Page 10 of 23
IM7.11-13 | Rheumatologic Diagnostic Testing — SDL Guide (Part 2)
Arthrocentesis: Indications, Technique, and Synovial Fluid Analysis
Arthrocentesis (joint aspiration) is the direct sampling of synovial fluid from a joint and represents the definitive diagnostic procedure for acute monoarthritis, crystal arthropathy, and suspected septic arthritis. No other clinical or laboratory finding can replace synovial fluid analysis in these conditions. The IM7.12 competency requires knowledge-level understanding of the indications for arthrocentesis — students are not expected to perform the procedure independently at undergraduate level, but must know when it is indicated and how to interpret the results, and must have observed the procedure under supervision. The key principle governing the decision to aspirate is clinical urgency: when a joint is acutely inflamed and the cause is unknown, the risk of missing septic arthritis — which destroys cartilage within 48–72 hours and can cause permanent joint destruction or septicaemia — far outweighs the minor discomfort and small procedural risk of arthrocentesis. The adage 'aspirate any joint you cannot clinically explain' reflects this calculus. Identifying crystals under polarised light microscopy can also prevent the over-diagnosis of septic arthritis and unnecessary prolonged antibiotic therapy in crystal arthropathy patients. The procedure is performed under sterile conditions with local anaesthetic infiltration of the overlying skin before needle insertion into the joint space; the synovial fluid obtained is immediately divided into three samples — culture bottle (for microbiological analysis), EDTA tube (for cell count and differential), and a plain glass slide for crystal preparation and polarised light microscopy.
Indications for arthrocentesis:
1. Acute monoarthritis with fever — septic arthritis must be excluded by Gram stain and culture of synovial fluid; this is a same-day emergency indication. Any delay increases the risk of irreversible joint destruction.
2. Acute severe monoarthritis without systemic features (possible crystal arthropathy) — polarised light microscopy for crystal identification
3. New large joint effusion of unknown cause — diagnostic workup for inflammatory vs non-inflammatory vs haemorrhagic effusion
4. Therapeutic drainage — large tense effusion causing pain and restricted ROM (e.g., haemarthrosis, massive OA effusion)
5. Intra-articular injection of corticosteroid — only after septic arthritis is excluded
Contraindications: Overlying skin infection (relative — route around the cellulitis); coagulopathy (relative — use caution, correct INR if >2.0); prosthetic joint (refer to orthopaedics — higher infection risk with inoculation).
Synovial fluid analysis — normal reference values and interpretation:
| Parameter | Normal | Non-inflammatory (Group I) | Inflammatory (Group II) | Septic (Group III) | Crystal (Group II-III) |
|---|---|---|---|---|---|
| Appearance | Clear, yellow | Clear, yellow | Turbid, yellow | Purulent, cloudy | Turbid, yellow |
| WBC count (cells/μL) | <200 | 200–2,000 | 2,000–50,000 | >50,000 (often >100,000) | 5,000–50,000 |
| PMN % | <25% | <25% | >50% | >90% | >70% |
| Glucose | ≈ serum | ≈ serum | Slightly low | <50% serum (low) | Variable |
| Protein | Low | Slightly elevated | Elevated | Very elevated | Elevated |
| Culture/Gram stain | Negative | Negative | Negative | Positive (70–90%) | Negative |
| Crystals | None | None | None | None | Present |
Crystal identification under polarised light microscopy:
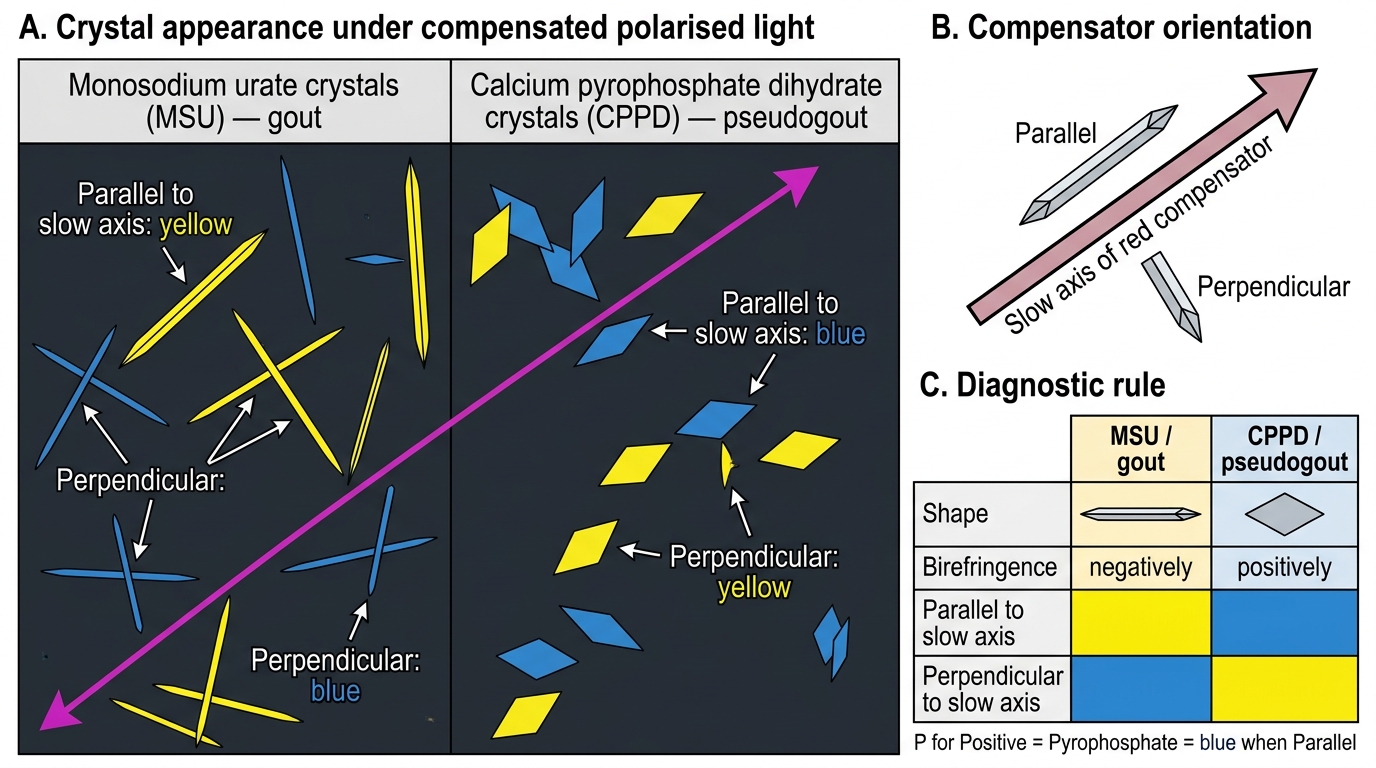
- Monosodium urate (MSU) crystals — Gout: Needle-shaped, long (2–10 μm), sharply pointed. Under compensated polarised light: negatively birefringent — appear YELLOW when their long axis is parallel to the slow axis of the first-order red compensator, and BLUE when perpendicular. This is the most tested fact in rheumatology — memorise: 'Gout = Negative = Yellow when parallel.'
- Calcium pyrophosphate dihydrate (CPPD) crystals — Pseudogout: Rhomboid-shaped, smaller (1–5 μm), with blunt ends. Under compensated polarised light: positively birefringent — appear BLUE when their long axis is parallel to the compensator's slow axis, YELLOW when perpendicular. Mnemonic: 'CPPD = Positive = Blue when parallel.'
Serum uric acid interpretation trap: Serum uric acid levels often fall during an acute gout attack due to increased renal uric acid excretion triggered by the inflammatory stress response. A normal or even low serum uric acid during the acute attack does NOT exclude gout — synovial fluid crystal analysis is the definitive diagnostic test.
Compensated Polarised Light Microscopy: MSU vs CPPD Crystals
SELF-CHECK
A 65-year-old woman with hypertension presents with a 3-day history of a swollen, hot, painful right knee. She is afebrile. Arthrocentesis yields turbid fluid. Under compensated polarised light microscopy, crystals appear BLUE when their long axis is parallel to the slow axis of the compensator. What is the crystal type and diagnosis?
A. Monosodium urate crystals — gout (negatively birefringent)
B. Calcium pyrophosphate dihydrate crystals — pseudogout (positively birefringent)
C. Calcium hydroxyapatite crystals — Milwaukee shoulder syndrome
D. Cholesterol crystals — chronic inflammatory arthritis
Reveal Answer
Answer: B. Calcium pyrophosphate dihydrate crystals — pseudogout (positively birefringent)
Crystals that appear BLUE when their long axis is parallel to the compensator's slow axis are POSITIVELY birefringent. Positively birefringent crystals in joint fluid are calcium pyrophosphate dihydrate (CPPD) — the diagnosis is pseudogout. CPPD crystals are rhomboid in shape (blunt ends), in contrast to the needle-shaped gout crystals. The memory rule: 'P for Positive = P for Pyrophosphate (CPPD) = Blue when Parallel.' Monosodium urate crystals in gout are negatively birefringent (yellow when parallel — 'Negative = Yellow when parallel'). Pseudogout typically affects middle-aged to elderly patients and is more common in large joints (knee, wrist) compared with classic podagra gout at the first MTP joint.
Plain Radiograph Interpretation in Joint Disease
Plain radiographs of joints are the primary imaging investigation for all chronic joint diseases and provide structural information that complements the clinical and serological assessment. The IM7.13 competency requires that students enumerate the indications for joint X-rays and interpret them — an SH-level skill requiring supervised practice at the radiograph viewing box or a PACS workstation. Plain radiographs are indicated at baseline in suspected RA, OA, crystal arthropathy, and spondyloarthropathy; at intervals during follow-up to detect disease progression; and urgently to exclude fracture, dislocation, or osteomyelitis when clinical features demand it. Radiographs of the hands and feet (anteroposterior views) are the standard initial series in RA because these joints contain the smallest bones and the earliest erosive changes are most visible here. Sacroiliac joint X-rays (an anteroposterior pelvis view adequately demonstrates both SI joints) are the first-line imaging study in suspected ankylosing spondylitis. The important limitation of plain radiography is that it detects only bony changes — cartilage loss, synovitis, and early erosions are not visible until structural damage has already occurred; MRI detects synovitis, bone marrow oedema, and early erosions 2–3 years before they become visible on X-ray and is therefore more sensitive for early RA and early sacroiliitis. The following systematic approach to joint X-ray interpretation should be applied to every film: assess in order — soft tissues, bone density, joint space, bone surface (periarticular bony changes), and any specific diagnostic features. The SOFTER mnemonic provides a reliable sequence.
SOFTER mnemonic for systematic joint X-ray interpretation:
- S — Soft tissues (swelling, calcification, tophi)
- O — Osteoporosis (periarticular osteopenia — RA; or diffuse — systemic corticosteroid use)
- F — Findings at joint space (narrowing, widening, or preservation)
- T — Texture of bone (osteophytes, erosions, cysts, sclerosis)
- E — Erosions (RA, psoriatic arthritis — marginal; OA — subchondral)
- R — Relationship of bony surfaces (subluxation, fusion, alignment)
Radiographic features by diagnosis:
Rheumatoid arthritis (RA):
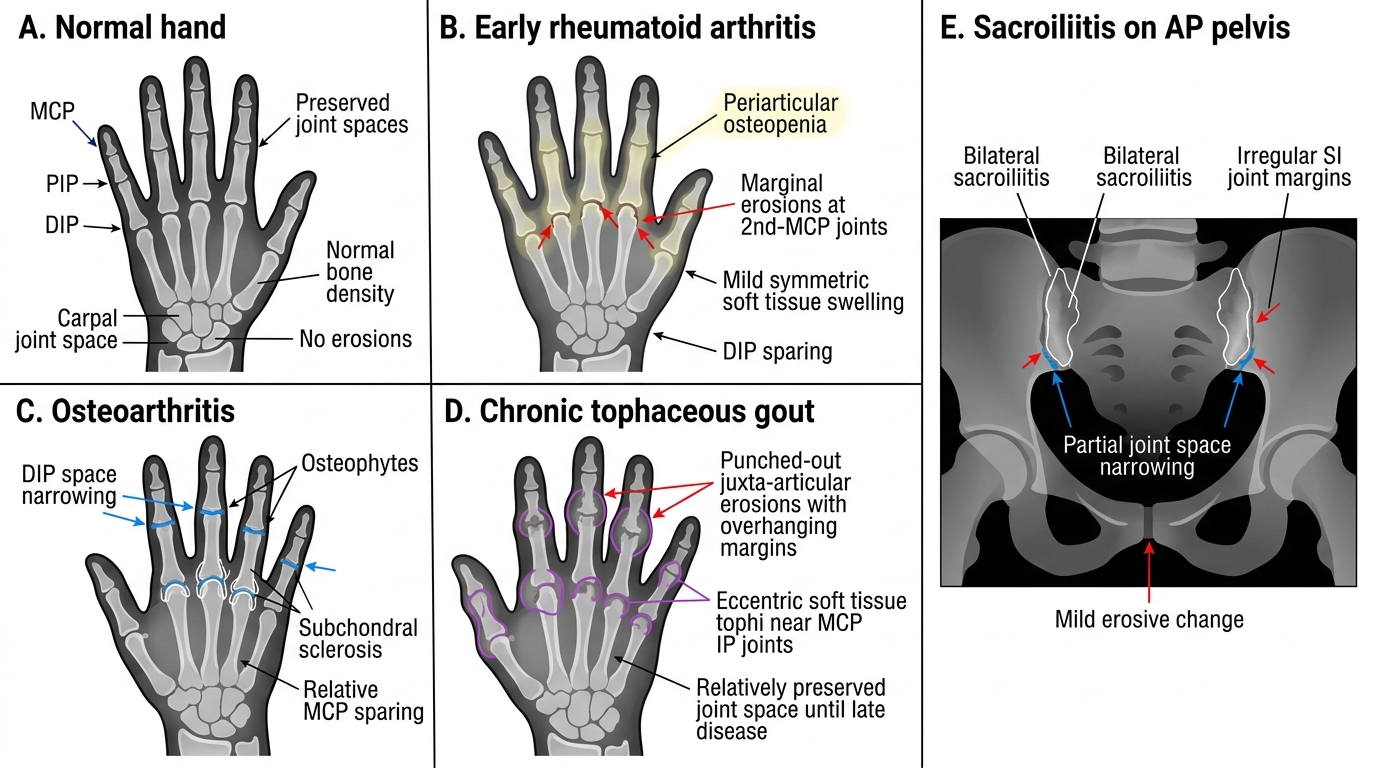
- Periarticular osteopenia: juxta-articular osteoporosis of the metacarpal heads and proximal phalanges — an early sign, visible within weeks of active disease
- Joint space narrowing: uniform narrowing of the joint space, reflecting cartilage loss; typically symmetric and bilateral at the MCPs, PIPs, and wrists
- Erosions: the hallmark of erosive RA — marginal erosions at the 'bare area' (the part of the joint not covered by cartilage, where the pannus erodes bone); best seen at the radial aspect of the 2nd and 3rd MCP joints and ulnar styloid. Erosions are seen in 30% of patients at 2 years and 70% at 10 years without DMARD therapy
- Subluxation and deformity: ulnar deviation, boutonnière, swan-neck (late disease)
- Atlantoaxial subluxation: in severe RA — C1-C2 instability due to destruction of the transverse ligament; potentially catastrophic if the patient undergoes general anaesthesia without cervical spine stabilisation. Detect by lateral cervical flexion X-ray: atlantodental interval >3 mm is abnormal in adults.
- Absent in early RA: X-rays may be completely normal in the first year of inflammatory disease — MRI is more sensitive for early erosions and synovitis
Osteoarthritis (OA):
- Joint space narrowing: non-uniform (asymmetric) in OA, typically greatest at the area of maximum mechanical loading — medial compartment of the knee (varus deformity), superolateral hip
- Subchondral sclerosis: increased radiodensity of the bone directly beneath the narrowed cartilage — reflects bone remodelling under stress
- Osteophytes: bony outgrowths at the joint margins — the radiographic hallmark of OA; present at the tibial plateaux, femoral condyles, acetabular rim, and vertebral endplates (spondylosis)
- Subchondral cysts (geodes): fluid-filled cavities within the subchondral bone, communicating with the joint space through cartilage defects
- No erosions, no periarticular osteopenia: OA does not produce marginal erosions or periarticular bone loss (contrasts with RA)
Gout:
- Soft tissue tophi: radiopaque (slightly denser than soft tissue) tophi near affected joints, especially the first MTP joint and olecranon; occasionally calcified
- Normal early: acute gout attacks do not produce X-ray changes — early disease shows only soft tissue swelling
- Punched-out erosions: in chronic tophaceous gout — well-defined, round or oval erosions with overhanging margins (a 'rat-bite' appearance); occur next to tophi but notably with preserved joint space until late (contrasting with RA where joint space is lost early)
- Preserved joint space (until late): distinctive feature of tophaceous gout — even with multiple erosions, the joint space is preserved because cartilage destruction is less prominent than in RA
Ankylosing spondylitis (sacroiliac joints):
- Sacroiliitis: the earliest and most reliable X-ray sign — bilateral symmetric blurring and irregularity of the SI joint margins, sclerosis (increased density), and eventual erosion and fusion (ankylosis). Graded 0–4 (modified New York criteria Grade 2 or higher bilaterally, or Grade 3-4 unilaterally = positive for sacroiliitis)
- Bamboo spine: late disease — bridging syndesmophytes (vertical ligamentous ossification linking vertebral bodies) creating the characteristic 'bamboo spine' appearance on AP view
- Squaring of vertebral bodies: loss of the normal concave anterior vertebral contour due to periostitis and ossification at the corners (Romanus lesion) — a relatively early sign
Radiographic Patterns in Common Rheumatologic Disorders
Applied Practice: Diagnostic Workup for Common Rheumatologic Scenarios
Applied diagnostic practice in rheumatology means selecting the correct investigations based on the clinical hypothesis, avoiding the common pitfall of ordering an undifferentiated autoimmune panel, and being able to interpret the results in context. The following three diagnostic scenarios illustrate the systematic approach expected at the IM7.11–IM7.13 level. For each scenario, note the hypothesis-first approach: the clinical assessment generates the differential, which directs the investigation selection, which is then interpreted against the pre-test probability.
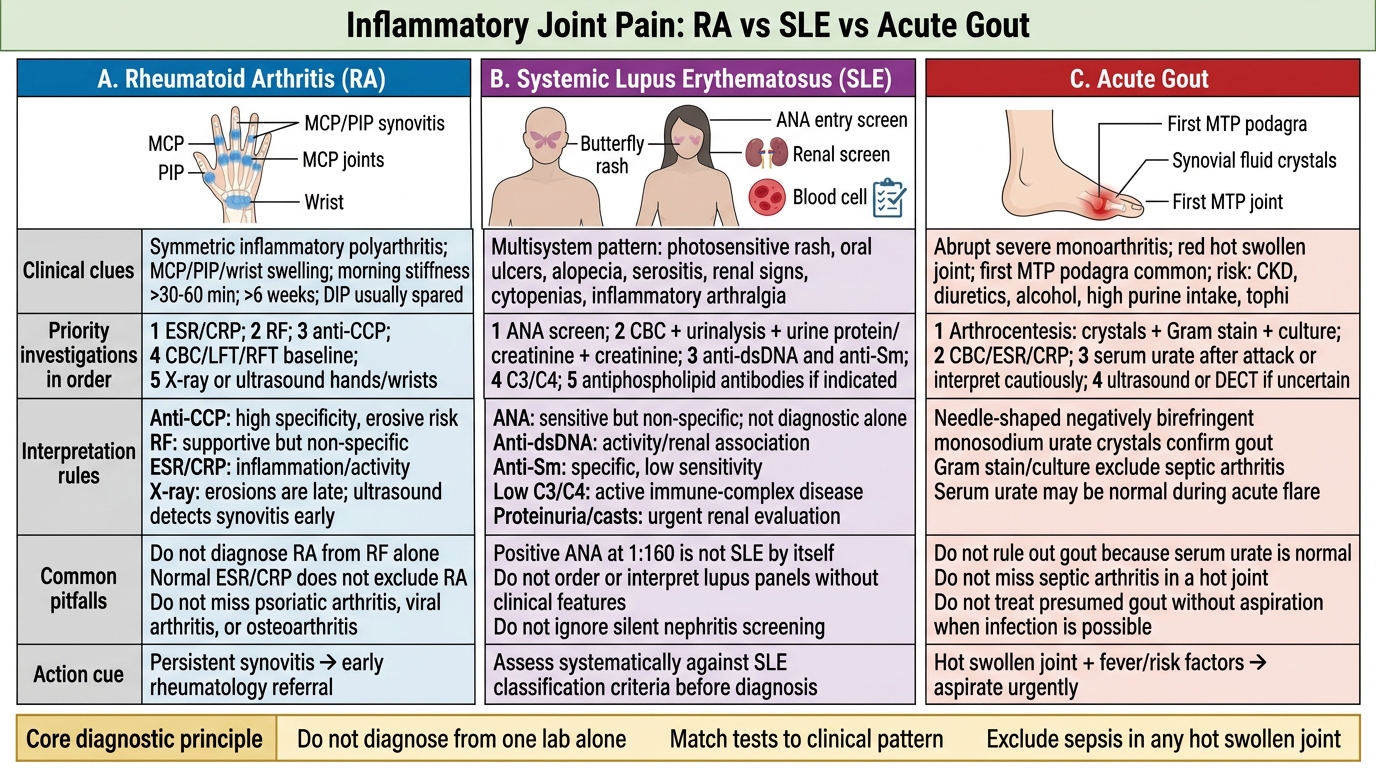
Scenario A — Suspected early RA: A 40-year-old woman presents with 3 months of symmetric MCP and PIP joint pain, DIP sparing, morning stiffness lasting 2 hours, ESR 54 mm/h, CRP 28 mg/L. Working diagnosis: early RA. Investigation plan: (1) RF — ordered because sensitivity for RA is 70–80%; negative does not exclude RA but positive (especially high titre) supports it; (2) anti-CCP — ordered first if resources are limited, because higher specificity than RF; a high-positive result (>3× ULN) scores maximally in ACR/EULAR 2010 criteria; (3) CBC — to assess for anaemia of chronic disease and as a baseline before DMARD initiation; (4) renal and liver function — baseline before methotrexate; (5) plain X-rays of hands and feet (AP view) — to detect erosions early; MRI of hands if X-rays normal but high clinical suspicion (more sensitive); (6) do NOT order ANA or anti-dsDNA as the first-line workup — the clinical picture does not point to SLE, and ANA is frequently positive at low titre in RA patients (up to 30%), creating diagnostic confusion.
Scenario B — Suspected SLE: A 24-year-old woman presents with 2 months of bilateral wrist and MCP joint pain, facial rash after sun exposure, 3 episodes of oral ulcers, and two-plus proteinuria on dipstick. Working diagnosis: SLE. Investigation plan: (1) ANA — the screening test; a negative ANA makes SLE very unlikely; if positive, proceed to specific antibodies; (2) anti-dsDNA — high specificity for SLE, titres correlate with disease activity; (3) anti-Sm — very high specificity, present in ~25% of SLE patients; (4) complement C3 and C4 — reduced in active SLE due to consumption by immune complexes; rising anti-dsDNA + falling C3/C4 = impending flare; (5) CBC with differential — look for lymphopenia, anaemia, thrombocytopenia; (6) urinalysis with microscopy (NOT just dipstick) — red cell casts indicate proliferative glomerulonephritis (lupus nephritis WHO class III or IV); 24-hour urine protein or spot protein:creatinine ratio; (7) renal function; (8) antiphospholipid antibodies (anticardiolipin, anti-β2-GP1, lupus anticoagulant) — if thrombosis history, pregnancy loss, or thrombocytopenia.
Scenario C — Acute monoarthritis: A 58-year-old man on hydrochlorothiazide presents with a 1-day history of severe pain, swelling, and redness in the right first MTP joint. Temperature 37.1°C. Working diagnosis: acute gout (podagra). Priority investigation: (1) arthrocentesis with polarised light microscopy — look for needle-shaped negatively birefringent (yellow when parallel) monosodium urate crystals; (2) Gram stain and culture of synovial fluid — mandatory to exclude septic co-infection; (3) serum uric acid — order but interpret cautiously: may be normal or low during the acute attack due to stress-mediated uricosuria; a normal result does NOT exclude gout; (4) renal function and urine microscopy — urate nephropathy in chronic gout; (5) plain X-ray of the affected joint — assesses for punched-out erosions in chronic tophaceous gout; (6) CBC — elevated WBC supports inflammation; very high WBC (>20,000) with fever should raise concern for co-existing infection.
RA vs SLE vs Acute Gout: Diagnostic Comparison
SELF-CHECK
A 50-year-old woman is referred with a 6-month history of fatigue and arthralgia. Her physician ordered an ANA which returned positive at 1:160 (speckled pattern). She has no rash, no oral ulcers, no photosensitivity, no hair loss, no renal symptoms, and normal CBC. Which is the MOST appropriate next step?
A. Diagnose SLE based on the positive ANA and refer immediately to rheumatology
B. Reassure the patient that a positive ANA at 1:160 is diagnostic of a benign condition
C. Assess clinical features systematically against SLE classification criteria; if insufficient criteria are met, no SLE diagnosis should be made
D. Order anti-dsDNA urgently to confirm SLE
Reveal Answer
Answer: C. Assess clinical features systematically against SLE classification criteria; if insufficient criteria are met, no SLE diagnosis should be made
ANA is a sensitive but non-specific screening test. ANA is positive at low titres (≤1:80) in 5–15% of the healthy population and at various titres in thyroid disease, Sjögren syndrome, fibromyalgia, drug-induced lupus, hepatitis, and many other conditions. A positive ANA at 1:160 is NOT diagnostic of SLE — it only means SLE must be considered and systematically evaluated. The correct next step is to assess the patient against SLE classification criteria (SLICC 2012 or ACR/EULAR 2019): if fewer than 4 criteria are met (or <10 points in ACR/EULAR 2019), SLE cannot be classified. In a patient with only arthralgia and positive ANA without any other features, the diagnosis of SLE should NOT be made. Anti-dsDNA should be ordered to further characterise, but the interpretation must be tied to the clinical picture, not treated as confirmatory in isolation.