Page 3 of 15
IM8.1-7 | Hypertension Foundations — SDL Guide (Part 3)
Self-Assessment: Integrating Foundations of Hypertension
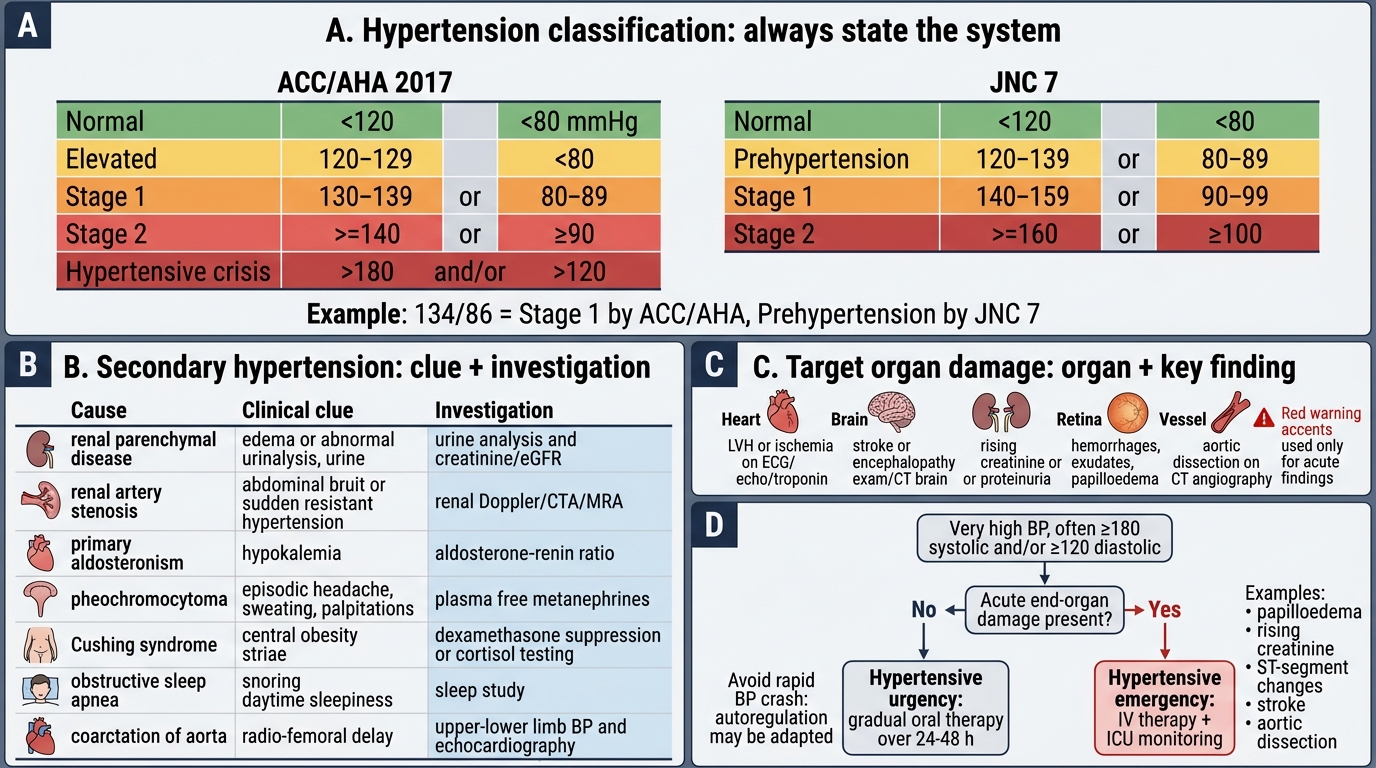
You have now covered the core foundations of hypertension: definitions and staging (ACC/AHA 2017 vs JNC 7), epidemiology and genetics, pathophysiology of primary hypertension, primary vs secondary causes with clinical clues and investigation, hypertensive urgency vs emergency, and target organ damage. The following integrative scenarios consolidate this learning at the KH level required for IM8.1–IM8.7.
Scenario A — Staging and Clinical Clues:
A 38-year-old man is found to have BP 158/98 mmHg on three visits. He has spontaneous serum potassium of 2.9 mEq/L without diuretic use. He has no family history of hypertension. How would you classify his BP under (a) ACC/AHA 2017 and (b) JNC 7? What is the most likely secondary cause, and what is the first-line screening investigation?
Analysis: (a) ACC/AHA 2017: systolic 158 and diastolic 98 — Stage 2 hypertension (≥140/≥90). (b) JNC 7: Stage 1 (140–159 systolic). Clinical clues to secondary cause: young age, no family history, spontaneous hypokalaemia → primary aldosteronism. First-line investigation: plasma aldosterone-to-renin ratio (ARR).
Scenario B — Urgency vs Emergency:
A 55-year-old woman is brought to the emergency department with severe headache and BP 200/118 mmHg. Fundoscopy shows grade III changes (flame haemorrhages and cotton-wool spots). Her Glasgow Coma Scale is 15/15, she has no focal neurological deficits, her troponin is normal, creatinine is mildly elevated at 1.4 mg/dL (baseline unknown), and her ECG shows LVH. Is this urgency or emergency? What is the target BP reduction in the first hour, and what agent would you use?
Analysis: Hypertensive emergency — grade III retinopathy (haemorrhages and cotton-wool spots) constitutes acute end-organ damage (retinal). The mildly elevated creatinine may represent acute-on-chronic hypertensive nephropathy. Management: admit to ICU, IV agent (nicardipine or labetalol), target MAP reduction of no more than 20–25% in the first hour (do NOT aim for normal BP acutely). After stabilisation, investigate for secondary causes given relatively young age.
Scenario C — Target Organ Damage Review:
For Ramesh (from the hook), list ALL the evidence of target organ damage present at his initial visit: ECG finding, urine finding, and fundoscopic finding. What does each indicate?
Analysis:
- ECG: LVH with strain pattern → cardiac TOD (hypertensive heart disease)
- Urine: 2+ proteinuria → renal TOD (hypertensive nephrosclerosis; must quantify with spot ACR or 24-hour urine protein)
- Fundoscopy: AV nicking + arteriolar narrowing → grade II hypertensive retinopathy
All three indicate established, multi-organ target organ damage consistent with years of undetected or untreated hypertension. This upgrades his cardiovascular risk to very high (TOD present) regardless of the 10-year cardiovascular risk score — intensive BP control and assessment for other risk factors (diabetes, dyslipidaemia, smoking) are mandatory.
Hypertension Foundations: Classification, Causes, Damage, and Emergencies
CLINICAL PEARL
The most important single insight in hypertension management is that blood pressure numbers alone do not determine urgency versus emergency — the presence or absence of acute end-organ damage does. A patient with BP 210/130 mmHg who is alert, has no focal neurology, normal retinas, normal troponin, and stable creatinine has a hypertensive urgency — gradual oral therapy over 24–48 hours is appropriate and safe. The same BP with fundoscopic papilloedema, a rising creatinine, or ST-segment changes on ECG is an emergency requiring IV therapy and ICU monitoring. Students who confuse the two risk either undertreating a true emergency or causing iatrogenic harm by crashing the BP of a patient with urgency, whose cerebral autoregulation has adapted to a higher pressure set-point and may not tolerate a rapid drop.
A second pearl: always state which BP classification system you are using. The difference between ACC/AHA 2017 (threshold 130/80) and JNC 7 (threshold 140/90) is not merely academic — a patient at 134/86 is Stage 1 hypertensive on ACC/AHA guidelines, requiring treatment if they have high cardiovascular risk, but is only pre-hypertensive on JNC 7, requiring lifestyle modification. Indian hospital protocols often follow IGH-IV/JNC 7, but examination questions may use either. Name the system and apply it correctly.