Page 2 of 15
IM8.1-7 | Hypertension Foundations — SDL Guide (Part 2)
Primary vs Secondary Hypertension: Distinguishing Features and Aetiologies
Primary (essential) hypertension accounts for 90–95% of all cases. It has no single identifiable cause — it is the product of interacting genetic, environmental, and physiological factors. It typically presents in the 30s–50s, is insidious in onset, and progresses gradually. There is often a positive family history. Its management is lifelong.
Secondary hypertension accounts for 5–10% of cases overall, but up to 20–30% of cases in younger patients (under 40), patients with severe hypertension (Stage 2 at presentation), resistant hypertension (BP uncontrolled on ≥3 drugs including a diuretic at optimal doses), and hypertension with hypokalaemia or metabolic abnormalities. Secondary hypertension is important because it may be curable (surgical correction of renal artery stenosis, adrenalectomy for phaeochromocytoma, primary aldosteronism, or Cushing syndrome) or specifically treatable — the drug class chosen for primary hypertension may be ineffective or even harmful in some secondary causes.
Clinical clues that should prompt a search for secondary hypertension:
- Young age (<30 years) or no family history of hypertension
- Abrupt onset or rapid progression
- Resistant to ≥3 antihypertensive drugs
- Hypokalaemia without diuretic therapy (primary aldosteronism)
- Episodic hypertension with headache, sweating, and palpitations (phaeochromocytoma triad)
- Abdominal bruit (renal artery stenosis)
- Truncal obesity, striae, proximal myopathy, cushingoid facies (Cushing syndrome)
- Sleep apnoea symptoms (snoring, daytime somnolence, witnessed apnoeas)
- Pulse disparity between arms or radio-femoral delay (aortic coarctation)
- Delayed femoral pulses and lower BP in legs than arms (coarctation)
- Thyroid abnormalities (systolic hypertension in hyperthyroidism, diastolic in hypothyroidism)
Major secondary causes and their mechanisms (IM8.4 and IM8.6):
1. Renovascular hypertension (renal artery stenosis): Reduced renal perfusion pressure → juxtaglomerular cells release renin → high renin state → angiotensin II → vasoconstriction + aldosterone → hypertension. Causes: atherosclerotic renal artery stenosis (older patients, risk factors for atherosclerosis, often unilateral) and fibromuscular dysplasia (FMD) (young women, beaded appearance of renal artery on angiography, often bilateral). Clue: abdominal/renal bruit, hypokalaemia. Investigation: renal Doppler ultrasound, CT angiography or MR angiography, captopril renography. Treatment: renal artery angioplasty (FMD — high success rate) or stenting (atherosclerotic — modest BP benefit); ACE inhibitors or ARBs reduce proteinuria but can precipitate acute kidney injury in bilateral stenosis (bilateral RAS is a relative contraindication to ACE inhibitor/ARB).
2. Primary aldosteronism (Conn syndrome): Autonomous excess aldosterone secretion independent of renin → sodium retention + potassium wasting → hypertension + hypokalaemia. Now recognised as the most common secondary cause of hypertension, accounting for 5–10% of all hypertensive patients (much higher than previously thought). Causes: aldosterone-producing adenoma (APA, Conn's original description) or bilateral adrenal hyperplasia (the commoner cause). Clue: hypokalaemia (spontaneous or diuretic-exacerbated), muscle weakness, polyuria. Investigation: plasma aldosterone-to-renin ratio (ARR) is the screening test (elevated in primary aldosteronism); confirmed by saline suppression test or fludrocortisone suppression test; adrenal CT/MRI; adrenal vein sampling to lateralise. Treatment: adrenalectomy for APA; spironolactone or eplerenone (mineralocorticoid antagonists) for bilateral hyperplasia.
3. Phaeochromocytoma: Catecholamine-secreting tumour of the adrenal medulla (phaeochromocytoma) or sympathetic ganglia (paraganglioma). Presents as episodic or sustained hypertension with the classic triad of headache + palpitations + diaphoresis (sweating). May be normotensive between episodes. Life-threatening hypertensive crises can be triggered by anaesthesia, surgery, contrast dye, or certain drugs (e.g., beta-blocker alone, metoclopramide). Can be part of MEN2A/2B or von Hippel-Lindau syndrome. Investigation: 24-hour urinary metanephrines and catecholamines (most sensitive), or plasma metanephrines; CT/MRI abdomen for localisation; MIBG scan for extra-adrenal or metastatic disease. Treatment: surgical excision, AFTER adequate alpha-blockade (phenoxybenzamine, minimum 10–14 days) — NEVER start a beta-blocker before adequate alpha-blockade (can cause paradoxical severe hypertension from unopposed alpha-vasoconstriction).
4. Cushing syndrome: Cortisol excess → hypertension via mineralocorticoid effects of cortisol, RAAS activation, and increased vascular sensitivity to catecholamines. Clinical features: central obesity, moon face, buffalo hump, striae (violaceous), proximal myopathy, easy bruising, hirsutism, glucose intolerance. Causes: pituitary ACTH-secreting adenoma (Cushing disease), adrenal adenoma, ectopic ACTH production. Investigation: 24-hour urinary free cortisol, late-night salivary cortisol, overnight dexamethasone suppression test. Treatment: depends on cause (transsphenoidal surgery for Cushing disease, adrenalectomy for adrenal adenoma, treat underlying malignancy for ectopic ACTH).
5. Coarctation of the aorta: Congenital narrowing of the aorta (typically just distal to the origin of the left subclavian artery) causes hypertension in the upper limbs with reduced or absent femoral pulses and lower BP in the lower limbs. Radio-femoral pulse delay is the clinical hallmark. CXR shows rib notching (from dilated intercostal collateral arteries). ECG may show left ventricular hypertrophy. Diagnosed by echocardiography or CT/MR aortography. Treatment: surgical repair or balloon dilatation with stenting.
6. Obstructive sleep apnoea (OSA): Recurrent nocturnal hypoxic episodes → sympathetic activation → raised 24-hour mean BP → non-dipping nocturnal BP pattern (failure of the normal nocturnal BP dip). OSA is increasingly recognised as a major cause of resistant hypertension. Treatment: CPAP therapy reduces daytime and nocturnal BP.
7. Drug-induced/exogenous: OCP (especially high-oestrogen preparations; oestrogen increases angiotensinogen and RAAS activity), NSAIDs (sodium retention, blunt the effect of diuretics and ACE inhibitors), glucocorticoids, decongestants (sympathomimetics), calcineurin inhibitors (tacrolimus, cyclosporine), erythropoietin, liquorice.
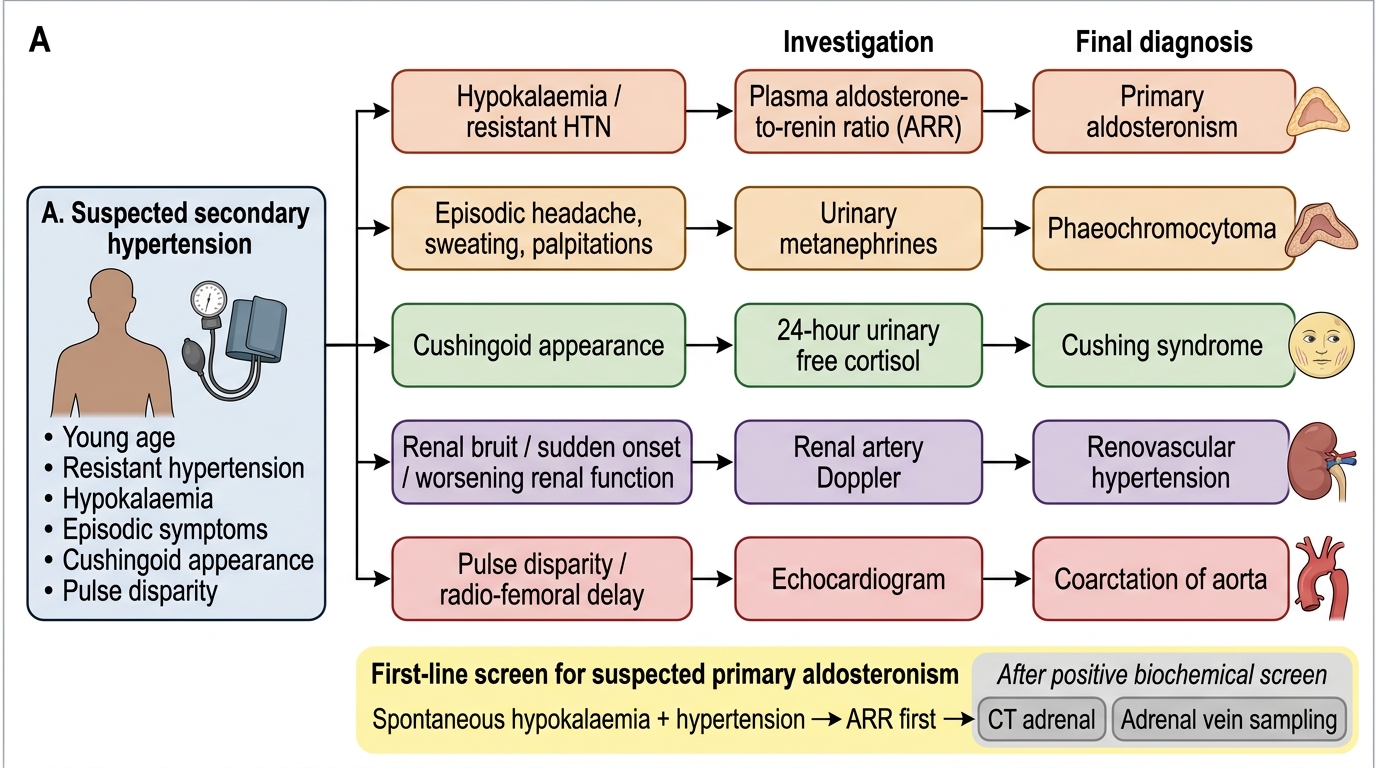
Diagnostic Algorithm for Suspected Secondary Hypertension
SELF-CHECK
A 34-year-old woman presents with hypertension (BP 178/102) and spontaneous hypokalaemia (serum K+ 2.8 mEq/L). She is on no diuretics. Which investigation is the BEST first-line screening test for primary aldosteronism?
A. 24-hour urinary potassium excretion
B. CT scan of the adrenal glands
C. Plasma aldosterone-to-renin ratio (ARR)
D. Adrenal vein sampling
Reveal Answer
Answer: C. Plasma aldosterone-to-renin ratio (ARR)
The plasma aldosterone-to-renin ratio (ARR) is the recommended first-line screening test for primary aldosteronism. An elevated ARR (typically >30 with aldosterone in ng/dL and plasma renin activity in ng/mL/hr, though cut-offs vary by laboratory) indicates autonomous aldosterone excess suppressing renin. CT adrenal imaging and adrenal vein sampling are appropriate but come AFTER a positive ARR screen. Adrenal vein sampling is the gold standard for lateralisation (to distinguish adenoma from bilateral hyperplasia) but is performed only after biochemical confirmation. Urinary potassium would confirm renal potassium wasting but does not identify the cause. The combination of hypertension + spontaneous hypokalaemia in a young patient without diuretics is a classic trigger to screen for primary aldosteronism.
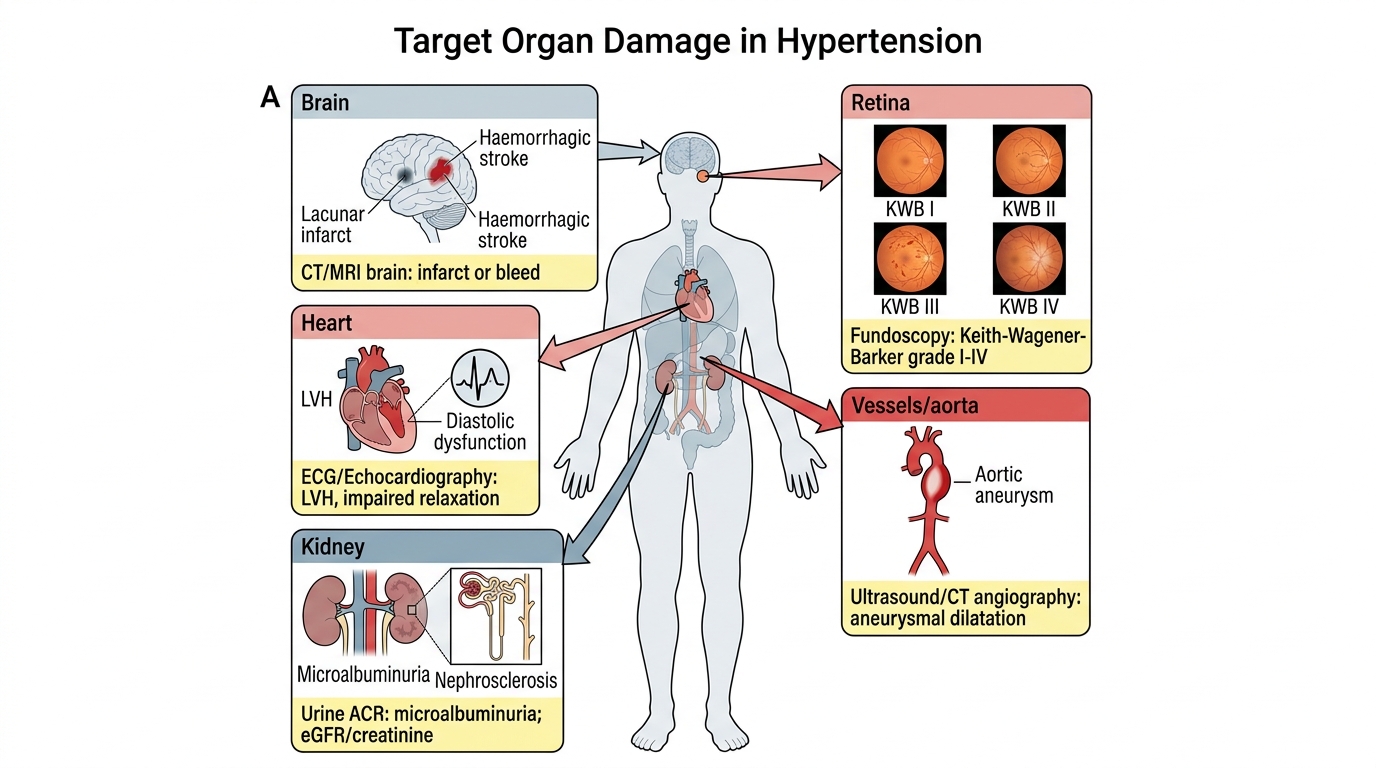
Target Organ Damage in Hypertension
Target organ damage (TOD) in hypertension refers to the structural and functional harm that sustained elevated blood pressure inflicts on specific organs — the heart, brain, kidneys, retina, and large vessels. Recognising TOD is one of the most clinically important skills for the final-year student because it serves two distinct and complementary purposes. First, the presence of TOD upgrades the patient's cardiovascular risk category to 'very high' regardless of the current BP reading or 10-year risk score, directly informing the urgency and intensity of antihypertensive therapy. Second, the nature and severity of TOD provide a window into the cumulative haemodynamic burden over years or decades, allowing the clinician to estimate how long hypertension has been present and how well controlled it has been — even in the patient who, like Ramesh, presents for the first time and is asymptomatic. The systematic identification of TOD therefore transforms a single blood pressure number into a longitudinal narrative of disease severity. Competency IM8.7 requires the ability to describe, discuss, and identify TOD from history, examination, ECG, fundoscopy, urinalysis, and basic blood tests — the exact toolkit available at a district hospital or outpatient clinic without advanced imaging.
Heart:
- Left ventricular hypertrophy (LVH): The most important cardiac consequence of sustained hypertension. Increased afterload (elevated SVR) forces the left ventricle to generate higher wall stress, triggering concentric LVH (increased wall thickness, normal or small cavity). LVH on ECG (voltage criteria: Sokolow-Lyon criteria: S in V1 + R in V5/V6 >35 mm; Cornell criteria: R in aVL + S in V3 >28 mm in men, >20 mm in women) indicates significant hypertensive burden. Echocardiographic LVH (LV mass index >115 g/m² in men, >95 g/m² in women by BSA) is more sensitive. LVH is independently associated with increased risk of ventricular arrhythmia, sudden cardiac death, and heart failure.
- Diastolic dysfunction: LVH-related increased myocardial stiffness impairs relaxation (diastolic dysfunction), raising LV filling pressures. This manifests as HFpEF (heart failure with preserved ejection fraction) — dyspnoea on exertion, orthopnoea, with normal LVEF. Echocardiographic findings: E/A ratio <1 (Grade I), or elevated E/e' ratio.
- Coronary artery disease (CAD): Hypertension is a major risk factor for atherosclerotic CAD through endothelial damage, LDL oxidation, and plaque formation. Hypertensive patients are at 2-3× increased risk of myocardial infarction.
- Heart failure: Chronic LVH can progress to systolic dysfunction (HFrEF, LVEF ≤40%) in advanced hypertensive heart disease.
- Atrial fibrillation: LVH and diastolic dysfunction raise left atrial pressure, causing left atrial enlargement and predisposing to AF.
Brain:
- Lacunar infarction: Small vessel disease in penetrating arteries (lenticulostriate arteries, pontine perforators) causes lacunar infarcts — small, deep infarcts producing classic lacunar syndromes (pure motor stroke, pure sensory stroke, ataxic hemiparesis, dysarthria-clumsy hand). Hypertension is the dominant risk factor.
- Haemorrhagic stroke: Chronic hypertension causes lipohyalinosis (replacement of vessel wall smooth muscle by fibrous tissue) in deep perforating arteries and development of Charcot-Bouchard microaneurysms. Rupture causes hypertensive intracerebral haemorrhage — most commonly in the basal ganglia (putamen/thalamus), internal capsule, pons, and cerebellum.
- Vascular dementia: Widespread small vessel disease and lacunar infarction leads to vascular cognitive impairment and dementia, characterised by stepwise decline.
- Hypertensive encephalopathy/PRES: Acute extreme BP elevation overwhelms cerebrovascular autoregulation → forced vasodilation → cerebral oedema, particularly in the posterior parietal and occipital regions.
Kidneys:
- Hypertensive nephrosclerosis: Chronic hypertension causes afferent arteriolar hyalinisation and interlobular artery wall thickening → glomerular ischaemia → glomerulosclerosis → progressive GFR reduction. Microalbuminuria (urinary albumin excretion 30–300 mg/day, or albumin-to-creatinine ratio ACR 30–300 mg/g) is the earliest marker of hypertensive renal involvement — it both reflects renal damage and predicts future cardiovascular events. Overt proteinuria (>300 mg/day) and rising creatinine indicate established nephrosclerosis.
- End-stage renal disease (ESRD): Hypertension is the second most common cause of ESRD after diabetic nephropathy in India.
Retina:
- Keith-Wagener-Barker (KWB) grading of hypertensive retinopathy:
- Grade I: Mild arteriolar narrowing (increased light reflex, 'silver wiring')
- Grade II: Moderate arteriolar narrowing + arteriovenous (AV) nicking (Salus sign, Gunn sign)
- Grade III: Grade II + flame haemorrhages and/or cotton-wool spots (nerve fibre layer infarcts)
- Grade IV: Grade III + papilloedema (swelling of optic disc)
- Grades III–IV constitute hypertensive emergency — immediate BP control is required.
Large vessels:
- Aortic aneurysm and dissection: Hypertension is the major risk factor for aortic aneurysm formation and for Type A and Type B aortic dissection.
- Peripheral arterial disease (PAD): Hypertension accelerates lower limb atherosclerosis; ankle-brachial index (ABI) <0.9 indicates significant PAD.
Target Organ Damage in Hypertension
Hypertensive Urgency and Emergency
A hypertensive crisis is defined as a severe elevation of blood pressure — typically systolic >180 mmHg and/or diastolic >120 mmHg — that requires a clinical decision about the urgency and pace of intervention. The critical distinction is NOT based on the BP number alone, but on whether there is acute end-organ damage.
Hypertensive urgency (IM8.5): Severe elevation of BP (usually >180/120 mmHg) without evidence of acute target organ damage. The patient may have headache or nausea but has no acute neurological signs, no chest pain, no breathlessness, no acute kidney injury, and normal retinal examination (or only grade I-II changes). There is no immediate life threat. Management involves gradual reduction of BP over 24–48 hours using oral agents (amlodipine, telmisartan, clonidine, or labetalol orally). Rapid BP reduction is CONTRAINDICATED in urgency — precipitous lowering in a patient with chronically elevated BP risks cerebral ischaemia (autoregulation has reset to operate at higher pressures), myocardial ischaemia, and acute kidney injury. The patient can be managed as an outpatient after confirming response to the first oral dose.
Hypertensive emergency (IM8.5): Severe elevation of BP with evidence of acute end-organ damage — this is a true medical emergency requiring immediate hospitalisation, continuous BP monitoring (intra-arterial line if available), and carefully titrated intravenous antihypertensive therapy. The goal is controlled, NOT precipitous, BP reduction.
Target organ damage patterns that define hypertensive emergency:
| Organ | Manifestation | Notes |
|---|---|---|
| Brain | Hypertensive encephalopathy — confusion, headache, visual disturbance, seizures; PRES (posterior reversible encephalopathy syndrome) | MRI/CT to exclude haemorrhagic stroke first |
| Brain (stroke) | Acute ischaemic or haemorrhagic stroke with very high BP | BP management differs for haemorrhagic vs ischaemic stroke |
| Heart | Acute pulmonary oedema, acute coronary syndrome (NSTEMI/STEMI) | New ST changes, troponin rise, S3 gallop |
| Aorta | Acute aortic dissection — tearing, interscapular pain, pulse differential | Immediate surgical consult; target SBP <120 mmHg rapidly |
| Kidney | Acute kidney injury — rising creatinine, oliguria, haematuria, heavy proteinuria (malignant hypertension) | Microangiopathic haemolytic anaemia may coexist |
| Retina | Grade III (flame haemorrhages, cotton-wool spots) or Grade IV (papilloedema) — funduscopic emergency | Keith-Wagener-Barker grading |
| Uterus (pregnancy) | Severe pre-eclampsia or eclampsia (≥160/110 mmHg + proteinuria + neurological symptoms) | Immediate obstetric involvement |
BP targets and intravenous agents in hypertensive emergency:
The general rule is: reduce mean arterial pressure (MAP) by no more than 20–25% in the first hour, then gradually to 160/100 mmHg over the next 2–6 hours, then to goal over 24–48 hours. Exception: aortic dissection — target SBP <120 mmHg within 20 minutes using IV labetalol (combined alpha + beta block) or esmolol + nitroprusside.
Commonly used IV agents:
- Labetalol (IV bolus or infusion): combined alpha-1 and non-selective beta-blocker; useful for most emergencies including aortic dissection and hypertensive encephalopathy
- Nicardipine (IV infusion): dihydropyridine CCB; smooth titratability; good for hypertensive encephalopathy and perioperative hypertension
- Sodium nitroprusside (IV infusion): immediate onset vasodilator (arterial + venous); risk of cyanide toxicity with prolonged use (>24–48 hours, renal failure); use in ICU with continuous arterial monitoring
- Esmolol (IV infusion): ultra-short-acting beta-1 selective blocker; used in aortic dissection with nitroprusside, perioperative, and tachyarrhythmia
- Hydralazine (IV): direct arterial vasodilator; used in pre-eclampsia/eclampsia; unpredictable, can cause reflex tachycardia
- Furosemide (IV): loop diuretic; indicated when there is acute pulmonary oedema or volume overload
Malignant hypertension (also called accelerated-malignant hypertension) is a specific syndrome of severely elevated BP with grade III–IV retinopathy and evidence of microangiopathic haemolytic anaemia, thrombocytopaenia, and acute kidney injury — a form of hypertensive emergency associated with thrombotic microangiopathy affecting the renal and cerebral microvasculature.
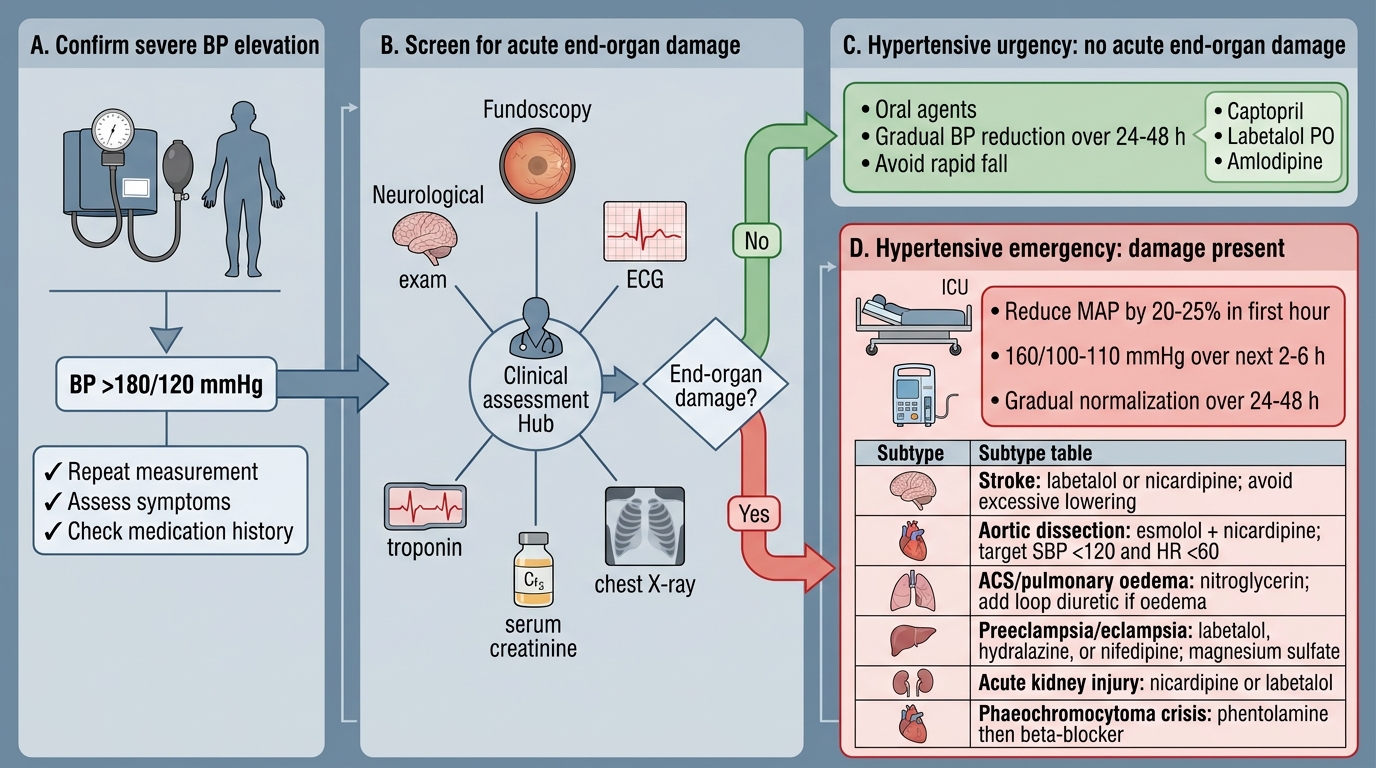
Triage and Management of Hypertensive Crisis
SELF-CHECK
A 58-year-old man with poorly controlled hypertension (average BP 176/108 mmHg for 8 years) presents with gradually worsening exertional dyspnoea. His ECG shows S in V1 (18mm) + R in V5 (20mm) = 38mm. His echo shows LVEF 62%, E/A ratio 0.7, elevated E/e' ratio. His urine ACR is 55 mg/g. What is the most accurate characterisation of his cardiac involvement?
A. Heart failure with reduced ejection fraction (HFrEF) due to hypertensive cardiomyopathy
B. Left ventricular hypertrophy with diastolic dysfunction (HFpEF) — hypertensive heart disease
C. Right heart failure secondary to pulmonary hypertension
D. Coronary artery disease with normal systolic function
Reveal Answer
Answer: B. Left ventricular hypertrophy with diastolic dysfunction (HFpEF) — hypertensive heart disease
This patient has hypertensive heart disease with LVH (Sokolow-Lyon criteria: S in V1 + R in V5/V6 >35 mm — here 38 mm, positive) and diastolic dysfunction (E/A <1 suggests Grade I diastolic dysfunction; elevated E/e' suggests elevated LV filling pressure). LVEF is 62%, which is preserved (≥50%), so this is HFpEF (heart failure with preserved ejection fraction), not HFrEF. The urine ACR of 55 mg/g indicates microalbuminuria — a marker of hypertensive renal involvement. This is classic hypertensive heart disease with target organ damage to both heart and kidneys. HFrEF would require LVEF ≤40%; there is no evidence of right heart failure or CAD from the data given.