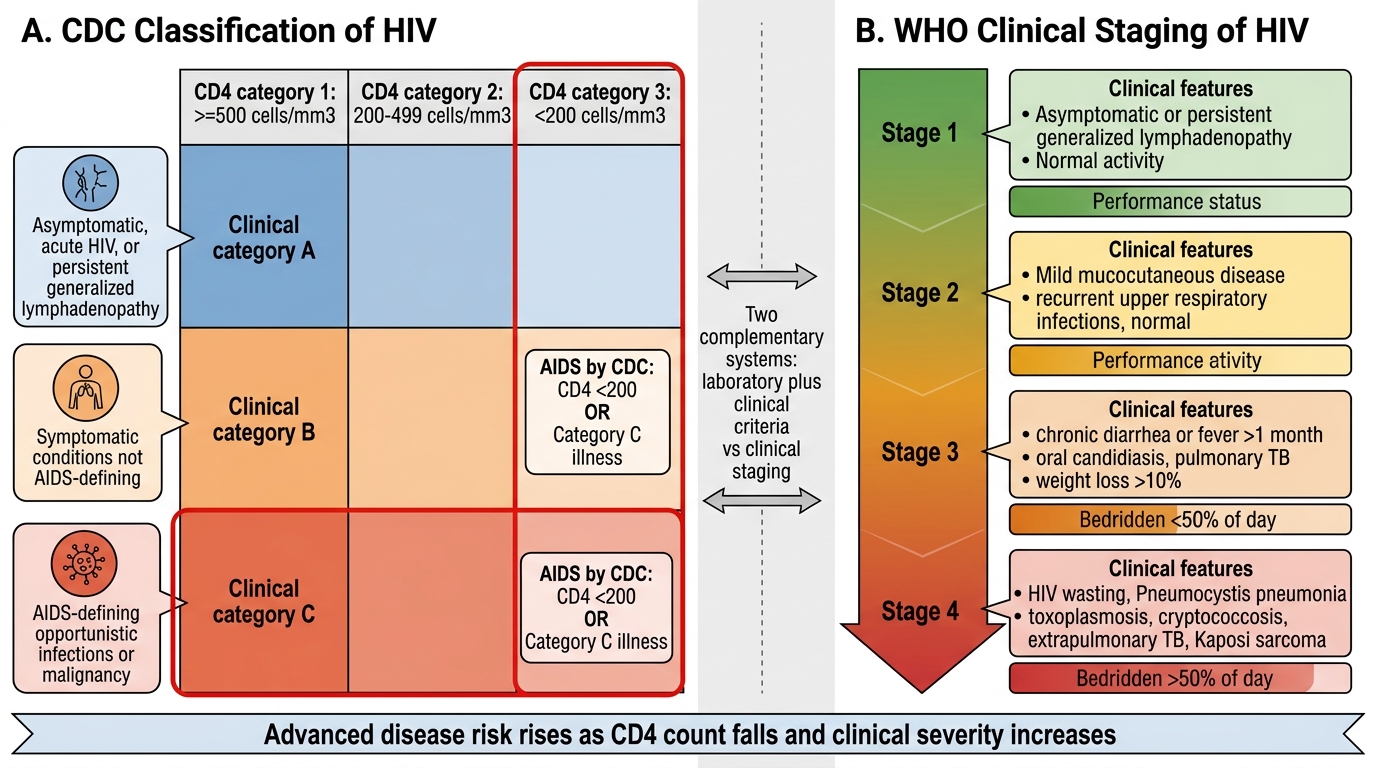
CDC and WHO Classification of HIV Disease
In India, NACO uses a combination of WHO staging (for clinical decision-making in ART centres) and CD4 count. Under the 'Treat All' policy instituted from 2017, ART is initiated for all PLHIV regardless of CD4 count or WHO stage — the CD4 threshold of 350 or 500 cells/µL that governed earlier guidelines is now obsolete for treatment initiation. However, CD4 count remains critical for prophylaxis decisions and for determining the urgency of ART initiation.
CD4 Count, Immunosuppression, and the Risk of Opportunistic Infections
The CD4 count is the single most important laboratory measure of immune competence in HIV infection. It reflects the current level of immunosuppression, predicts the risk of specific opportunistic infections (OIs), guides prophylaxis thresholds, and — before the 'Treat All' era — determined when to start ART. Understanding the relationship between CD4 count and OI risk is the conceptual scaffold on which all HIV management decisions are built. This is not a matter of memorising a table but of understanding that different pathogens require different levels of immune competence to be controlled: pathogens that are easily cleared by a modestly impaired immune system emerge at higher CD4 counts, while those that require near-intact immunity emerge only at profound immunosuppression.
The pathogenesis of this progressive immunological collapse is as follows. HIV gp120 envelope protein binds the CD4 receptor on T-helper cells; after co-receptor engagement (CCR5 for macrophage-tropic/R5 strains, CXCR4 for T-tropic/X4 strains), the viral membrane fuses with the host cell membrane. The viral RNA genome is reverse-transcribed into DNA by reverse transcriptase (highly error-prone → genetic diversity → drug resistance potential), then the double-stranded viral DNA is integrated into the host chromosome by integrase (forming the provirus). HIV-infected CD4 cells are depleted by: direct cytopathic effect (virus-mediated cell lysis), immune-mediated killing (cytotoxic CD8 T cells recognise infected cells), and chronically activated immune system-mediated bystander apoptosis. The progressive CD4 depletion impairs virtually every arm of adaptive immunity — helper function for CD8 cells, antibody class-switching support for B cells, and macrophage activation — creating a state of combined cellular and humoral immunodeficiency that mounts over years.
The key CD4 thresholds and their associated OI risks:
| CD4 count (cells/µL) | Major risks / recommended prophylaxis |
|---|---|
| <500 | Recurrent bacterial infections; herpes zoster; oral candidiasis; pulmonary TB (all CD4 levels, increased risk at all stages) |
| <200 | Pneumocystis jirovecii pneumonia (PCP) — initiate co-trimoxazole prophylaxis; cerebral toxoplasmosis (if Toxoplasma IgG+); Cryptosporidium diarrhoea; Microsporidiosis; Visceral leishmaniasis |
| <100 | Cryptococcal meningitis; CMV disease; disseminated histoplasmosis; Toxoplasma encephalitis |
| <50 | Disseminated Mycobacterium avium complex (MAC); CMV retinitis; primary CNS lymphoma; disseminated CMV; HIV wasting |
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
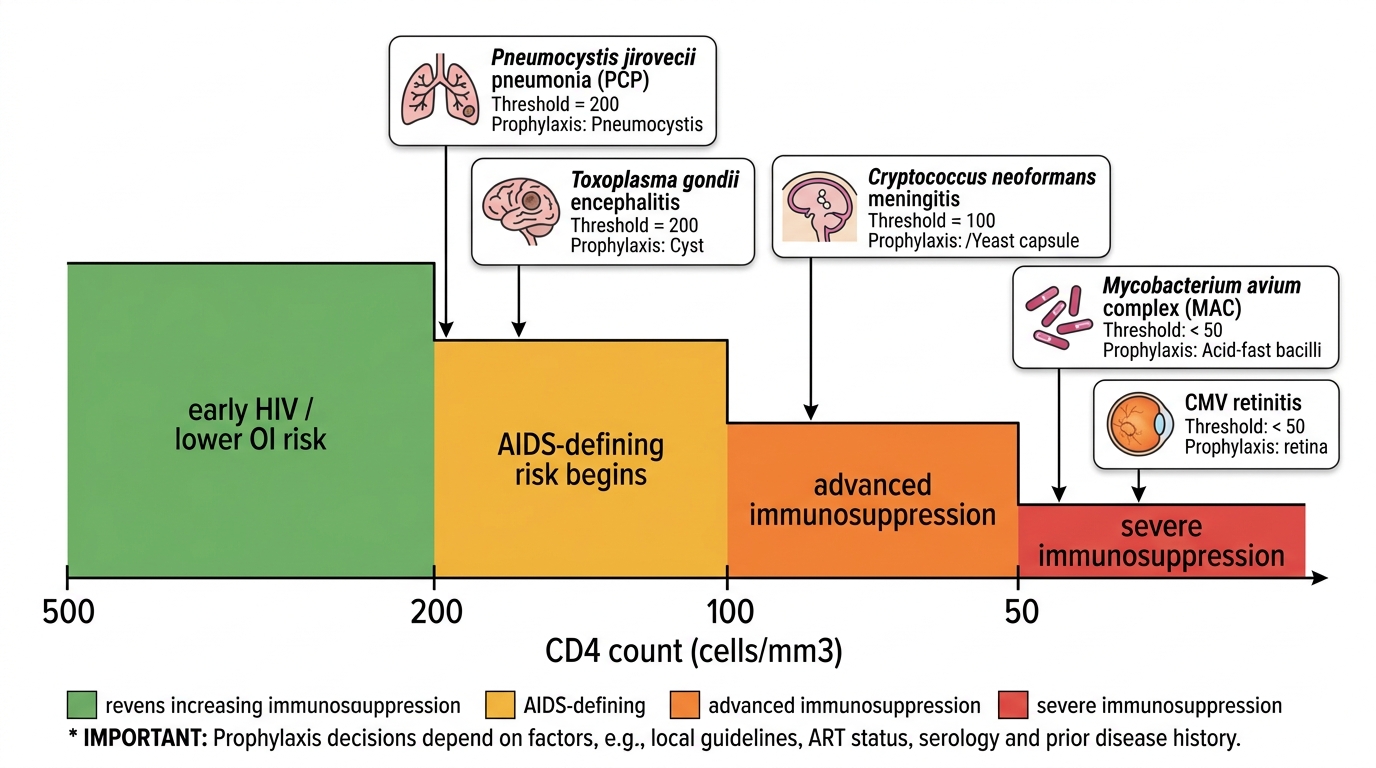
CD4 Thresholds for HIV Opportunistic Infections
Co-trimoxazole (trimethoprim-sulfamethoxazole, TMP-SMX) prophylaxis is indicated at CD4 <200 cells/µL and protects against PCP (primary prophylaxis), cerebral toxoplasmosis, some bacterial infections (Salmonella, Nocardia), and Isospora belli diarrhoea. In India, co-trimoxazole prophylaxis is recommended by NACO at CD4 <250 cells/µL (a slightly more conservative threshold than the global <200). Isoniazid preventive therapy (IPT) for latent TB should be considered for all PLHIV after excluding active TB — a critical Indian priority given the very high TB-HIV co-infection burden.
SELF-CHECK
A 28-year-old HIV-positive man has a CD4 count of 175 cells/µL and is not yet on ART. He is Toxoplasma gondii IgG-seropositive. Which prophylaxis regimen is MOST appropriate to initiate immediately?
A. Fluconazole 200 mg daily
B. Azithromycin 1250 mg weekly
C. Co-trimoxazole (TMP-SMX) double-strength once daily
D. Dapsone 100 mg daily alone
Reveal Answer
Answer: C. Co-trimoxazole (TMP-SMX) double-strength once daily
At CD4 <200 cells/µL, co-trimoxazole (TMP-SMX) is the first-line prophylaxis for both PCP and Toxoplasma gondii encephalitis (in a seropositive patient). It covers both pathogens in a single agent. Fluconazole is used for cryptococcal prophylaxis at CD4 <100. Azithromycin weekly is MAC prophylaxis at CD4 <50. Dapsone alone covers PCP but does NOT cover Toxoplasma — the combination of dapsone + pyrimethamine is the TMP-SMX-intolerant alternative for dual prophylaxis. Co-trimoxazole DS once daily remains the first-line choice.