Page 2 of 23
IM6.1-6 | HIV Foundations and Opportunistic Disease — SDL Guide (Part 2)
Common Opportunistic Infections: Pathogenesis and Clinical Features
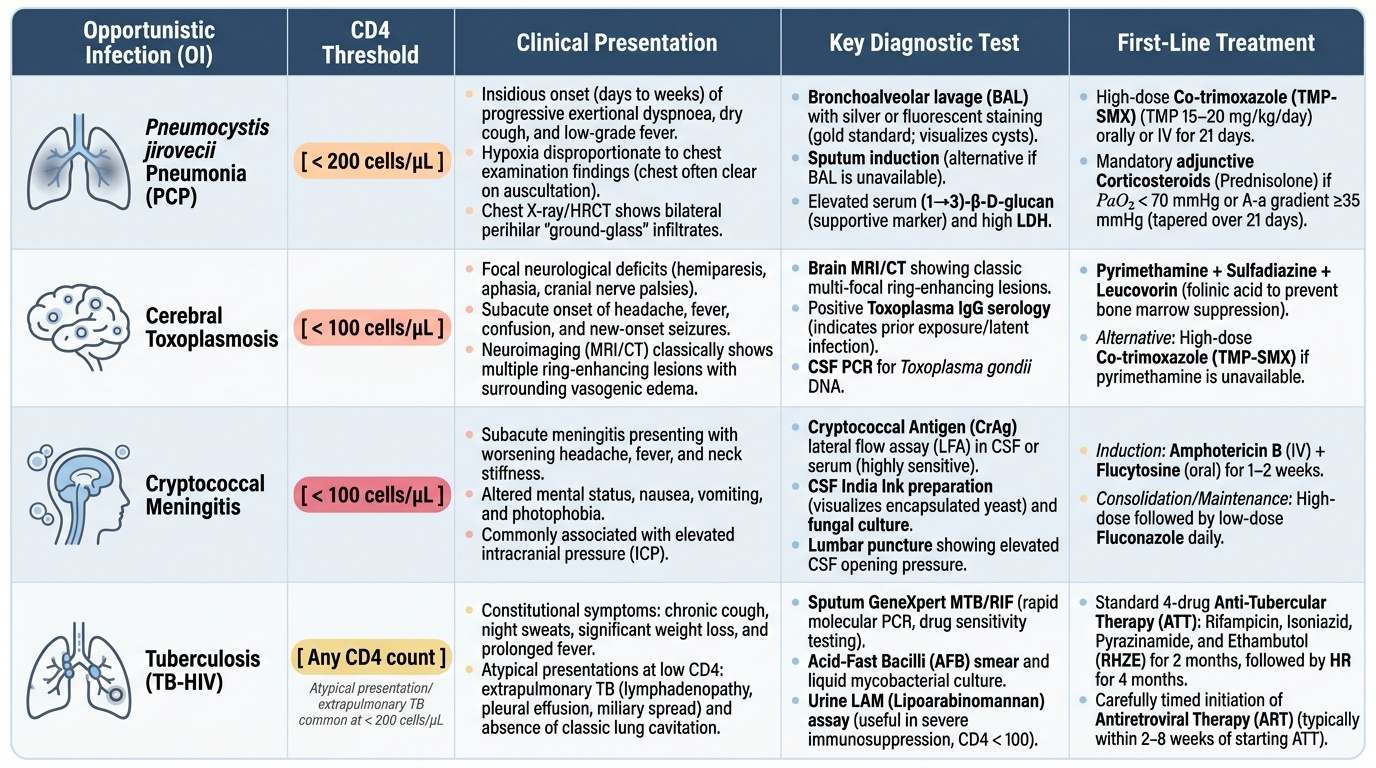
Opportunistic infections are the direct cause of most HIV-related morbidity and mortality. Their clinical presentation often differs from immunocompetent individuals — blunted inflammatory responses can mask classical signs, presentations may be atypical, and multiple co-infections are common. Each OI has a characteristic CD4 threshold, a predilection for specific organ systems, and a pathogen-specific diagnostic approach. The four most clinically important in the Indian context are discussed below in detail; the others are summarised in a reference table.
Provided image
1. Pneumocystis jirovecii Pneumonia (PCP) — formerly called Pneumocystis carinii pneumonia; the organism was reclassified as a fungus. PCP is the most common AIDS-defining OI in the non-TB world and typically occurs at CD4 <200 cells/µL. The pathogenesis involves inhalation and reactivation of latent pneumocystis organisms (most adults have been colonised by early childhood). In an immunocompromised host, the organisms proliferate within the alveolar spaces, filling alveoli with a frothy exudate and causing progressive gas exchange failure. Clinically, the onset is insidious — days to weeks of progressive exertional dyspnoea, dry non-productive cough, and low-grade fever, with examination revealing hypoxia disproportionate to the chest findings (sparse crackles or even clear chest). The chest X-ray classically shows bilateral perihilar interstitial or 'ground-glass' infiltrates, though it can be normal in up to 25% early. High-resolution CT (HRCT) shows bilateral ground-glass opacification with a geographic distribution. The LDH is typically markedly elevated (reflecting alveolar damage) and correlates with severity. Diagnosis: bronchoalveolar lavage (BAL) with silver or fluorescent stain for cysts is the gold standard; sputum induction is diagnostic in ~60% if BAL is unavailable. Serum (1→3)-β-D-glucan is elevated in PCP and can be a useful adjunct. Treatment: high-dose co-trimoxazole (TMP 15–20 mg/kg/day in 3 divided doses × 21 days) is first-line. Adjunctive corticosteroids (prednisolone 40 mg BD tapering over 21 days) are mandatory if PaO₂ <70 mmHg or A-a gradient >35 mmHg on room air — corticosteroids reduce the risk of respiratory failure and death in moderate-to-severe PCP. Second-line: IV pentamidine, atovaquone, or dapsone + trimethoprim.
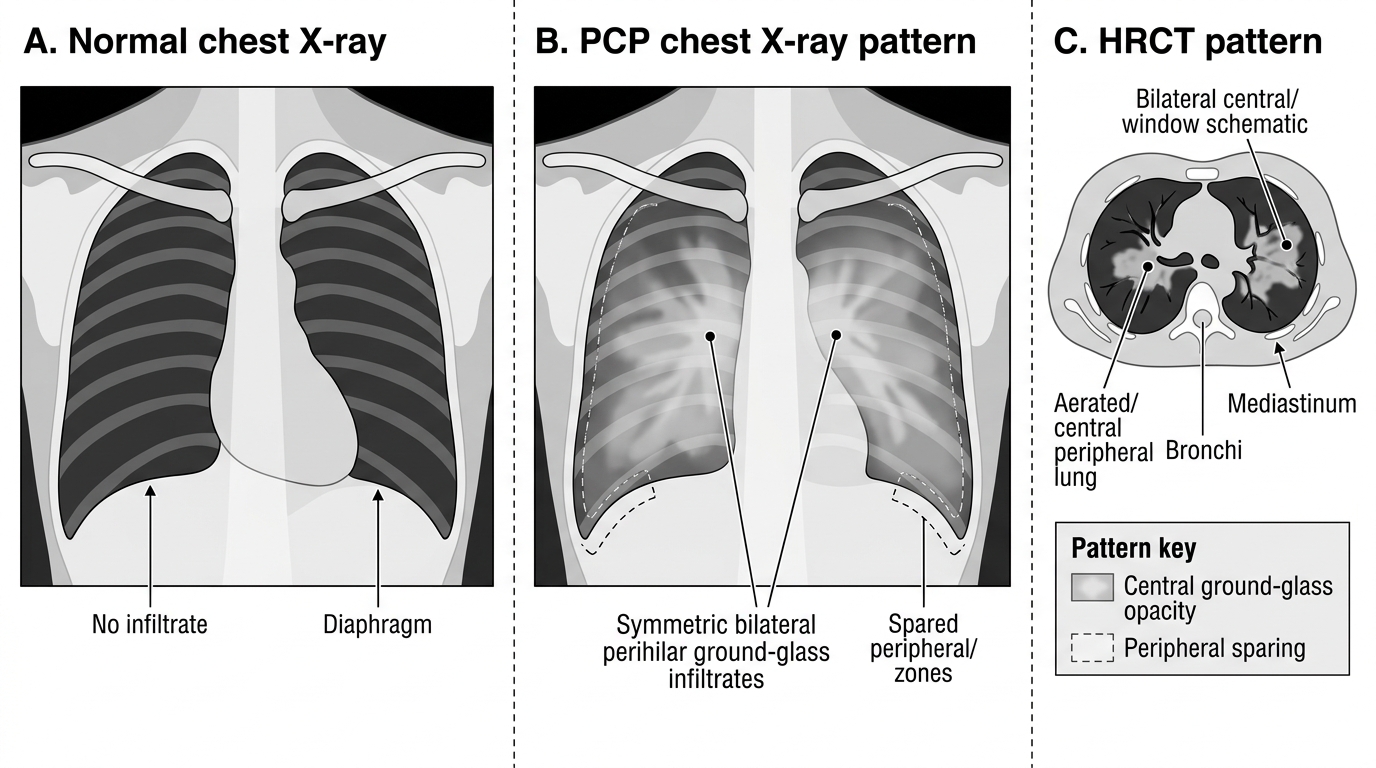
PCP Lung Imaging Pattern in HIV
2. Cerebral Toxoplasmosis — caused by Toxoplasma gondii, an obligate intracellular protozoan, typically presenting at CD4 <100 cells/µL (often <50). It almost always results from reactivation of latent cysts in the brain (primary infection from cat faeces or undercooked meat acquires latency in all seropositive individuals). Reactivation in immunosuppression causes multiple cerebral abscesses, preferentially in the basal ganglia and corticomedullary junction. Clinically: subacute onset of focal neurological deficits (hemiparesis, hemianopia, aphasia), altered consciousness, headache, and seizures — the combination of fever, focal neurology, and a CD4 <100 should trigger urgent neuroimaging. CT/MRI: multiple ring-enhancing lesions with surrounding oedema and mass effect, typically in basal ganglia. The key differential diagnosis is primary CNS lymphoma (usually a single ring-enhancing lesion, diffuse and larger, also in basal ganglia). Serum Toxoplasma IgG seropositivity supports reactivation toxoplasmosis (a seronegative patient is unlikely to have cerebral toxoplasmosis). Definitive diagnosis requires brain biopsy, but empirical treatment is standard: if the patient responds to anti-toxoplasma therapy (pyrimethamine + sulfadiazine + folinic acid) within 2 weeks on MRI, the diagnosis is confirmed. Pyrimethamine + sulfadiazine + leucovorin for 6 weeks is the treatment; then chronic suppression (secondary prophylaxis) with the same agents at reduced doses until CD4 >200 for ≥6 months on ART.
3. Cryptococcal Meningitis — caused by Cryptococcus neoformans, an encapsulated yeast, typically at CD4 <100 cells/µL. Infection is by inhalation of spores (bird droppings, soil); in immunosuppressed patients it disseminates to the CNS. Clinically: subacute or chronic meningitis (weeks of headache, fever, gradually worsening), often with minimal meningism (because the intense inflammation of classic bacterial meningitis requires a functional immune response). Raised intracranial pressure (ICP) is the most dangerous complication and the main cause of death — papilloedema, CN VI palsy, altered consciousness. Lumbar puncture (LP) findings: elevated opening pressure (often >25 cm H₂O), mildly elevated protein, mildly reduced glucose, India ink stain reveals encapsulated yeast (positive in ~70%), cryptococcal antigen (CrAg) in CSF is >90% sensitive (ELISA or LFA — lateral flow assay). Serum CrAg can be positive even before CNS involvement, enabling screening of PLHIV at CD4 <100. NACO protocol: serum CrAg screen at CD4 <100; CrAg-positive patients receive fluconazole pre-emptive therapy to prevent progression to meningitis. Treatment of confirmed meningitis: induction with IV Amphotericin B deoxycholate (1 mg/kg/day) + flucytosine (25 mg/kg QID) for 2 weeks; consolidation with fluconazole 400 mg/day for 8 weeks; maintenance with fluconazole 200 mg/day until CD4 >200 cells/µL for ≥6 months on ART. Therapeutic LP (to reduce ICP) is critically important — remove 20–30 mL CSF daily until opening pressure normalises.
4. HIV-TB Co-infection — India accounts for >25% of the global TB burden, and HIV is the strongest known risk factor for progression of latent TB to active disease (the relative risk is ~20-fold). TB can occur at any CD4 count but atypical presentations (extrapulmonary, disseminated, smear-negative) predominate at lower CD4 counts. Miliary TB, TB meningitis, and disseminated TB (affecting liver, spleen, bone marrow) are AIDS-defining. All PLHIV should be screened for active TB at every visit (WHO 4-symptom screen: cough, fever, weight loss, night sweats — a positive screen requires further investigation, negative screen can receive IPT). Treat TB first with standard NTEP regimen (2HRZE + 4HR) — weight-band based, daily FDCs — then start ART within 2 weeks (or 8 weeks if CD4 <50).
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
Major Opportunistic Infections in HIV
HIV-Related Malignancies
Malignancy complicates advanced HIV infection through two principal mechanisms: immunosuppression-related failure of immune surveillance (allowing proliferation of oncogenic viruses and tumour cells) and direct viral oncogenesis (HIV alters the tumour microenvironment, and co-infecting oncogenic viruses exploit the HIV-induced immune deficiency). The three AIDS-defining malignancies are Kaposi sarcoma, primary CNS lymphoma, and invasive cervical cancer. Understanding their pathogenesis is essential for recognising them clinically and for understanding why ART alone can cause regression of some tumours.
Provided image
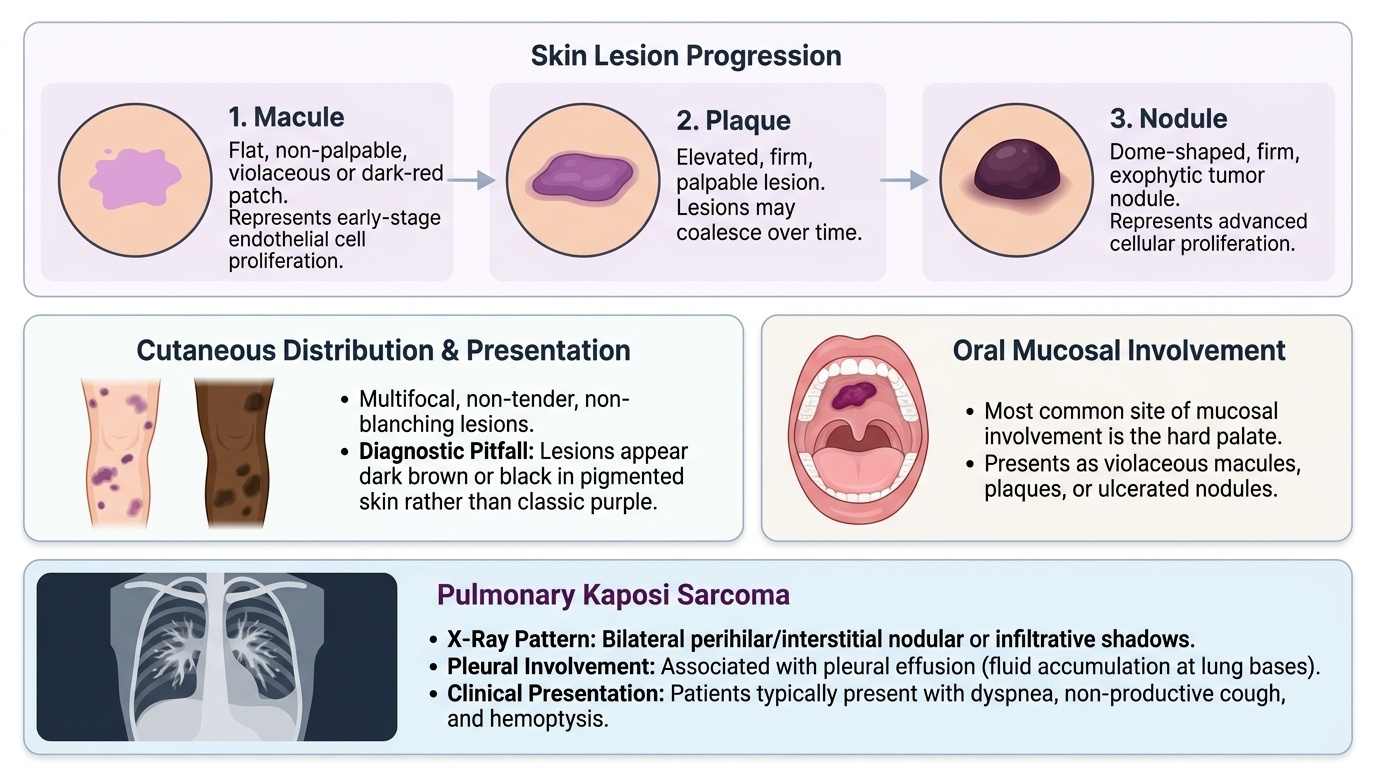
Kaposi Sarcoma (KS) is caused by co-infection with Human Herpesvirus 8 (HHV-8), also called Kaposi sarcoma-associated herpesvirus (KSHV). It is a spindle-cell vascular tumour with multiple clinical forms; the epidemic (AIDS-related) form affects PLHIV with CD4 <200 cells/µL, particularly men who have sex with men (MSM). Pathogenesis: HHV-8 infects endothelial and spindle cells; in the context of HIV-induced immunosuppression and HIV Tat protein-mediated angiogenesis, HHV-8 drives uncontrolled spindle-cell proliferation. Clinically: violaceous (dark purple or brown), non-tender, non-blanching papules, plaques, or nodules affecting the skin, oral mucosa, lymph nodes, GI tract, and lungs. In pigmented Indian skin, lesions may appear dark brown or black rather than the classic purple — a diagnostic pitfall. Oral KS is common on the hard palate. Pulmonary KS causes haemoptysis and a distinctive chest X-ray appearance (bilateral nodular or infiltrative shadows with pleural effusion). The diagnosis is clinical in typical cases; biopsy shows spindle cells and slit-like vascular spaces. ART alone can induce regression in early or limited disease by restoring immune surveillance; advanced disease (visceral or rapidly progressive) requires chemotherapy (liposomal doxorubicin or paclitaxel).
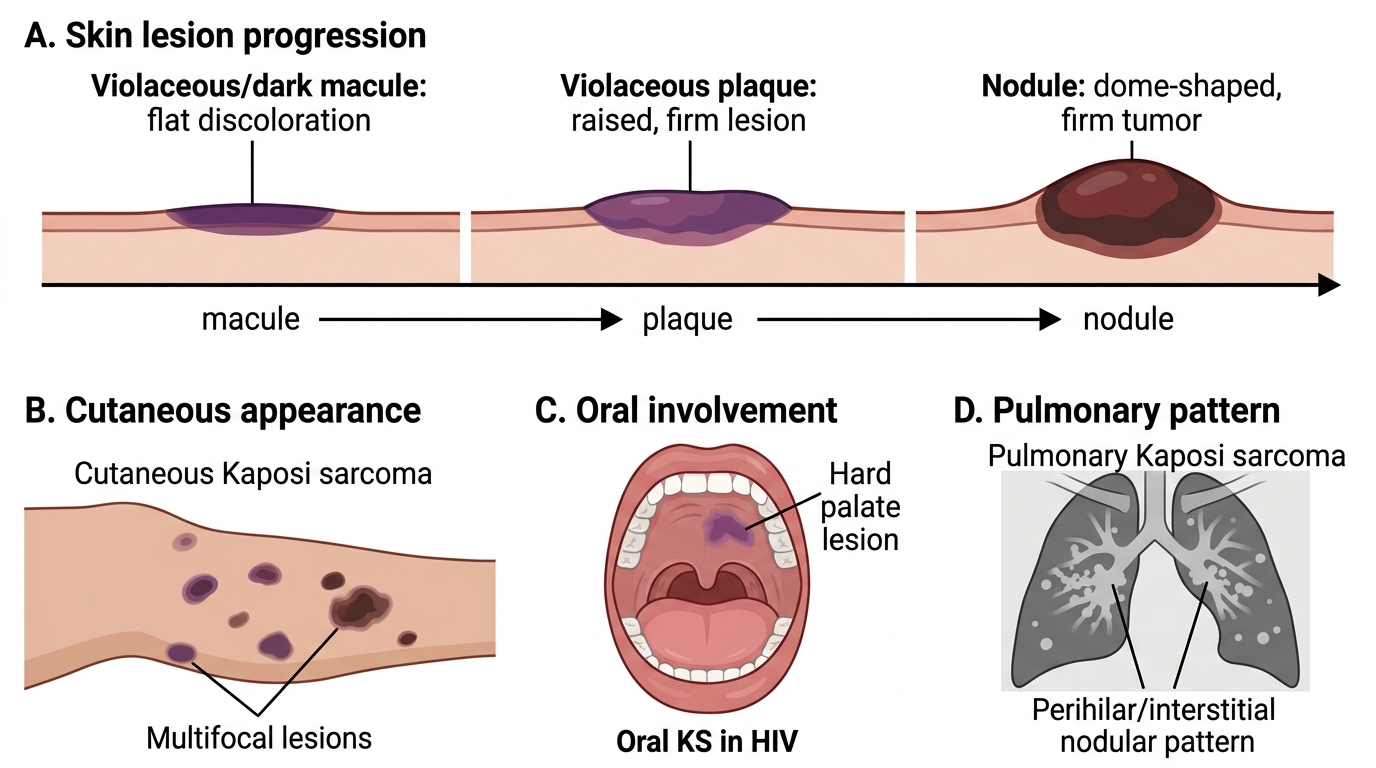
Clinical Appearance of Kaposi Sarcoma in HIV
Non-Hodgkin Lymphoma (NHL) — HIV patients have a 60–100-fold increased risk of aggressive B-cell NHL compared with the general population. The most common subtypes are Burkitt lymphoma (driven by EBV co-infection in some cases and MYC translocation) and diffuse large B-cell lymphoma (DLBCL). Primary CNS lymphoma (PCNSL) is uniformly associated with EBV in HIV patients and is AIDS-defining; it presents with focal neurological deficits and a single large ring-enhancing lesion on MRI — the key differential from cerebral toxoplasmosis. CSF EBV PCR and thallium-201 SPECT (positive in lymphoma, negative in toxoplasmosis) help distinguish them. Systemic NHL presents with extranodal involvement (GI tract, bone marrow, liver), B symptoms (fever, night sweats, weight loss), and unexplained cytopenias. Treatment is chemotherapy (R-CHOP for DLBCL, dose-adjusted regimens in HIV) with concurrent ART.
Invasive Cervical Cancer is AIDS-defining because HIV accelerates progression of HPV-related cervical intraepithelial neoplasia (CIN) to invasive cancer. HIV causes impaired immune clearance of high-risk HPV (HPV-16, HPV-18), enhanced HPV replication, and rapid CIN-to-cancer progression. PLHIV women require more frequent cervical cancer screening (Pap smear or VIA every 1–2 years vs every 3 years for the general population). ART does not fully reverse the increased cervical cancer risk, underscoring the importance of HPV vaccination and screening in PLHIV.
Other malignancies with increased incidence in HIV: Hodgkin lymphoma (paradoxically more common at intermediate CD4 levels, linked to EBV), anal cancer (HPV-driven, particularly in MSM), hepatocellular carcinoma (HIV accelerates hepatitis B and C progression to cirrhosis and HCC), and lung cancer (independent risk factor beyond smoking).
SELF-CHECK
A 34-year-old HIV-positive man with a CD4 count of 45 cells/µL presents with multiple dark-brown nodular skin lesions on the face, hard palate, and lower extremities, some ulcerated. He also has haemoptysis and a bilateral nodular infiltrate on chest X-ray. What is the MOST likely diagnosis and its causative pathogen?
A. Disseminated Mycobacterium avium complex (MAC) — M. avium-intracellulare
B. Cutaneous cryptococcosis — Cryptococcus neoformans
C. Kaposi sarcoma — Human Herpesvirus 8 (HHV-8)
D. Bacillary angiomatosis — Bartonella henselae
Reveal Answer
Answer: C. Kaposi sarcoma — Human Herpesvirus 8 (HHV-8)
Kaposi sarcoma (KS) is caused by HHV-8 and presents with violaceous/dark nodular lesions on skin, oral mucosa (hard palate is characteristic), and viscera including lungs (haemoptysis + bilateral nodular infiltrates on CXR). A CD4 of 45 cells/µL is consistent with AIDS-defining KS. Disseminated MAC causes systemic illness (fever, weight loss, anaemia, hepatosplenomegaly) without these skin and mucosal lesions. Cutaneous cryptococcosis can cause molluscum-like papules but not this multi-site nodular pattern. Bacillary angiomatosis (Bartonella) causes papular skin lesions resembling early KS but is distinguished by biopsy (HHV-8 positive in KS vs negative in bacillary angiomatosis).
HIV-Related Skin and Oral Lesions
Skin and oral lesions are among the most visible and accessible markers of HIV disease stage and CD4 count. Many dermatological conditions in PLHIV occur at specific immune thresholds, making the skin 'a window onto the immune system.' Recognising these lesions enables rapid clinical staging, and some — like oral hairy leucoplakia — are virtually pathognomonic of HIV infection.
Provided image
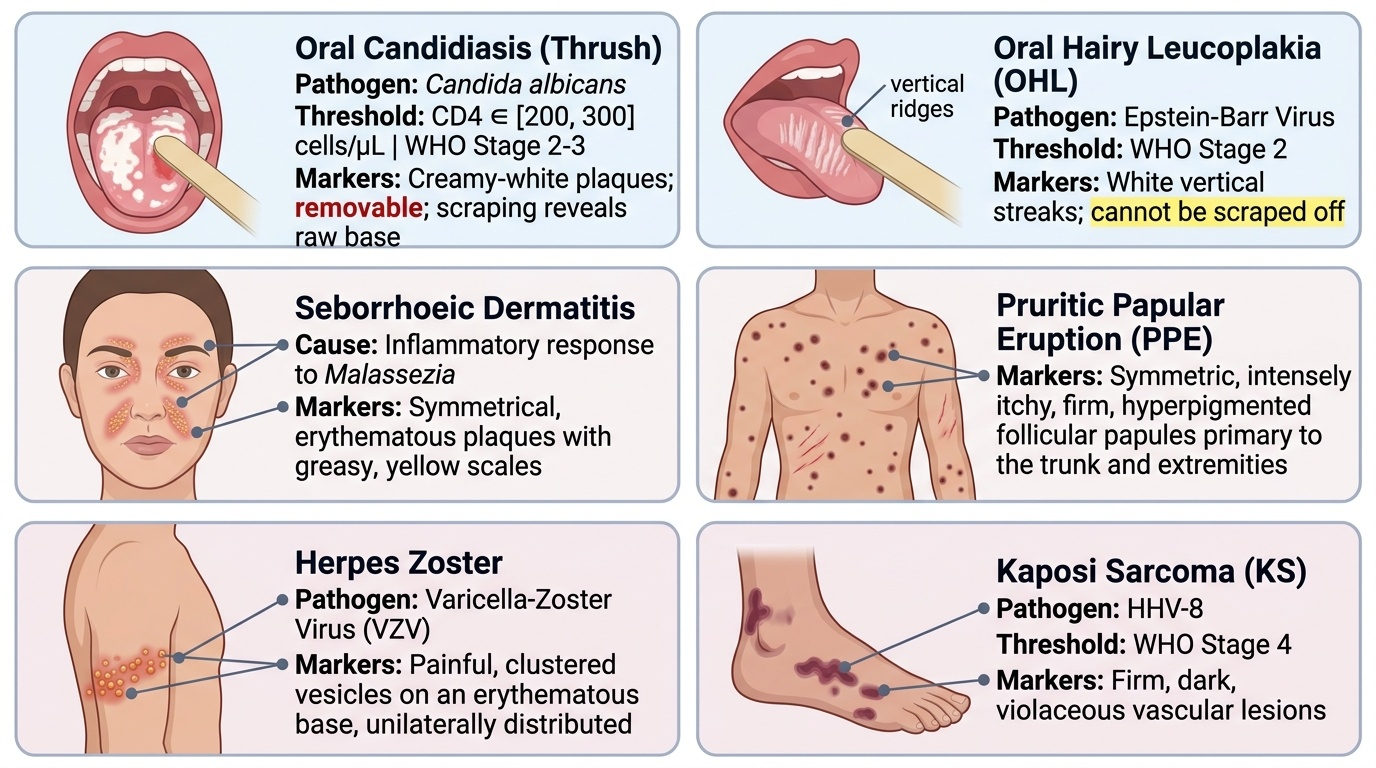
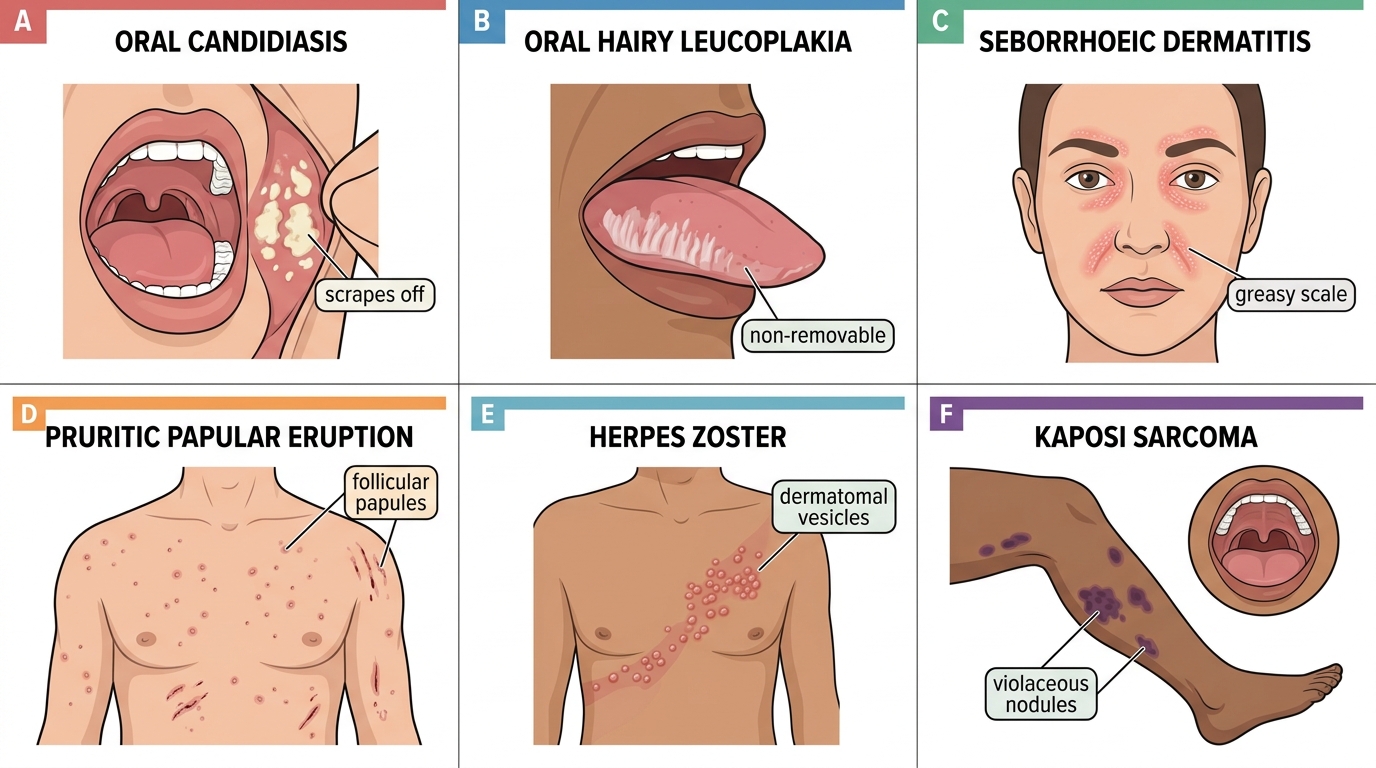
Oral Candidiasis (Thrush) — the most common oral manifestation; occurs at CD4 <200–300 cells/µL. Caused by Candida albicans. Three forms: (1) Pseudomembranous candidiasis — white curd-like plaques on the buccal mucosa, palate, tongue, or oropharynx that can be wiped off leaving a red, bleeding surface; (2) Erythematous (atrophic) candidiasis — flat, red patches on the dorsum of the tongue or hard palate; (3) Angular cheilitis — erythema and fissuring at the corners of the mouth. Oral candidiasis is a WHO Stage 2–3 feature. Treatment: fluconazole 100–200 mg/day × 7–14 days; topical nystatin or clotrimazole for mild cases.
Oral Hairy Leucoplakia (OHL) — a WHO Stage 2 lesion caused by Epstein-Barr virus (EBV) replication in epithelial cells. Presents as white vertical streaks or corrugated (hairy) plaques on the lateral borders of the tongue, which — critically — cannot be scraped off (unlike oral candidiasis, which can). It is usually asymptomatic, requires no specific treatment, and regresses with effective ART. OHL is virtually diagnostic of HIV infection in the appropriate context.
Seborrhoeic Dermatitis — a WHO Stage 2 condition, more severe and more extensive in HIV than in the general population. Presents as greasy yellowish scales on the nasolabial folds, eyebrows, scalp, ears, and central chest, with erythematous base. Caused by exaggerated response to Malassezia yeasts in the context of immune dysregulation. Management: topical antifungals (ketoconazole shampoo/cream) and mild corticosteroids.
Pruritic Papular Eruption (PPE) — the most common HIV-specific dermatosis in Africa and Asia, occurring at CD4 <200–350 cells/µL. Presents as symmetrical itchy follicular papules on the trunk, arms, and legs, with post-inflammatory hyperpigmentation (particularly visible in dark skin). The pathogenesis involves exaggerated immune response to insect antigens (demodex, follicular mites). Diagnosis is clinical; biopsy shows eosinophilic folliculitis. Treatment: potent topical corticosteroids, antihistamines; ART leads to resolution.
Herpes Zoster — reactivation of varicella-zoster virus (VZV) in the dorsal root ganglia, occurring at CD4 200–500 cells/µL (WHO Stage 2). A single dermatomal vesicular eruption in a young adult is a classic indicator of underlying HIV. Multidermatomal or disseminated zoster (involving >2 dermatomes or viscera) suggests more profound immunosuppression. Treatment: acyclovir (800 mg 5× daily for 7 days for localised disease; IV acyclovir 10 mg/kg TDS for disseminated or ophthalmic involvement).
Molluscum Contagiosum — caused by Molluscum contagiosum virus (MCV); in HIV, it presents atypically with multiple, large (>5 mm), confluent lesions on the face (particularly the beard area) — unlike the self-limiting small lesions in immunocompetent children. The number and size of lesions inversely correlates with CD4 count; resolution follows immune reconstitution with ART.
Kaposi Sarcoma (skin lesions) — covered in detail in the malignancy section; in Indian patients with dark skin, lesions may be dark brown or black; look for the characteristic hard palate involvement.
Major HIV-Associated Skin and Oral Lesions
SELF-CHECK
A 36-year-old HIV-positive woman presents with white lesions on the lateral border of the tongue. Unlike her previous oral lesion (white plaques inside the cheeks that could be wiped off), these CANNOT be removed by scraping. What is the MOST likely diagnosis and its causative virus?
A. Oral candidiasis — Candida albicans
B. Oral hairy leucoplakia — Epstein-Barr virus (EBV)
C. Oral herpes simplex — HSV-1
D. Condyloma acuminatum — Human papillomavirus (HPV)
Reveal Answer
Answer: B. Oral hairy leucoplakia — Epstein-Barr virus (EBV)
Oral hairy leucoplakia (OHL) is caused by Epstein-Barr virus (EBV) replication in epithelial cells and presents as white corrugated/hairy plaques on the lateral borders of the tongue that CANNOT be scraped off — the key distinguishing feature from oral candidiasis (which scrapes off leaving a bleeding surface). OHL is a WHO Stage 2 indicator and is virtually pathognomonic of HIV infection in the clinical context. Oral herpes simplex typically causes painful ulcers, not white plaques. HPV-related condylomata occur on the palate and oral mucosa but not as lateral tongue streaks.