Page 5 of 23
IM7.8-10 | Rheumatologic Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and structure a rheumatologic history across seven clinical domains
- Perform the GALS screen and regional joint examination using look-feel-move at each joint
- Identify and document key signs of synovitis, periarticular disease, and skin/nail/muscle involvement
- Apply the MCP squeeze test, Schober test, FABER test, and other specific rheumatologic tests
- Generate and prioritise a differential diagnosis based on the clinical pattern of joint involvement and extra-articular features
- Present a structured rheumatologic case assessment to a supervising clinician
INSTRUCTIONS
This module develops the clinical skill of rheumatologic history-taking, systematic joint and skin examination, and structured differential diagnosis generation. These are SH-level competencies requiring bedside practice under supervision — reading alone is not sufficient. Use the structured history framework and GALS examination approach on every musculoskeletal patient you see in the clinic.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chapter 353 — Approach to Articular and Musculoskeletal Disorders (textbook)
- API Textbook of Medicine, 10th ed., Musculoskeletal History and Examination (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Chapter 26 — Assessment of the Musculoskeletal System (textbook)
- GALS Screen — Doherty M et al., Annals of Rheumatic Diseases 1992 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Priya, a 30-year-old software engineer, walks into your outpatient clinic and says: 'Doctor, both my hands are aching and I have been feeling tired for the past three months.' In 25 minutes, you need to determine whether she has rheumatoid arthritis, lupus, a viral arthritis, fibromyalgia, or one of a dozen other conditions — without an autoimmune panel, and possibly without an X-ray. Your most powerful diagnostic instrument in this encounter is not a laboratory — it is the structured history you take and the hands-on examination you perform. How you question her, in what order, and with what specific clinical detail will determine whether you leave the room with a working diagnosis and a logical investigation plan, or with a vague impression and a scatter-gun blood test request. Rheumatologic history and examination is a teachable, learnable skill — one that reduces unnecessary investigation costs, accelerates diagnosis, and is examined at every level of clinical assessment from MBBS to postgraduate fellowship.
WHY THIS MATTERS
The NMC competencies IM7.8 (elicit, document, and present a medical history that will differentiate the aetiologies of disease) and IM7.9 (perform a systematic examination of all joints, muscles, and skin that will establish the diagnosis and severity of disease) are SH-level competencies — meaning students are expected to be able to perform these skills under supervision in a real patient encounter, not merely describe them. IM7.10 (generate and prioritise a differential diagnosis based on clinical features) is a KH-level integration competency that bridges history and examination to clinical reasoning. Together, these three competencies constitute the clinical bedrock of rheumatologic practice. In India, where serological testing is expensive, access to specialist care may be delayed, and conditions like TB joint disease must always be actively considered, a thorough bedside evaluation is not merely good practice — it is often the only reliable diagnostic tool available.
RECALL
Before proceeding, activate your foundational knowledge. Recall from the previous module that rheumatologic complaints arise from four anatomical compartments: the synovial joint (articular), the periarticular structures (tendons, bursae, entheses), the bone, and the systemic/multi-organ domain. Recall that the two most important clinical discriminations are (a) inflammatory vs mechanical — based primarily on morning stiffness duration, and (b) articular vs periarticular — based on whether both active and passive joint movement are restricted (articular) or only specific active movements are painful with preserved passive ROM (periarticular). Also recall that arthralgia (pain only, no objective signs) and arthritis (pain + objective signs of synovitis: warmth, swelling, tenderness) are not synonymous. These distinctions are generated from the history and examination — not from blood tests.
Clinical Indication and Relevance of Rheumatologic History
The rheumatologic history is indicated whenever a patient presents with joint pain, muscle pain, stiffness, swelling, skin rash in combination with joint symptoms, unexplained fatigue, or features suggesting systemic inflammatory disease. It is relevant not only to the rheumatology outpatient setting but also to internal medicine, emergency medicine, paediatrics, and obstetrics — where connective tissue diseases such as SLE may present for the first time. A structured rheumatologic history transforms an undifferentiated complaint of 'my joints hurt' into a clinically useful localisation across the four diagnostic axes — compartment, number of joints, temporal pattern, and inflammatory vs mechanical character — before any investigation is ordered.
The history serves two simultaneous functions. First, it generates a hypothesis — by the end of the history, the clinician should have a working diagnosis or a short ranked differential list. Second, it directs the examination — knowing that a patient describes stiffness in both wrists, MCPs, and PIPs lasting 2 hours after waking will direct you to examine the small joints of the hand systematically rather than performing a general musculoskeletal survey. This targeted examination is more efficient and more informative than a non-directed approach. In busy Indian outpatient settings where time per patient is limited, the clinician who takes a focused rheumatologic history and examines precisely is more effective than one who orders a blanket autoimmune panel and waits for results before forming a hypothesis.
Structured Rheumatologic History Framework
Taking the Rheumatologic History: A Structured Approach
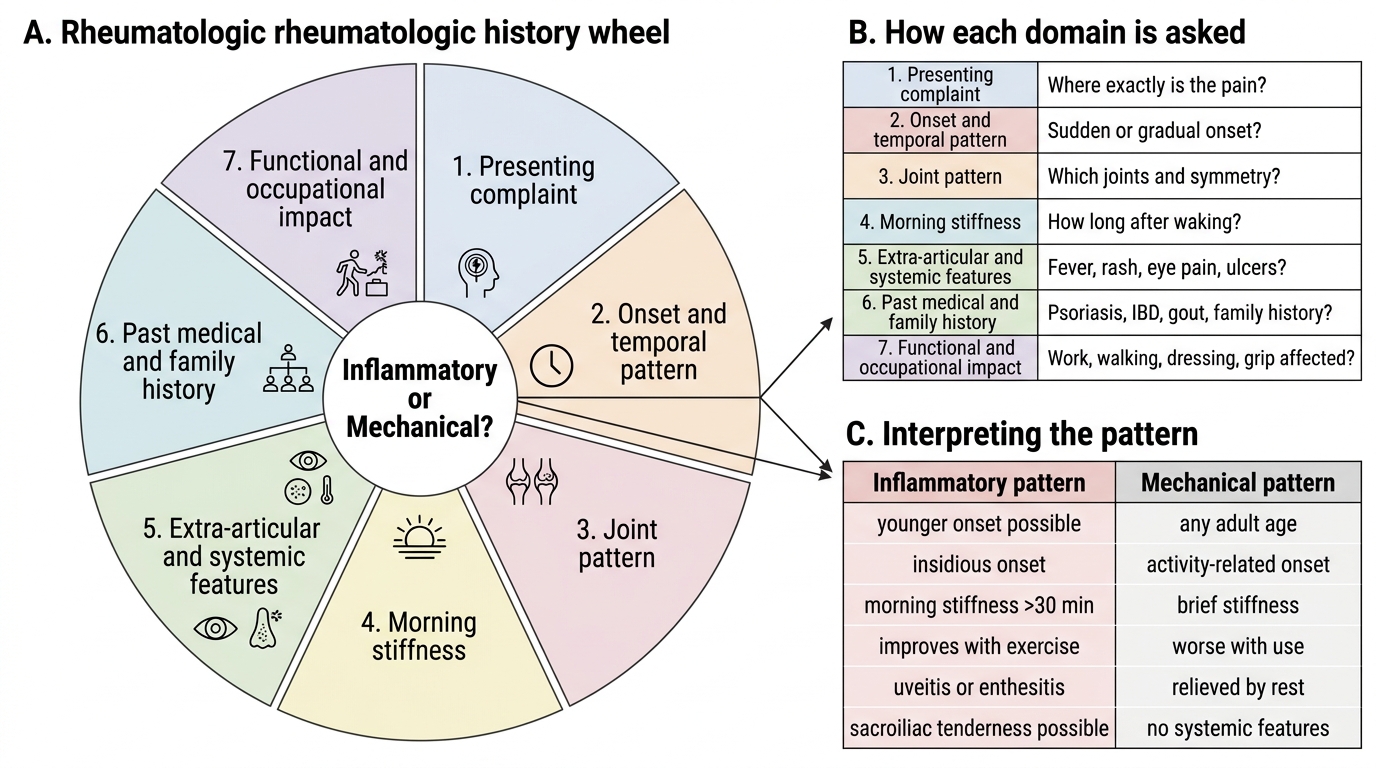
A structured rheumatologic history follows seven domains. Each domain is asked in a specific way that generates the most clinically useful information. Students who understand why each question is asked will ask it more naturally and interpret the answer more accurately than those who memorise a checklist without mechanistic understanding. The following framework is derived from Harrison's, Davidson's, and the API Textbook approach to musculoskeletal history — adapted for the Indian outpatient setting where time and resources are finite.
Provided image
Domain 1 — Presenting complaint and onset. Ask: 'Where exactly is your pain?' (joint line vs periarticular), 'When did it start?', 'How did it start — sudden (acute, overnight as in gout) or gradual (weeks to months as in RA)?', 'Did it start in one joint and spread, or in multiple joints from the beginning?'. Sudden onset monoarthritis of the first MTP joint overnight is gout until proven otherwise. Insidious symmetric polyarthritis of the small joints over weeks is RA until proven otherwise.
Domain 2 — Joint pattern (number, distribution, symmetry, migration). 'Which joints are affected?' Ask the patient to point. Confirm with examination. 'Are both sides equally affected (symmetric) or one side more than the other (asymmetric)?'. 'Has the pain moved from joint to joint (migratory — rheumatic fever, gonococcal arthritis) or accumulated (additive — RA, OA)?'. Map the joint involvement: small (MCP, PIP, DIP, wrist, MTP) vs large (knee, hip, shoulder, ankle); axial (sacroiliac, lumbar, cervical) vs peripheral.
Domain 3 — Morning stiffness. Ask: 'Do you feel stiff when you wake up?' If yes: 'How long does the stiffness last before you can move normally?' Duration ≥1 hour = inflammatory arthritis; <30 minutes = mechanical/degenerative. This single question is the most diagnostically powerful in the entire history. Ask it in every joint consultation without exception. Note that afternoon stiffness ('inactivity stiffness' while sitting) is also inflammatory, though less marked.
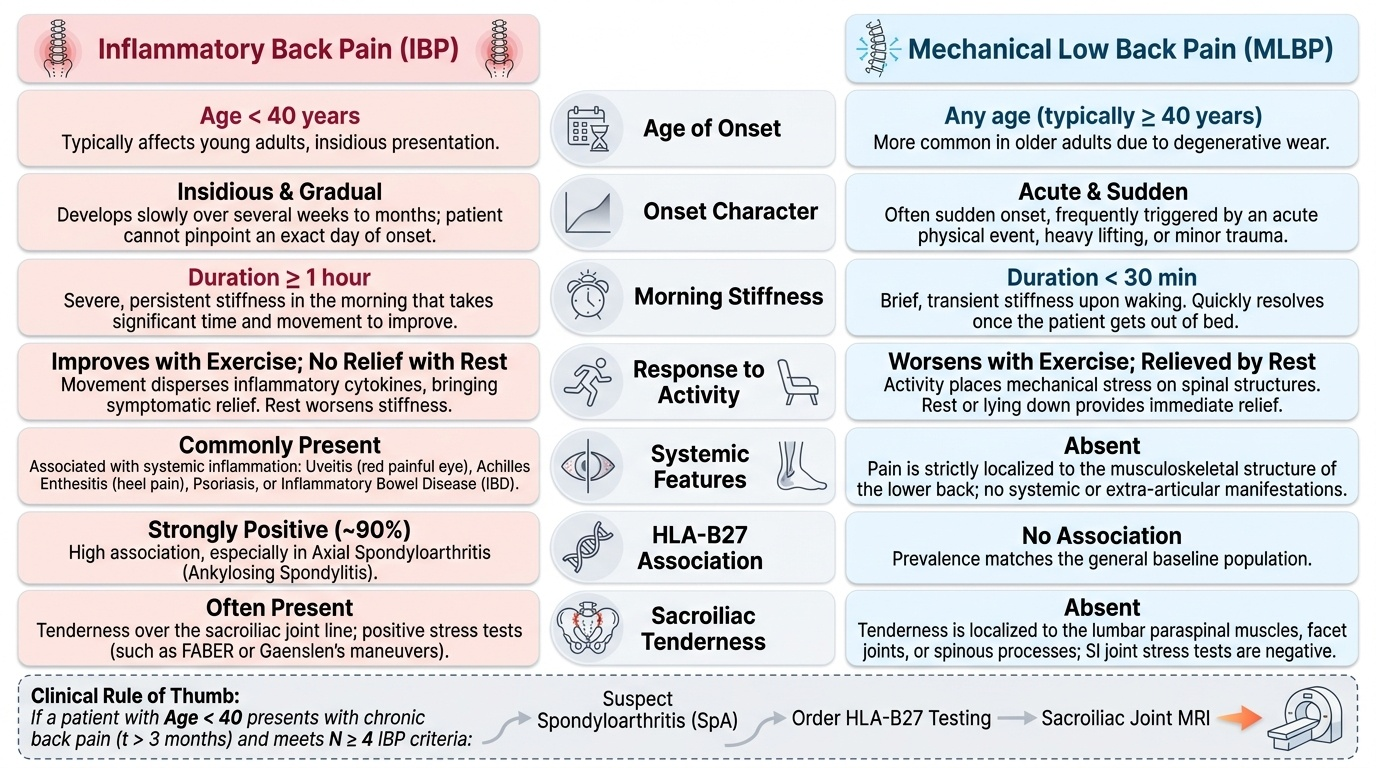
Domain 4 — Aggravating and relieving factors. 'Does the pain get better or worse with movement?' Inflammatory arthritis improves with movement (cytokines disperse); mechanical pain worsens with use. 'Does rest help?' Inflammatory: rest worsens stiffness; mechanical: rest relieves pain. 'Does exercise make it better or worse?' Inflammatory back pain in ankylosing spondylitis is characteristically BETTER with exercise — a diagnostically key feature that differentiates it from mechanical low back pain.
Domain 5 — Extra-articular and systemic symptoms. Screen systematically for organ involvement using a brief organ-by-organ review:
- Skin: rash (where? photosensitive? psoriatic plaques?), hair loss, oral ulcers, Raynaud's phenomenon
- Eyes: red eye (uveitis — spondyloarthropathy), dry eyes (Sjögren syndrome)
- Mouth: dryness (Sjögren), ulcers (SLE, reactive arthritis, Behçet)
- Constitutional: fever (RA low-grade; adult-onset Still's = high spiking quotidian fever), weight loss, fatigue, lymphadenopathy
- Genitourinary: urethritis/cervicitis (reactive arthritis), past STI
- Bowel: diarrhoea, rectal bleeding (IBD-associated arthritis)
- Family history: first-degree relatives with psoriasis, ankylosing spondylitis, RA, IBD, gout — all have familial associations
Domain 6 — Past medical history and medications. Previous joint problems, previous infections that preceded arthritis, TB history (relevant for TB joint disease and before starting biologics), current medications (some drugs cause drug-induced lupus — hydralazine, isoniazid, procainamide; gout can be triggered by diuretics, low-dose aspirin, cyclosporin).
Domain 7 — Functional impact and occupational history. 'Which activities can you no longer do that you could before?' Grip strength, climbing stairs, writing, opening jars — functional loss is the outcome metric of rheumatic disease and its treatment. Occupational history: repetitive strain injuries are periarticular; certain occupations increase gout risk (diuretic use in the elderly) or reactive arthritis risk.
SELF-CHECK
A 28-year-old man has had low back pain for 8 months. He says it is worst in the early morning, makes him wake up in the night, and actually gets better after he goes for a morning run. There is no history of trauma. Which historical feature is MOST specific for inflammatory back pain (axial spondyloarthropathy)?
A. Young age of onset
B. Nocturnal waking due to pain
C. Improvement with exercise
D. No history of trauma
Reveal Answer
Answer: C. Improvement with exercise
Improvement with exercise is the most specific feature of inflammatory back pain (axial spondyloarthropathy, including ankylosing spondylitis). In mechanical low back pain, exercise typically worsens the pain. The paradox of inflammatory back pain — better with movement, worse with rest — reflects the underlying mechanism: cytokines accumulate during inactivity and disperse with movement. Young age of onset and nocturnal waking are also features of inflammatory back pain, but improvement with exercise is the single most diagnostically specific feature. This directly distinguishes axial spondyloarthropathy from mechanical disc disease or spondylosis.
Systematic Joint Examination: Technique and Findings
The systematic joint examination follows the principle of look, feel, move at every joint, combined with specific special tests where indicated. This sequence is applied consistently whether examining the hands in a 3-minute focused exam or performing a full GALS screen (Gait, Arms, Legs, Spine). The GALS screen is a validated rapid musculoskeletal assessment tool that takes 2–3 minutes and identifies which regional examination to focus on in depth. The purpose of the examination is twofold: to confirm the presence and nature of joint pathology (synovitis, structural deformity, periarticular inflammation) and to document the distribution and severity of disease for baseline comparison and monitoring. Mastery of the examination sequence — knowing what to look for, where to palpate, and how to interpret the findings in real time — is an SH-level competency that can only be developed through repeated supervised bedside practice. What follows is the technique in sufficient detail to begin that practice.
The GALS screen (Gait, Arms, Legs, Spine):
- Gait: observe normal walking, turning, stopping — reveals gross lower limb or spine pathology
- Arms: arms above head (shoulder ROM), hands behind head (external rotation), prayer sign and reverse prayer sign (wrist flexion/extension), make a fist (grip), supinate/pronate (forearms), squeeze MCPs across the row (metacarpal squeeze test for MCP synovitis)
- Legs: knee flexion to 90° (knee ROM), ankle dorsiflexion (subtalar), squeeze MTPs (metatarsal squeeze test for MTP synovitis — a sensitive sign of early RA of the feet)
- Spine: cervical rotation, forward flexion (lumbar — Schober test for ankylosing spondylitis), lateral flexion; inspect for kyphosis or loss of lumbar lordosis
Hand and wrist examination in detail:
1. Inspection: skin (erythema, psoriatic plaques, nail pitting/onycholysis), deformities (swan-neck, boutonnière, ulnar deviation, Heberden's/Bouchard's nodes), swelling (diffuse = synovial thickening in RA; focal = gout tophus; sausage digit = dactylitis)
2. Palpation: MCP squeeze test (transverse pressure across the metacarpal heads — tenderness indicates MCP synovitis, very sensitive for RA); palpate each MCP, PIP, and DIP joint individually for warmth and tenderness; palpate wrist joint line, distal radioulnar joint
3. Movement: power grip (make a fist and squeeze examiner's fingers), precision grip (pinch), wrist flexion/extension/deviation; compare with contralateral side
Knee examination:
1. Inspection: swelling (prepatellar bursitis — focal, anterior to patella; joint effusion — diffuse, bulging on medial and lateral aspects of patella), deformity (valgus = RA; varus = OA), quadriceps wasting (suggests chronic joint disease)
2. Palpation: warmth by comparing with dorsum of examiner's hand; patellar tap test (large effusion — ballottement of patella); bulge/wipe test (small effusion — fluid shifts from medial gutter to lateral and back); joint line tenderness (medial/lateral); assessment of synovial thickening
3. Movement: flexion/extension (normally 0–135°); note pain and crepitus
Spine examination for spondyloarthropathy:
- Schober's test: mark 10 cm above and 5 cm below the posterior superior iliac spines (15 cm total); ask patient to bend maximally forward; distance should increase to ≥20 cm; if <20 cm = restricted lumbar flexion (ankylosing spondylitis)
- Chest expansion: at the nipple line during maximal inspiration vs forced expiration; normal ≥5 cm; <2.5 cm = costovertebral joint involvement in AS
- Occiput-to-wall distance: patient stands with heels and back against wall; occiput should touch the wall; positive (gap) indicates kyphosis from AS
- Sacroiliac joint tenderness: direct pressure over the SI joints posteriorly and FABER test (hip flexion, abduction, external rotation with knee at 90° — pressure on the contralateral SI joint causes pain)
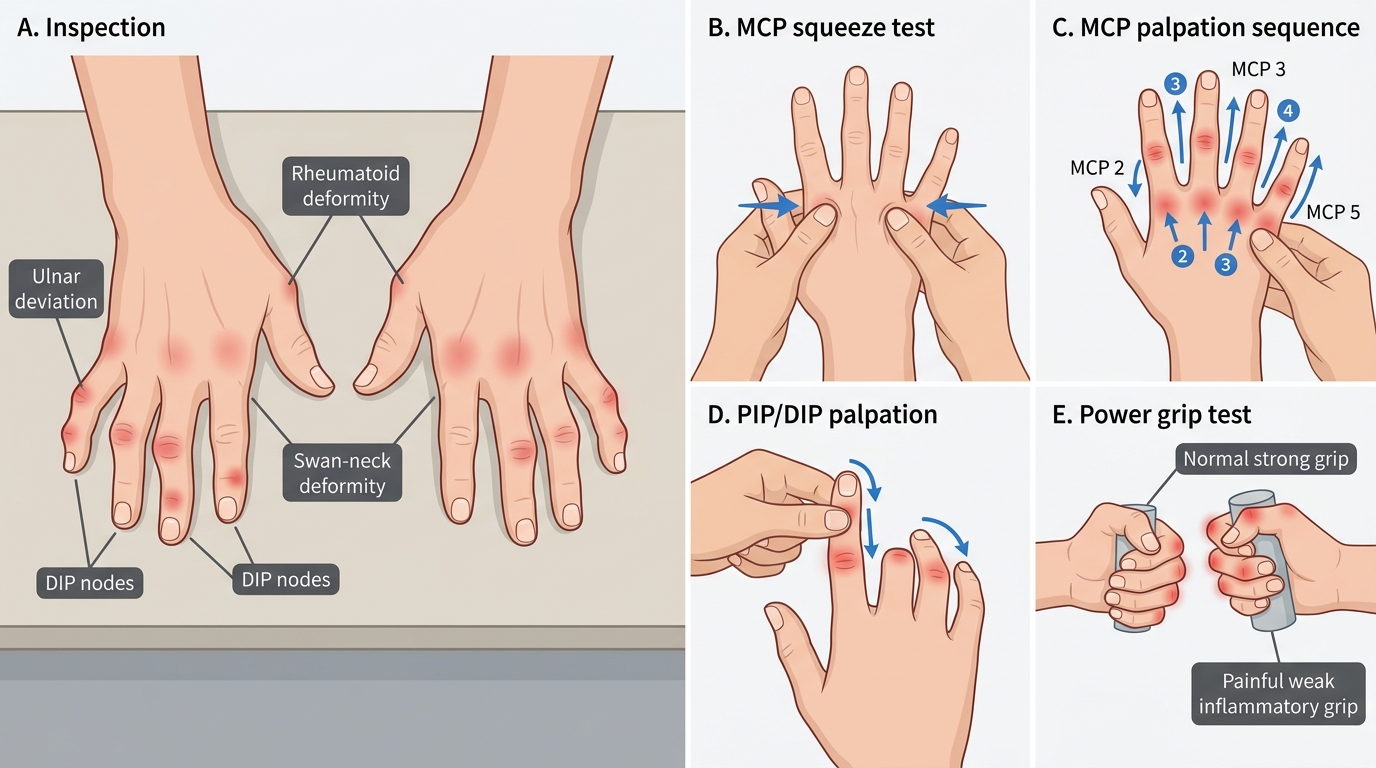
Hand and Wrist Examination in Rheumatologic Disease