Page 6 of 23
IM7.8-10 | Rheumatologic Clinical Evaluation — SDL Guide (Part 2)
Skin and Muscle Examination in Rheumatologic Disease
Dermatological and muscle examination is an integral part of the rheumatologic assessment — the skin is often the first organ to declare the diagnosis, and muscle weakness pointing to inflammatory myopathy is missed if not specifically tested. A complete rheumatologic examination must include inspection of the skin, nails, scalp, mucosae, and a brief assessment of proximal muscle power. Students often focus exclusively on the joints and neglect this broader survey, losing diagnostic information that is readily available at the bedside. The skin signs described below are not incidental findings — in conditions such as dermatomyositis, SLE, and psoriatic arthritis, skin examination is often the key that unlocks the diagnosis before any laboratory test result returns. This section covers the systematic approach to examining these structures in the context of rheumatologic disease, with the mechanistic rationale for each sign.
Skin examination — what to look for and where:
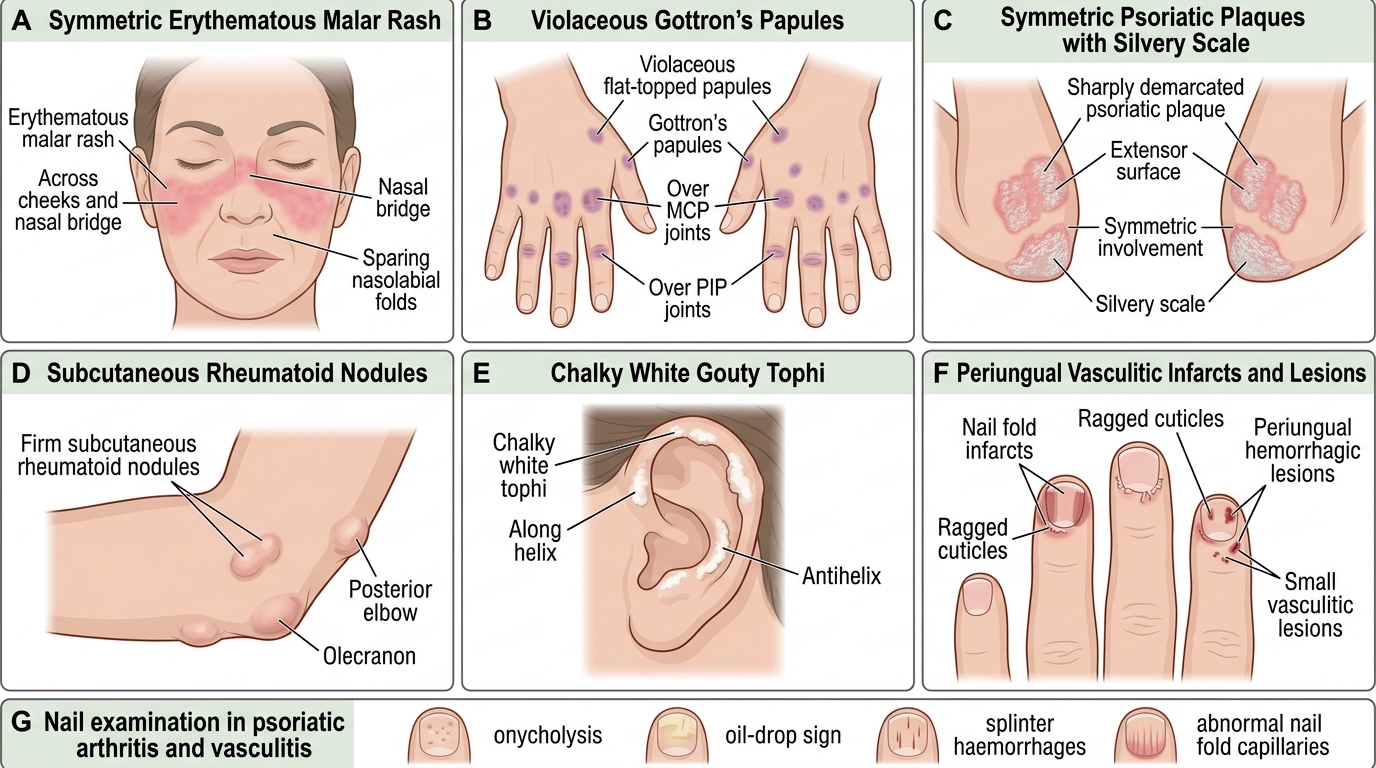
- Face: malar rash (SLE) — erythema over cheeks and nasal bridge sparing nasolabial folds; discoid plaques; heliotrope rash over eyelids (dermatomyositis); facial telangiectasia and tight skin (systemic sclerosis)
- Scalp: non-scarring alopecia (SLE — patchy, often at hairline); scarring alopecia (discoid lupus)
- Hands: Gottron's papules (dermatomyositis — violaceous papules over knuckles of MCPs and PIPs); nail fold infarcts (small vessel vasculitis in RA, SLE); nail fold capillary dilatation (dermatomyositis, systemic sclerosis — visible with dermatoscope or even naked eye as dilated loops); sclerodactyly (systemic sclerosis — tight skin binding fingers); digital ulcers (systemic sclerosis, vasculitis); tophi (gout — chalky nodules, ear helix, olecranon)
- Extensor surfaces: psoriatic plaques (pink-red, silvery scale, elbows, knees, scalp, umbilicus); rheumatoid nodules (firm, non-tender, olecranon, dorsum of fingers)
- Shins: erythema nodosum (tender, red nodules — reactive, associated with IBD, sarcoidosis, streptococcal infection, Behçet)
- Oral and genital mucosae: oral ulcers (SLE — painless; reactive arthritis/Behçet — painful); genital ulcers (Behçet disease — painful; reactive arthritis — painless)
Skin and Nail Findings in Rheumatic Diseases
Nail examination:
- Nail pitting (psoriatic arthritis — multiple shallow pits across the nail plate; also in Reiter syndrome)
- Onycholysis (lifting of nail from bed — psoriatic arthritis, also fungal infection)
- Oil-drop sign (salmon-coloured discolouration under the nail — highly specific for psoriatic arthritis)
- Splinter haemorrhages (subungual; vasculitis, endocarditis)
- Nail fold capillaroscopy abnormalities (systemic sclerosis, dermatomyositis)
Proximal muscle power assessment:
Inflammatory myopathy (polymyositis, dermatomyositis) causes symmetric proximal muscle weakness — the patient cannot rise from a chair without using their arms, cannot raise their arms above their head, and cannot climb stairs. Test specifically:
- Ask the patient to rise from a seated position without using their hands
- Ask them to raise both arms above their head
- Test shoulder abduction against resistance (MRC grading 0–5)
- Test hip flexion against resistance (lying supine, raise straight leg against downward pressure)
Proximal weakness with normal sensation (i.e., NOT peripheral neuropathy pattern) and elevated serum creatine kinase (CK) confirms myopathy. The hallmark skin signs (heliotrope rash, Gottron's papules, mechanic's hands — hyperkeratotic cracking skin on the lateral fingers) confirm dermatomyositis.
SELF-CHECK
You examine a 45-year-old woman with a 4-month history of joint pain and fatigue. She has difficulty rising from a chair and raising her arms above her head. On examination, you find violaceous papules over the MCP and PIP knuckles and a faint purple discolouration of her upper eyelids. Which physical sign is PATHOGNOMONIC of her diagnosis?
A. Difficulty rising from a chair
B. Gottron's papules over the knuckles
C. Violaceous eyelid discolouration (heliotrope rash)
D. Proximal shoulder girdle weakness
Reveal Answer
Answer: B. Gottron's papules over the knuckles
Gottron's papules — violaceous (purple-pink) papules over the dorsal surface of the MCP and PIP joints — are pathognomonic of dermatomyositis. They are highly specific for this condition. The heliotrope rash (purple eyelid discolouration) is very characteristic but not considered strictly pathognomonic. Proximal muscle weakness and difficulty rising from a chair are features of any inflammatory myopathy (polymyositis or dermatomyositis) but are not specific. Gottron's papules specifically identify dermatomyositis and are included as a definitive diagnostic criterion.
Interpretation of Findings and Differential Diagnosis Generation
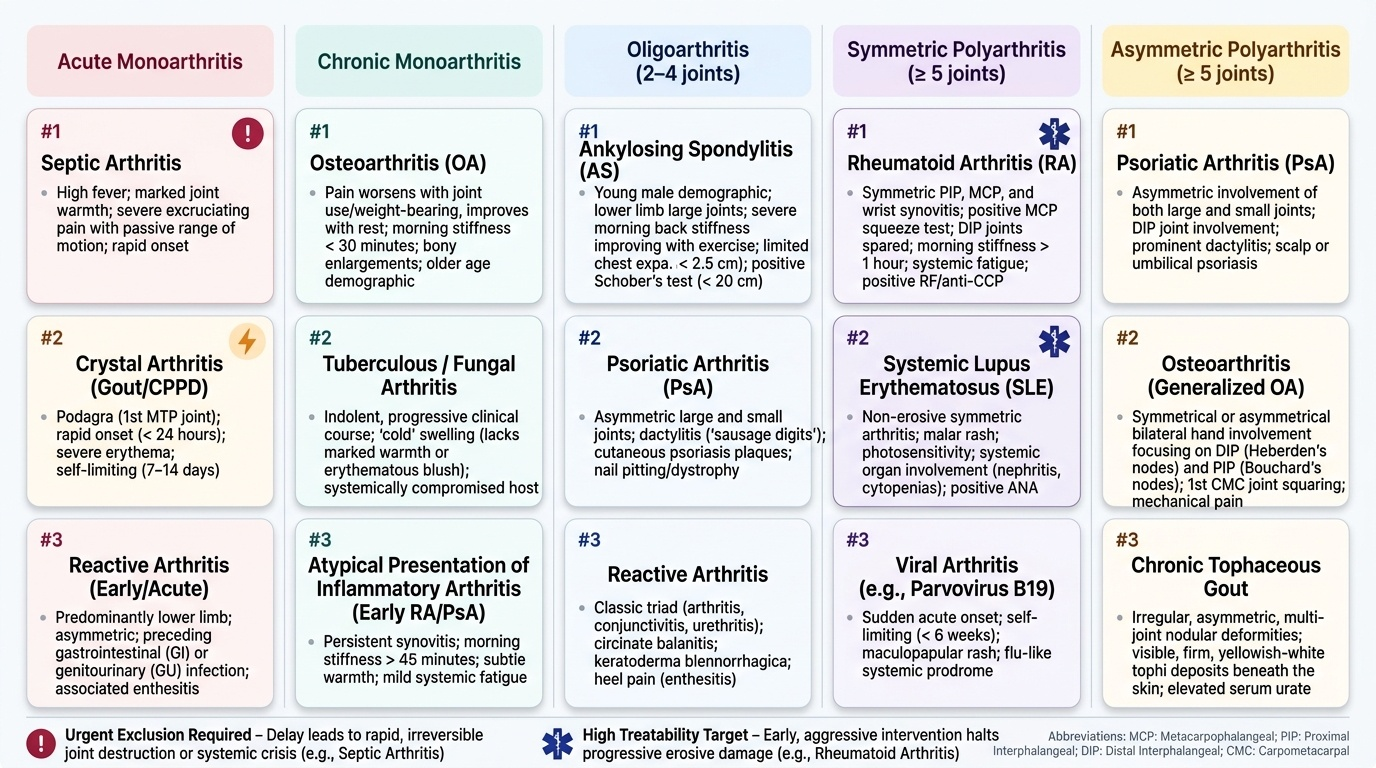
The clinical examination findings must be synthesised with the history to generate a ranked differential diagnosis. This synthesis follows the pattern-recognition approach: match the combined clinical picture (joint pattern + temporal features + extra-articular signs + examination findings) against prototypical disease patterns. The skill of differential diagnosis generation (IM7.10) is not a list-recitation exercise — it is a clinical reasoning skill that applies probability weighting and urgency-ranking to the findings in front of you. In rheumatology, the differential must always prioritise by (a) urgency — septic arthritis and crystal arthritis in acute monoarthritis must be excluded first; and (b) treatability — RA, SLE, and inflammatory myopathy can be treated if recognised early, and delay causes irreversible damage.
Provided image
The approach to differential diagnosis generation follows a structured pattern-recognition matrix. For each case, identify: (1) number of joints; (2) distribution; (3) inflammatory vs mechanical; (4) extra-articular features; (5) patient demographics (age, sex, ethnicity).
Key clinical syndromes and their examination signature:
Rheumatoid arthritis (RA): Symmetric MCP/PIP/wrist synovitis (tender, boggy, warm). Positive MCP squeeze test. Possible ulnar deviation, swan-neck, boutonnière. No DIP involvement (distinguishes from OA and psoriatic arthritis). Possible rheumatoid nodules at olecranon. Morning stiffness >1 hour. Systemic: weight loss, fatigue. Diagnosis confirmed by ACR/EULAR 2010 criteria: joint involvement score + serology (RF/anti-CCP) + acute-phase reactant (CRP/ESR) + duration ≥6 weeks.
Ankylosing spondylitis (AS): Restricted lumbar flexion (Schober's test <20 cm), restricted chest expansion (<2.5 cm), positive occiput-to-wall distance, SI joint tenderness on FABER test. Young male, morning stiffness >1 hour improving with exercise. Possible peripheral oligoarthritis (asymmetric, large joints), enthesitis (Achilles), anterior uveitis.
Septic arthritis: Acute monoarthritis with fever, marked warmth, exquisite tenderness, and inability to move the joint. Any delay in diagnosis is dangerous — synovial fluid culture is the key investigation; treat empirically with antibiotics after arthrocentesis while awaiting culture. Do NOT inject steroids before excluding infection.
Gout: Acute monoarthritis — typically first MTP (podagra), red-hot, extremely tender. Examine for tophi (ear helix, olecranon bursa, Achilles tendon). Precipitating factors: high-purine diet, alcohol, diuretics, dehydration. Synovial fluid: negatively birefringent needle-shaped monosodium urate crystals under polarised light.
SLE: Young woman with butterfly rash, photosensitivity, oral ulcers, non-erosive arthritis (MCPs, PIPs, wrists — Jaccoud's type), alopecia, and urine dipstick showing protein/blood. The SLICC 2012 or ACR/EULAR 2019 classification criteria guide diagnosis (need ≥10 points from clinical and immunological domains). Always check urine in every SLE suspect.
Prioritising the differential — the URGENT list: The following always require same-visit action and should be at the top of any acute joint differential:
- Septic arthritis: fever + acute monoarthritis + inability to weight-bear = arthrocentesis and antibiotics that day
- Crystal arthritis (gout/pseudogout): acute severe monoarthritis with hyperuricaemia history = synovial fluid aspiration for crystal analysis
- Acute haemarthrosis in an anticoagulated patient: immediate drainage if tense
- New or worsening SLE with proteinuria: renal function and urine microscopy urgently — lupus nephritis can progress to CKD rapidly
SELF-CHECK
A 55-year-old woman is referred with knee pain for 8 months. On examination: no warmth, cool small effusion, crepitus on movement, varus deformity, restricted flexion to 90°. No other joints involved. ESR 12 mm/h. Morning stiffness lasts 20 minutes. MCP squeeze test is negative. What is the most likely diagnosis, and what finding most strongly supports it?
A. Rheumatoid arthritis — positive MCP squeeze test
B. Septic arthritis — restricted ROM and effusion
C. Osteoarthritis — cool effusion, crepitus, varus deformity, and short morning stiffness
D. Gout — cool effusion and restricted ROM
Reveal Answer
Answer: C. Osteoarthritis — cool effusion, crepitus, varus deformity, and short morning stiffness
The findings are classic for osteoarthritis: monoarticular involvement of the knee, cool effusion (non-inflammatory synovial fluid), crepitus, varus deformity (medial compartment OA), restricted flexion, normal ESR, and morning stiffness lasting only 20 minutes. The negative MCP squeeze test argues strongly against RA (which would involve small hand joints and produce a positive squeeze). Septic arthritis would cause fever, warmth, inability to weight-bear, and high ESR. Gout at the knee may produce effusion but is typically acute and very painful; ESR would be elevated. The 20-minute morning stiffness is below the 30-minute threshold for mechanical disease.
Documenting and Presenting the Rheumatologic Assessment
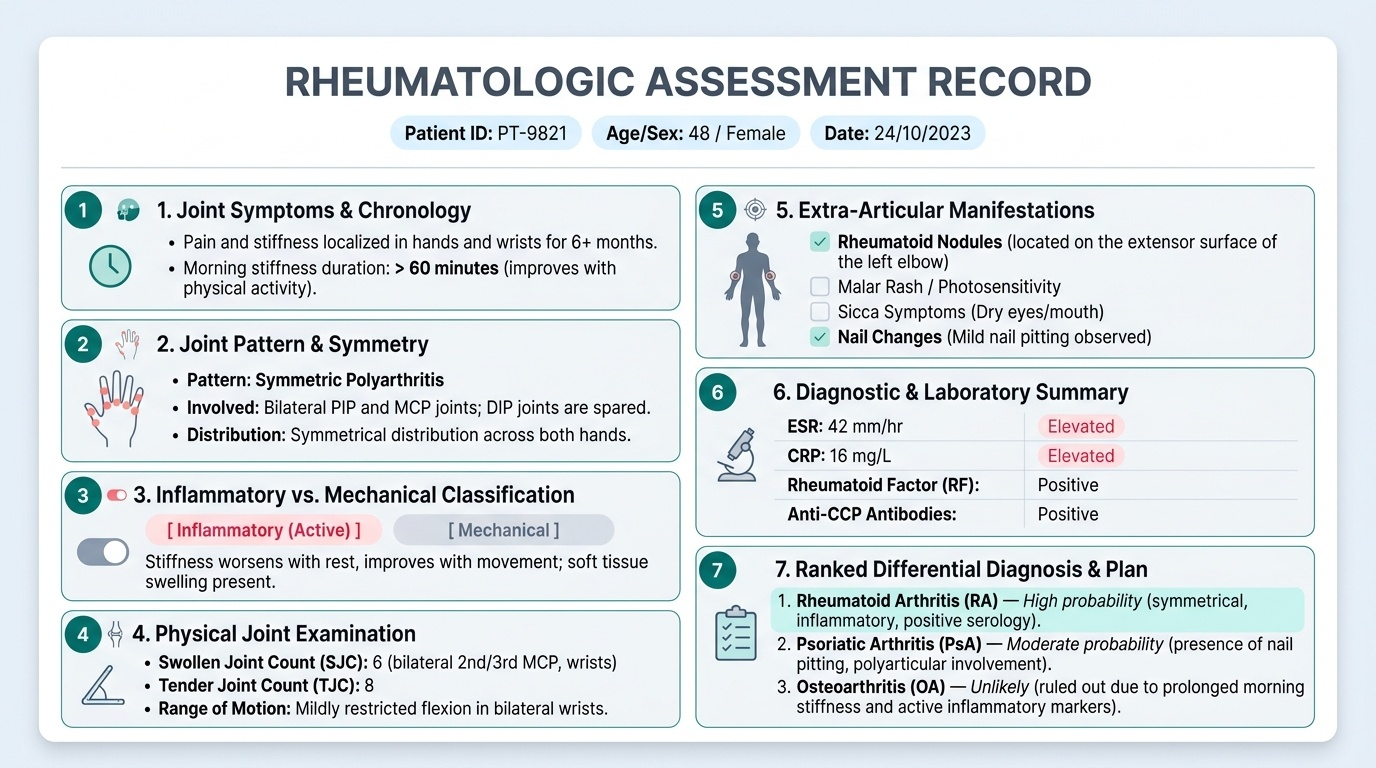
A well-documented rheumatologic history and examination is as much a clinical skill as the examination itself. In teaching hospitals and specialist clinics, the ability to present findings succinctly and accurately — covering joint pattern, inflammatory vs mechanical classification, extra-articular features, and a ranked differential — is the test of whether the student has integrated the knowledge from this module into clinical practice. The format below is the standard structure for documenting a rheumatologic assessment in a case record or presenting to a senior clinician.
Provided image
Documentation of the joint examination must include: the number and identity of joints involved, whether the distribution is symmetric or asymmetric, the presence of warmth/swelling/tenderness at each joint, the nature of swelling (effusion vs synovial thickening vs bony enlargement), range of motion at each involved joint, and any specific signs (deformities, enthesitis, dactylitis, sacroiliac tenderness, Schober's test result).
A model presentation structure for a rheumatologic case:
1. Demography and presenting complaint: 'This is a 35-year-old woman presenting with a 3-month history of bilateral hand and wrist pain with stiffness'
2. Joint pattern summary: 'She has symmetric small-joint polyarthritis involving the MCPs, PIPs, and wrists bilaterally — no DIP involvement'
3. Inflammatory characterisation: 'Morning stiffness lasts 2 hours daily, and pain improves with use — consistent with inflammatory arthritis'
4. Extra-articular features: 'No rash, no oral ulcers, no uveitis, no dry eyes — systemic connective tissue disease features absent'
5. Examination summary: 'MCP squeeze test positive bilaterally; MCP 2 and 3 of the right hand show boggy synovial thickening and warmth; no ulnar deviation or deformity at this stage'
6. Differential and priority: 'Working diagnosis is early seropositive RA; SLE arthritis is less likely given absent systemic features. Urgent exclusion of septic arthritis is not required as the picture is polyarticular and subacute.'
7. Proposed investigations: 'RF, anti-CCP, ESR, CRP, CBC, ANA; X-rays of hands and wrists'