Page 9 of 23
IM7.11-13 | Rheumatologic Diagnostic Testing — SDL Guide
Learning Objectives
- Describe the diagnostic workup appropriate to each clinical hypothesis in rheumatologic disease (IM7.11)
- Enumerate the indications for and interpret CBC, anti-CCP, RF, ANA, anti-dsDNA, and other tests of autoimmunity (IM7.11)
- Enumerate the indications for arthrocentesis and interpret synovial fluid analysis including cell count and polarised light crystal microscopy (IM7.12)
- Enumerate the indications for joint plain radiographs and interpret key radiographic findings in RA, OA, gout, and ankylosing spondylitis (IM7.13)
- Apply the three governing principles — pre-test probability, integration, and specificity vs sensitivity — to clinical diagnostic decision-making
INSTRUCTIONS
Rheumatologic diagnostic testing is powerful when applied to a clear clinical hypothesis and dangerous when ordered as a blanket screen. This module trains hypothesis-first test selection, operating-characteristics-based interpretation, and integration of haematology, serology, synovial fluid, and radiographic data into a coherent diagnostic conclusion.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 354 — Rheumatoid Arthritis; Ch. 356 — Systemic Lupus Erythematosus (textbook)
- API Textbook of Medicine, 10th ed. — Diagnostic Approach in Rheumatology (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 26 — Investigation of Joint Disease (textbook)
- ACR/EULAR 2010 Classification Criteria for Rheumatoid Arthritis — Aletaha et al., Arthritis & Rheumatism 2010 (guideline)
- SLICC 2012 Classification Criteria for SLE — Petri et al., Arthritis & Rheumatism 2012 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Meera has ordered a full autoimmune panel on every patient with joint pain for the past year. Her junior colleague, Dr Rajan, has noticed the results are often confusing: three patients with positive ANA have been referred to rheumatology but turn out to have fibromyalgia, thyroid disease, and no connective tissue disease respectively. Two patients with undeniable inflammatory polyarthritis have been reassured for months because their RF was negative. And a patient whose knee aspirate showed rhomboid crystals in synovial fluid was treated for gout until the polarised light microscopy corrected the diagnosis. The problem is not that the tests are wrong — it is that they are being ordered without a clear diagnostic hypothesis, their results are being interpreted outside their clinical context, and the correct test (synovial fluid analysis) was ordered too late. This module teaches you when to order each rheumatologic diagnostic test, what it means when positive or negative, and how to interpret it in the context of the patient in front of you — not as an isolated number.
WHY THIS MATTERS
NMC competency IM7.11 requires that you describe the appropriate diagnostic workup based on the presumed aetiology and enumerate the indications for and interpret the results of complete blood count (CBC), anti-CCP, RF, ANA, anti-DNA, and other tests of autoimmunity. IM7.12 requires knowledge of the indications for arthrocentesis. IM7.13 requires you to enumerate indications for and interpret plain radiographs of joints — an SH-level competency requiring supervised practice. Together, these three competencies form the diagnostic bridge between the clinical impression generated by history and examination and the confirmed diagnosis that guides treatment. Ordering tests without a hypothesis wastes resources, creates anxiety, produces false-positive results that trigger unnecessary investigations, and delays the correct diagnosis. This module trains you to use rheumatologic diagnostics as hypothesis-confirmation tools — ordered after a clinical impression is formed, interpreted against pre-test probability, and acted upon only in clinical context.
RECALL
Before proceeding, recall the key clinical patterns from the previous module. Inflammatory vs mechanical joint disease is distinguished primarily by history — morning stiffness duration, response to exercise, and extra-articular features. The compartment-based differential generates the hypothesis before any investigation is ordered: symmetric small-joint polyarthritis with prolonged morning stiffness points to RA; acute severe monoarthritis points to crystal arthropathy or septic arthritis; axial pain with sacroiliac involvement points to spondyloarthropathy; multisystem disease in a young woman points to SLE. The investigations in this module are designed to confirm these clinical hypotheses, not to generate them from scratch. Also recall that most rheumatologic autoantibodies have imperfect sensitivity and specificity — a positive result is meaningful only when the pre-test probability is appropriate, and a negative result does not exclude a diagnosis when the clinical picture is compelling.
Clinical Indication and Relevance of Rheumatologic Diagnostic Tests
Rheumatologic diagnostic testing is indicated after the clinical history and examination have generated a working hypothesis. The tests serve four distinct purposes: (1) confirmation of a suspected diagnosis to a level of certainty required to initiate disease-modifying therapy, (2) severity and prognostic assessment (e.g., anti-CCP titre in RA correlates with erosive disease), (3) baseline measurement before starting immunosuppressive therapy (CBC, renal function, liver function before methotrexate; QUANTIFERON-TB before biologics), and (4) monitoring disease activity and drug toxicity during treatment (ESR, CRP, CBC at intervals). Initiating disease-modifying therapy on an autoimmune hypothesis is not a benign decision — methotrexate causes hepatotoxicity and teratogenicity, biologics reactivate latent TB and increase infection risk, and high-dose corticosteroids cause iatrogenic Cushing syndrome. The diagnostic tests serve as gatekeepers that ensure treatment is given to the right patient for the right disease.
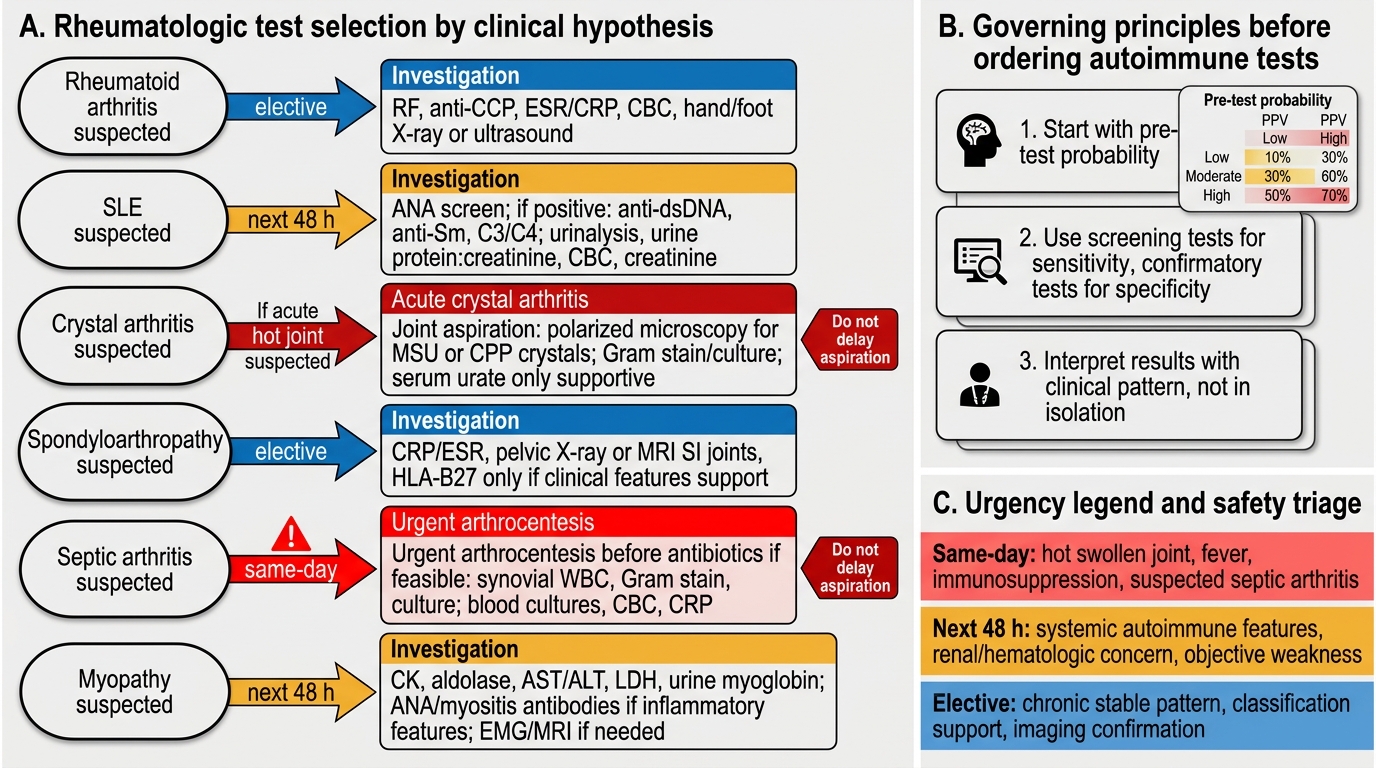
The appropriate diagnostic workup varies by the clinical hypothesis:
- Suspected RA: RF, anti-CCP antibody, ESR, CRP, CBC, renal function, liver function (before therapy), X-rays of hands and feet (look for erosions)
- Suspected SLE: ANA (screen), anti-dsDNA (specific), anti-Sm (specific), complement C3 and C4, CBC with differential (lymphopenia), urinalysis with microscopy (proteinuria, haematuria, casts), renal function
- Suspected crystal arthropathy: synovial fluid aspiration with polarised light microscopy; serum uric acid (note: may be normal during acute gout attack — see below); X-ray of affected joint (chondrocalcinosis in CPPD)
- Suspected spondyloarthropathy: plain X-ray of sacroiliac joints (anteroposterior view), ESR/CRP, HLA-B27 (not diagnostic alone — 8% of the healthy Indian population is HLA-B27 positive, so a positive result must be interpreted in context), HLAB27 is most useful when the pre-test probability is intermediate
- Suspected septic arthritis: synovial fluid urgent Gram stain, culture, and sensitivity; blood cultures; CBC; CRP; serial joint X-rays (late destruction) or MRI (early, sensitive)
- Suspected inflammatory myopathy: serum creatine kinase (CK), aldolase, LDH; anti-Jo-1 and myositis-specific antibodies panel; EMG; muscle biopsy (gold standard); MRI of affected muscle groups
Rheumatologic Test Selection Decision Tree
Governing Principles of Rheumatologic Autoimmune Testing
Three governing principles must be applied to every rheumatologic autoimmune test result. Failure to apply these principles causes both over-diagnosis and under-diagnosis and has been responsible for significant patient harm in rheumatology practice.
Provided image
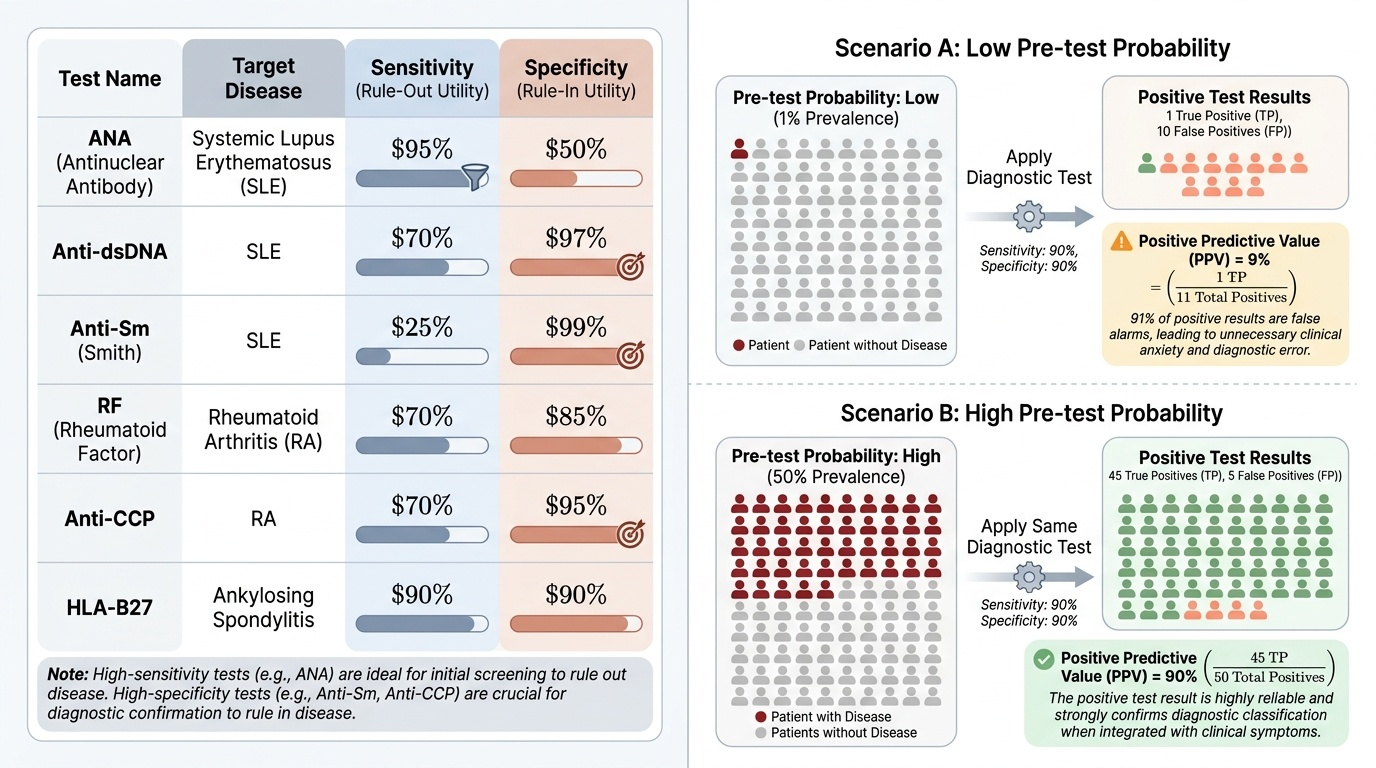
Principle 1: Pre-test probability determines the clinical value of the result. The sensitivity and specificity of a diagnostic test are fixed properties of the test. But the positive predictive value (PPV) — the probability that a positive test means the disease is present — depends critically on the prevalence of the disease in the population being tested (the pre-test probability). ANA is present in 95% of SLE patients (high sensitivity), but it is also positive in approximately 5–10% of the healthy population, in patients with thyroid disease, hepatitis, and fibromyalgia, and in drug-induced lupus. If you test an unselected outpatient population for ANA as a screening tool, most positive results will be false positives — because the pre-test probability of SLE in an unselected clinic population is very low. ANA should be ordered only when the clinical picture raises the probability of SLE to an intermediate or high level — multisystem features, arthritis, rash, renal disease, or cytopenias in a young woman. A positive ANA in a patient with fibromyalgia and no other SLE features is a red herring that leads to unnecessary referrals, patient anxiety, and repeat testing.
Principle 2: No single autoimmune test is diagnostic — use clinical + laboratory integration. No rheumatologic autoimmune test, in isolation, confirms a diagnosis. Diagnosis requires meeting classification criteria (ACR/EULAR for RA and SLE; ASAS for spondyloarthropathies) that integrate clinical and laboratory data. A positive RF alone does not diagnose RA — RF is also positive in Sjögren syndrome, SLE, chronic hepatitis C, bacterial endocarditis, and in 5% of the healthy population. A positive anti-CCP in the context of symmetric MCP/PIP syarthritis, elevated CRP, and morning stiffness >1 hour is meaningful. The same anti-CCP result in a patient with shoulder tendinitis and no other features is not. Integration, not isolation, is the rule.
Principle 3: Specificity is for confirmation; sensitivity is for screening. Use high-sensitivity, low-specificity tests (ANA, RF, ESR) to screen when the pre-test probability is low-to-intermediate — a negative result is useful to rule out. Use high-specificity tests (anti-dsDNA, anti-Sm for SLE; anti-CCP for RA; polarised light microscopy for crystal arthropathy) to confirm when the pre-test probability is moderate-to-high — a positive result is clinically meaningful.
Haematological Tests and Autoantibodies: Indications and Interpretation
This section provides the interpretation framework for each of the specific tests named in IM7.11, ordered from least to most specific for their respective conditions. Understanding each test's operating characteristics — when it is useful, when it is misleading, and what a positive result actually means — is the core clinical knowledge this competency requires.
Complete blood count (CBC) in rheumatologic disease: CBC is ordered as part of the baseline workup for almost all rheumatologic conditions and as a pre-treatment assessment before immunosuppressive therapy. Key abnormalities to seek: anaemia — the most common finding in chronic inflammatory disease is normocytic normochromic anaemia of chronic disease (ACD), also called anaemia of chronic inflammation; it results from inflammatory cytokine-mediated sequestration of iron within reticuloendothelial cells. SLE causes direct autoimmune haemolytic anaemia (positive Coombs test) and anaemia of renal disease. Lymphopenia (<1,000/μL) is one of the SLICC 2012 classification criteria for SLE and is not seen in RA or spondyloarthropathies. Thrombocytopenia in SLE may be immune-mediated (similar to ITP) or associated with antiphospholipid syndrome. Neutropenia can occur in Felty syndrome (RA + splenomegaly + neutropenia). Leucocytosis suggests infection (including septic arthritis) or drug-induced changes (corticosteroids cause leucocytosis as a normal pharmacological effect).
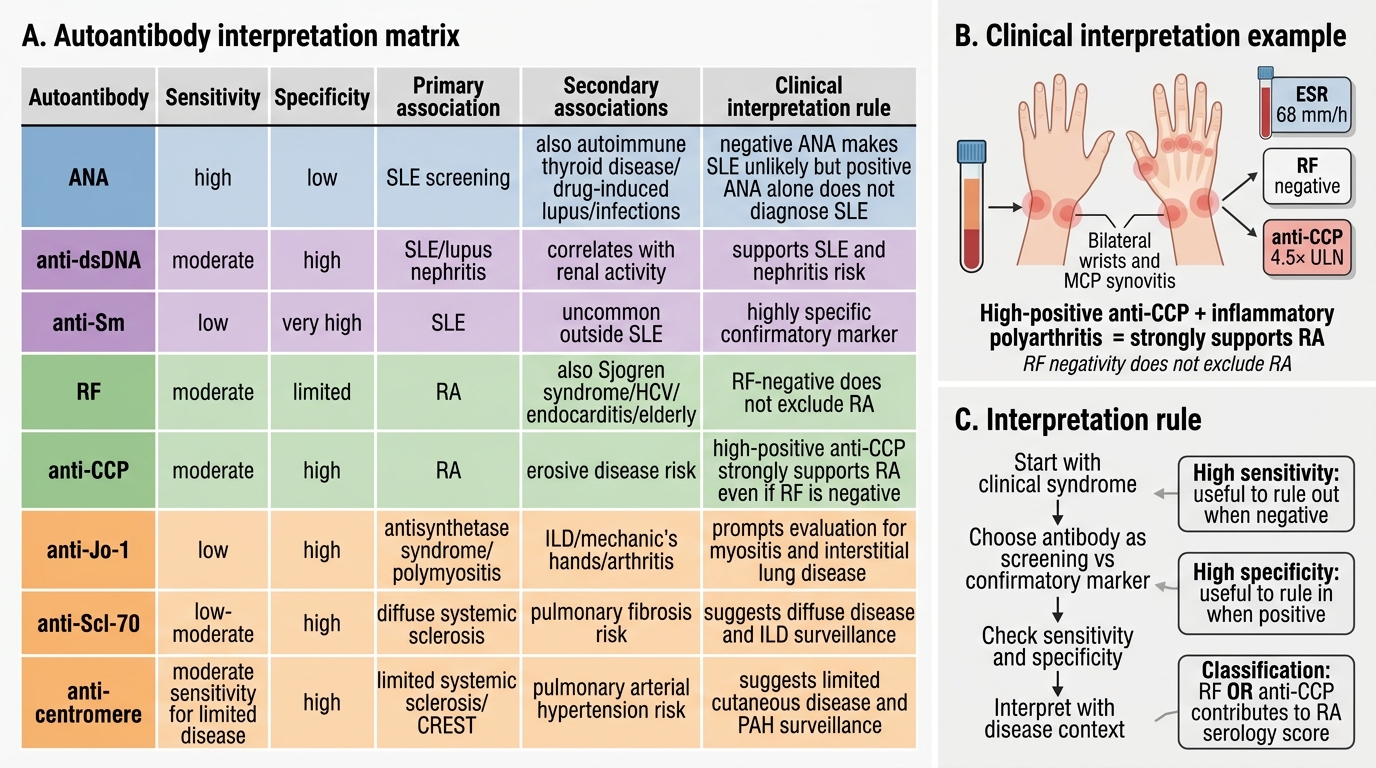
Rheumatoid factor (RF): RF is an IgM (occasionally IgG or IgA) autoantibody directed against the Fc portion of IgG. It is present in approximately 70–80% of RA patients. However, its specificity is limited — RF is also positive in: Sjögren syndrome (70–90% positive), SLE (30%), chronic hepatitis C (up to 40%), bacterial endocarditis, chronic infections, sarcoidosis, and in approximately 5% of healthy individuals over 60 years of age. A positive RF must always be interpreted in the clinical context — RF alone does not diagnose RA. A high-titre RF (>3× upper limit of normal) is more specific for RA than a weakly positive RF. Seronegative RA (RF negative) accounts for approximately 30% of RA patients — the diagnosis remains clinical in these patients, supported by anti-CCP and the ACR/EULAR 2010 criteria.
Anti-cyclic citrullinated peptide antibody (anti-CCP): Anti-CCP (also called anti-ACPA — anti-citrullinated protein antibody) is produced against citrullinated residues on proteins that form when arginine is converted to citrulline by peptidyl arginine deiminase enzymes within the inflamed joint. The critical clinical value of anti-CCP over RF is its superior specificity: anti-CCP has a specificity of approximately 95–98% for RA at standard cut-offs (compared with ~80% specificity for RF). This means that a positive anti-CCP is a much stronger indicator of RA than a positive RF. Furthermore, anti-CCP is positive in approximately 50% of patients who are RF-negative, increasing the overall diagnostic yield when both tests are combined. Anti-CCP can be detected 5–10 years BEFORE the clinical onset of RA — it is a preclinical biomarker that may appear during the 'at-risk' phase. A high-titre anti-CCP (>3× upper limit) is associated with erosive, more aggressive disease and predicts greater structural damage. Anti-CCP is used in the ACR/EULAR 2010 scoring system: a high-positive anti-CCP scores 3 points (the maximum in the serology domain).
Antinuclear antibody (ANA): ANA is a group of autoantibodies directed against components of the cell nucleus — DNA, histones, ribonucleoproteins. The test is performed by indirect immunofluorescence (IIF) on HEp-2 cells; results are reported as a titre and a pattern (homogeneous, speckled, nucleolar, peripheral/rim). ANA sensitivity for SLE is 95–98% — a negative ANA makes SLE highly unlikely (negative predictive value >95% in a clinically suspected case). However, ANA specificity is only 57–74% — many conditions produce a positive ANA without SLE, including drug-induced lupus (isoniazid, hydralazine, procainamide, minocycline, TNF-inhibitors), Sjögren syndrome, systemic sclerosis, mixed connective tissue disease (MCTD), autoimmune hepatitis, thyroid disease, and a low titre (≤1:80) in 5–15% of the healthy population. Therefore: (1) ANA is an excellent screening test for SLE in a patient with suggestive clinical features; (2) a positive ANA must always be followed by more specific antibodies (anti-dsDNA, anti-Sm) before diagnosing SLE.
Anti-double-stranded DNA antibody (anti-dsDNA): Anti-dsDNA is highly specific for SLE (specificity 97%) but less sensitive (sensitivity 57–70%). Anti-dsDNA titre correlates with disease activity — rising anti-dsDNA and falling complement (C3, C4) precede lupus nephritis flare and are used as monitoring biomarkers. Anti-dsDNA is part of the SLICC 2012 and ACR/EULAR 2019 SLE classification criteria. A persistently positive anti-dsDNA in a patient who does not yet meet full classification criteria is a prognostic warning of future SLE development.
Anti-Smith (anti-Sm) antibody: Anti-Sm is directed against the Smith antigen (a non-histone nuclear protein). It has very high specificity for SLE (~99%) but low sensitivity (~25–30%). A positive anti-Sm is essentially diagnostic of SLE when present in a clinical context consistent with the diagnosis. Anti-Sm and anti-dsDNA positivity together provide essentially diagnostic-level certainty for SLE.
Other autoimmune tests (selected): Anti-Ro (SS-A) and anti-La (SS-B) — Sjögren syndrome, subacute cutaneous lupus, neonatal lupus; anti-Scl-70 (anti-topoisomerase I) — systemic sclerosis (diffuse); anti-centromere — limited systemic sclerosis (CREST syndrome); anti-Jo-1 — dermatomyositis/polymyositis with lung involvement; antiphospholipid antibodies (anticardiolipin, anti-β2-glycoprotein I, lupus anticoagulant) — antiphospholipid syndrome (thrombosis, pregnancy loss).
Rheumatologic Autoantibody Interpretation Matrix
SELF-CHECK
A 26-year-old woman presents with 3 months of bilateral wrist and MCP joint pain, morning stiffness lasting 90 minutes, and an ESR of 68 mm/h. RF is negative. Anti-CCP is positive at 4.5× the upper limit of normal. What is the correct interpretation?
A. The diagnosis of RA is excluded because RF is negative
B. Anti-CCP positivity alone confirms RA even without RF
C. High-positive anti-CCP in the context of inflammatory polyarthritis strongly supports RA — seronegative RF does not exclude the diagnosis
D. Both RF and anti-CCP must be positive to classify a patient as having RA by ACR/EULAR 2010 criteria
Reveal Answer
Answer: C. High-positive anti-CCP in the context of inflammatory polyarthritis strongly supports RA — seronegative RF does not exclude the diagnosis
Seronegative RA (RF-negative) accounts for approximately 30% of RA patients. The ACR/EULAR 2010 criteria score the serology domain using either RF or anti-CCP — a high-positive anti-CCP (≥3× ULN) scores 3 points in the serology domain, the maximum score. In this patient, with bilateral MCP/wrist synovitis, morning stiffness >1 hour, elevated ESR, and high-positive anti-CCP, the ACR/EULAR 2010 score is ≥6 = definite RA, regardless of RF negativity. Anti-CCP has superior specificity (~97%) compared to RF (~80%) and is the more diagnostically valuable antibody in seronegative patients.