Page 3 of 23
IM7.1-7 | Rheumatologic Disease Foundations — SDL Guide (Part 3)
Principles of Management in Rheumatologic Disease
The management of rheumatologic disease has been transformed over the past three decades by the development of targeted therapies that interrupt the cytokine cascade at specific points, enabling disease remission rather than mere symptom control. Understanding the treatment principles for the most important conditions — RA, SLE, gout, seronegative spondyloarthropathies — is a core final-year competency that bridges pharmacology with clinical decision-making. The overarching framework for management follows a treat-to-target (T2T) philosophy: set a specific measurable target (clinical remission or low disease activity), monitor with validated disease activity scores at regular intervals, and escalate therapy at defined timepoints until the target is reached. This approach, first formalised for RA (ACR/EULAR 2010) and now applied across inflammatory arthritis, has demonstrably reduced long-term joint destruction and disability compared with symptom-driven prescribing.
Provided image
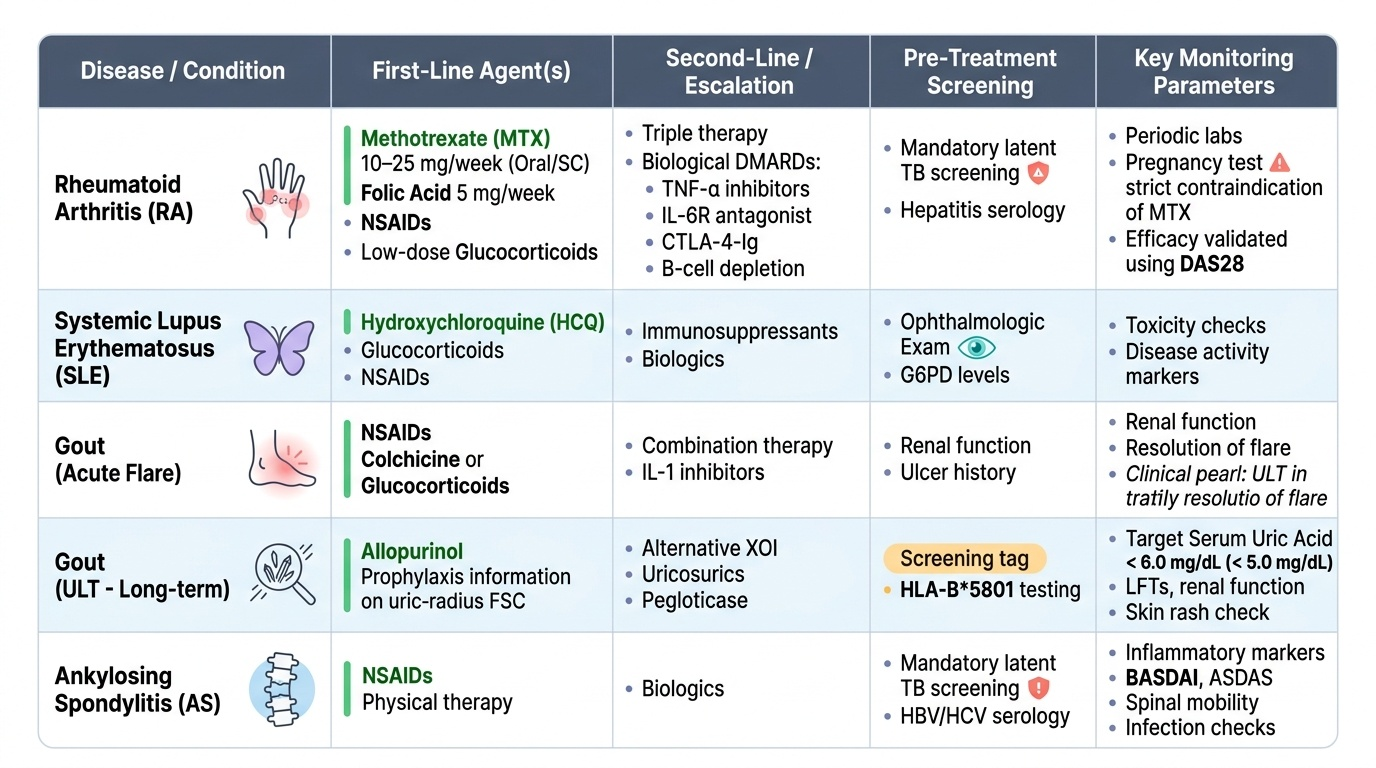
Rheumatoid arthritis — pharmacological management:
- NSAIDs and analgesics: provide symptomatic relief but do not modify disease course or prevent erosions; used as bridging therapy while DMARDs take effect
- Conventional synthetic DMARDs (csDMARDs): methotrexate (MTX) is the cornerstone first-line DMARD — typically 10–25 mg/week oral or subcutaneous, with folic acid supplementation (5 mg/week) to reduce toxicity; takes 6–12 weeks to work; requires baseline and periodic LFT, CBC, renal function; contraindicated in pregnancy (teratogenic)
- Combination csDMARDs: methotrexate + sulfasalazine + hydroxychloroquine (triple therapy) for moderate disease
- Biological DMARDs (bDMARDs): used when csDMARDs fail or are intolerable; TNF-α inhibitors (etanercept, adalimumab, infliximab) are first-line biologics; IL-6 receptor antagonists (tocilizumab) for MTX failure or high inflammatory activity; CTLA-4-Ig (abatacept) for T-cell co-stimulation blockade; B-cell depletion (rituximab) for seropositive RA failing anti-TNF
- Pre-biologic TB screening (mandatory): all patients starting biologics must be screened for latent TB with Mantoux test + CXR (or IGRA) — TNF-α is critical for granuloma maintenance, and anti-TNF therapy can reactivate latent TB; in India, with a high TB burden, this is non-negotiable
- Glucocorticoids: bridging therapy or low-dose maintenance for flares; minimise dose and duration due to osteoporosis, infection, and metabolic risk
SLE management:
- Hydroxychloroquine: given to ALL SLE patients unless contraindicated — reduces flares, improves survival, and reduces thrombotic risk; requires annual ophthalmological monitoring for retinopathy
- Prednisolone: for acute flares and organ-threatening disease; taper to the lowest effective dose
- Immunosuppressives: mycophenolate mofetil or cyclophosphamide for lupus nephritis; azathioprine for maintenance
- Sun protection: mandatory — UV triggers SLE flares via keratinocyte activation and nuclear antigen release
Gout management:
- Acute attack: NSAIDs (first-line, e.g., indomethacin), colchicine (within 24 hours of attack onset — highly effective), or prednisolone (if NSAIDs/colchicine contraindicated — renal impairment)
- Urate-lowering therapy (ULT): allopurinol is first-line (xanthine oxidase inhibitor); target serum urate <6 mg/dL (or <5 mg/dL with tophi); start ULT ONLY after the acute attack has fully settled; NEVER start allopurinol during an acute attack as it prolongs inflammation; febuxostat is an alternative for allopurinol intolerance
Seronegative spondyloarthropathies:
- NSAIDs: first-line for axial disease; regular use reduces progression in ankylosing spondylitis
- Anti-TNF biologics: for NSAID-refractory axial disease (etanercept, adalimumab, infliximab) or peripheral joint disease
- IL-17 inhibitors (secukinumab): effective for ankylosing spondylitis and psoriatic arthritis; preferred in psoriatic skin disease
- DMARDs for peripheral disease: sulfasalazine and methotrexate for peripheral joint involvement in psoriatic arthritis; they are NOT effective for axial disease
Self-Assessment: Applying Rheumatologic Foundations
You have now covered the core foundational concepts of rheumatologic disease — the pathophysiology and genetic basis of autoimmunity, the classification of joint pain by number, distribution, temporal pattern, and inflammatory versus mechanical character, the distinction between articular and periarticular disease, the systemic organ manifestations that extend rheumatologic disease far beyond the joint, and the management principles for the major conditions. The scenarios below consolidate these concepts with clinical vignettes that require you to apply the classification framework before reaching a diagnosis. Work through each scenario carefully: classify the joint disease, identify any systemic manifestations that point to a specific condition, apply the inflammatory-versus-mechanical distinction, and then select the appropriate first management step before reading the analysis. This is the skill level at which NMC final-year IM7 competencies are assessed.
Provided image
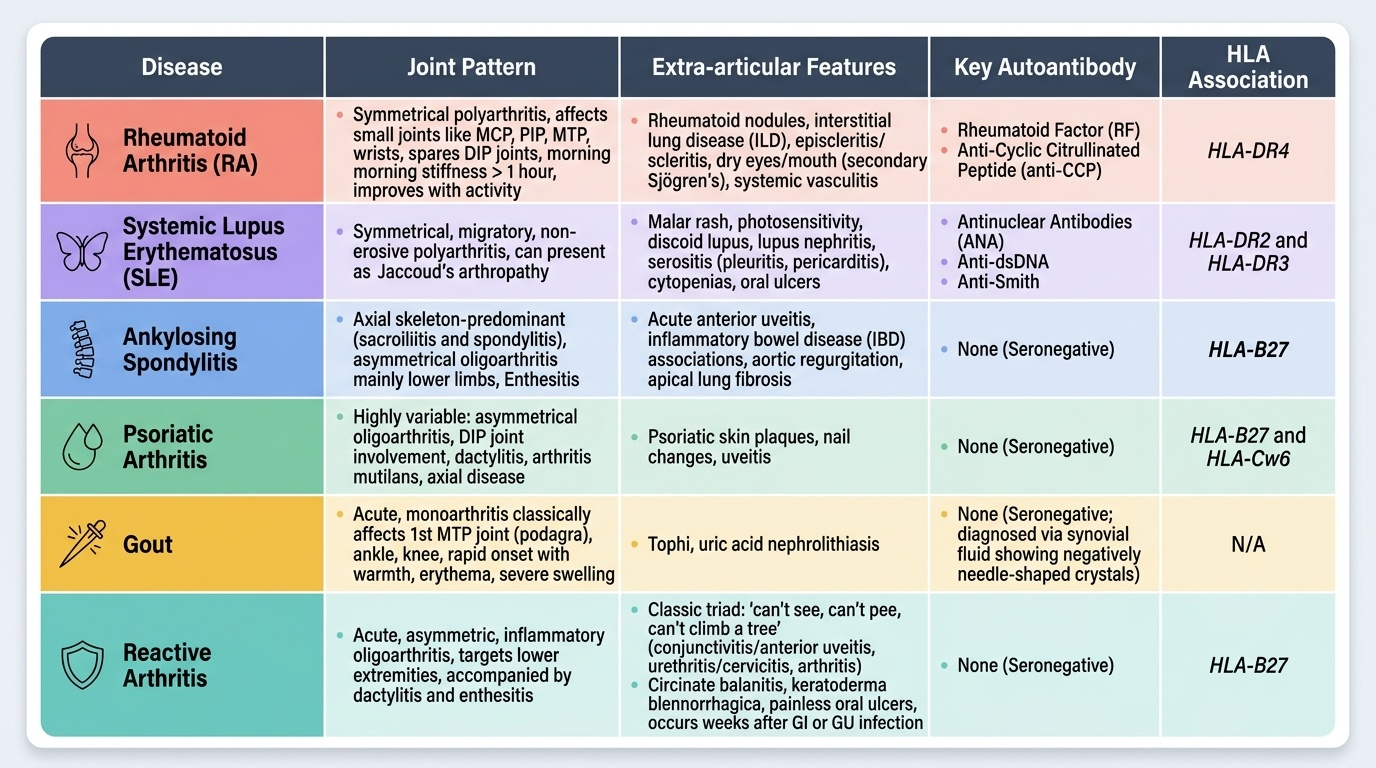
Scenario A: A 55-year-old woman reports 3 years of bilateral knee pain that worsens after walking and climbing stairs. Morning stiffness lasts about 15 minutes. Examination shows bony hard enlargement of both knees, crepitus, no warmth, and small cool effusions. Her DIP joints have hard nodular swellings. ESR is 14 mm/h. Classify: Mechanical/degenerative, polyarticular, chronic. DIP and knee involvement, Heberden's nodes, absent systemic inflammation. Diagnosis: Osteoarthritis. Key teaching: bony swelling (osteophytes) and cool effusions distinguish OA from inflammatory; ESR is normal.
Scenario B: A 40-year-old woman presents with a 6-month history of symmetric swelling of MCP and PIP joints of both hands, morning stiffness >2 hours, fatigue, and weight loss. Her RF is positive at high titre. Classify: Inflammatory, polyarticular, chronic, symmetric small joints. Diagnosis: Seropositive RA (confirm with anti-CCP, X-ray for erosions). First-line treatment: methotrexate (start at 10–15 mg/week with folic acid). Before adding a biologic: screen for latent TB.
Scenario C: A 24-year-old woman presents with a 4-month history of joint pain (wrists, MCPs, knees), a facial rash that worsens in sunlight, mouth ulcers, and hair loss. Her ESR is 88 mm/h, urine shows 2+ protein. Classify: Inflammatory, polyarticular, systemic. Multisystem involvement — skin, mucosal, renal, and joint manifestations. Diagnosis: SLE. Key teaching: malar rash + photosensitivity + oral ulcers + proteinuria + arthritis = SLE until proven otherwise; ANA is the screening test; start hydroxychloroquine for all patients, add prednisolone and mycophenolate for nephritis.
CLINICAL PEARL
The single most important clinical skill in rheumatology is distinguishing inflammatory from mechanical joint pain — and it is a history skill, not a test skill. The question 'how long is your morning stiffness?' is the most discriminating question you can ask. Stiffness lasting ≥1 hour points to inflammatory arthritis (RA, seronegative spondyloarthropathy, SLE arthritis); stiffness <30 minutes that resolves quickly with movement points to degenerative disease. Cytokines accumulate in the joint overnight during rest, producing the prolonged inflammatory stiffness. Exercise disperses them. Never order an 'RA panel' without first forming a clinical hypothesis — RF is positive in 5–10% of the healthy population and will mislead you if you order it without a pre-test clinical probability assessment.
A second pearl: never start allopurinol during an acute gout attack — this common mistake prolongs the flare by mobilising urate crystals. Start colchicine or an NSAID to settle the attack first, then begin allopurinol ≥4 weeks later. Similarly, never start a TNF-α inhibitor without TB screening — TNF is critical for maintaining the granuloma around latent Mycobacterium tuberculosis, and anti-TNF therapy can reactivate latent TB with fatal consequences.