Page 8 of 19
IM9.6-9 | Anaemia Diagnostic Testing — SDL Guide
Learning Objectives
- Select and justify an appropriate diagnostic workup for anaemia based on clinical pre-test probability and presumed aetiology (IM9.6)
- Interpret each component of the haemogram — Hb, MCV, MCH, MCHC, RDW, and reticulocyte count — in terms of its biological basis and diagnostic significance (IM9.7)
- Describe and interpret peripheral blood smear findings including microcytic hypochromic, macrocytic megaloblastic, spherocytic, sickling, and schistocyte patterns (IM9.7)
- Interpret iron studies (ferritin, serum iron, TIBC, transferrin saturation) to differentiate IDA, ACD, thalassaemia trait, and sideroblastic anaemia (IM9.7)
- Interpret B12, folate, MMA, homocysteine, and haemolytic markers (LDH, bilirubin, haptoglobin, Coombs test) in macrocytic and haemolytic anaemia (IM9.7)
- Describe the indications for bone marrow aspiration and trephine biopsy and interpret key findings (IM9.8)
- Construct an integrated diagnostic plan for common anaemia presentations including IDA in pregnancy, microcytic anaemia in a young Indian person, macrocytic anaemia with pancytopaenia, and haemolytic anaemia (IM9.9)
INSTRUCTIONS
Anaemia is one of the most common clinical problems in Indian medical practice, and its correct management depends entirely on accurate identification of the underlying cause. This module teaches you to approach anaemia diagnostics systematically — using the haemogram, peripheral smear, iron studies, B12 and folate markers, and haemolytic indices as an integrated panel — and to know when to escalate to bone marrow examination. Each section builds from the biological principles governing each test toward the clinical reasoning needed to construct a diagnostic plan for real patients.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 99 — Anaemia and Polycythaemia (textbook)
- API Textbook of Medicine, 10th ed. — Anaemia chapter (textbook)
- Hoffbrand's Essential Haematology, 8th ed. (textbook)
- ICMR Guidelines for Management of Anaemia in India (guideline)
- British Society for Haematology Guideline on Investigation and Management of Anaemia (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old woman presents with progressive fatigue and dyspnoea on climbing two flights of stairs. Her haemoglobin is 7.8 g/dL. The intern orders a haematinics panel and waits for the results. Two days later, the ferritin returns at 6 ng/mL, serum iron 28 µg/dL, TIBC 520 µg/dL, and transferrin saturation 5.4% — a classic iron-deficiency pattern. But a second look at the peripheral smear shows not only microcytic hypochromic red cells but also a population of macrocytes and hypersegmented neutrophils. The intern's straightforward diagnosis has become complicated: this patient may have a mixed deficiency of iron and vitamin B12. Without the peripheral smear, that crucial second diagnosis would have been missed entirely. Now consider a different scenario: a 25-year-old man with sickle cell disease presents with an acute haemolytic crisis. His haemoglobin has fallen from a baseline of 9 g/dL to 6.2 g/dL over 48 hours. The reticulocyte count is 18% — a reassuring sign of active marrow response. But the LDH is 980 IU/L, total bilirubin is 4.8 mg/dL (unconjugated fraction 3.9 mg/dL), and haptoglobin is undetectable. The smear shows sickled cells, polychromasia, and occasional nucleated red cells. Each number tells a specific part of the haemolysis story. These two cases illustrate a central truth about anaemia diagnostics: the laboratory investigations are not a checklist but a structured interrogation of the red cell lifecycle, and the physician who understands each test's biological basis can read that story accurately.
WHY THIS MATTERS
Anaemia affects approximately 40% of the global population, with India bearing one of the highest burdens — the National Family Health Survey (NFHS-5, 2019–21) reported anaemia in 57% of women aged 15–49, 67% of children under 5, and 25% of adult men. Yet anaemia is not a diagnosis in itself — it is a haematological abnormality whose correct management depends entirely on identifying the underlying cause. Inappropriate empirical treatment with iron when the patient actually has thalassaemia trait, or failing to investigate a new-onset microcytic anaemia in a 55-year-old man who needs colonoscopy not oral iron, are common and preventable errors that stem from incomplete diagnostic reasoning. For the final-year MBBS student, competencies IM9.6 through IM9.9 demand more than familiarity with test names — they require you to select investigations based on the presumed aetiology, understand the biological basis of each component of the haemogram, interpret results in clinical context, and construct a logical diagnostic plan that narrows the differential to the correct cause.
RECALL
Activate your prior knowledge before proceeding. Recall that anaemia is classified by two complementary frameworks: the morphological classification based on mean corpuscular volume (MCV) — microcytic (<80 fL), normocytic (80–100 fL), and macrocytic (>100 fL) — and the kinetic classification based on reticulocyte production index (RPI): hypoproliferative anaemia (RPI <2, marrow not responding) versus hyperproliferative anaemia (RPI ≥2, marrow working harder than normal, as in haemolysis or blood loss). Recall the major causes under each category: microcytic = iron deficiency, thalassaemia, anaemia of chronic disease, sideroblastic; normocytic = anaemia of chronic disease, aplastic anaemia, CKD, hypothyroidism; macrocytic = B12 deficiency, folate deficiency, myelodysplastic syndrome, drugs. Also recall basic red cell physiology: the red cell lifespan is approximately 120 days, and old cells are destroyed in the reticuloendothelial system, releasing iron for recycling, bilirubin for hepatic conjugation, and raising LDH. These relationships underpin the interpretation of every test that follows.
Clinical Indication and Diagnostic Triage of Anaemia
The decision about which investigations to order for a patient with anaemia begins with a clinical triage based on the history, examination, and initial complete blood count (CBC) — not with a reflex panel of every available test. Ordering investigations rationally requires first constructing a pre-test probability estimate of the likely aetiology based on clinical context, then selecting tests that will most efficiently confirm or exclude the top differential diagnoses.
The clinical clues that should guide the initial investigation strategy are as follows. First, age, sex, and physiological state: a pre-menopausal woman with menorrhagia almost certainly has iron deficiency anaemia; an elderly man with new-onset microcytic anaemia requires investigation for gastrointestinal blood loss until proven otherwise; a pregnant woman with macrocytosis needs folate and B12 levels. Second, dietary history and geographical background: vegetarian diet in India increases risk of B12 and iron deficiency. Third, ethnic background: thalassaemia trait is prevalent among individuals from Gujarat, Maharashtra, and parts of Tamil Nadu; sickle cell disease is prevalent in Odisha, Chhattisgarh, and tribal populations in central India; G6PD deficiency is common across South Asia. Fourth, medication history: metformin impairs B12 absorption over time; methotrexate and hydroxyurea are anti-folate agents; NSAIDs cause chronic GI blood loss; phenytoin interferes with folate metabolism. Fifth, systemic symptoms: fever, night sweats, and weight loss suggest an inflammatory or malignant cause; jaundice points toward haemolysis; bone pain suggests marrow infiltration. Sixth, family history: haemolytic anaemias including sickle cell disease, thalassaemia, hereditary spherocytosis, and G6PD deficiency are heritable.
Once the clinical pre-test probability is formulated, the investigation strategy follows a tiered approach. The first tier is the complete haemogram (CBC with differential), red cell indices, and peripheral blood smear — these three together provide the morphological classification and a first-pass kinetic estimate. The second tier is targeted at the suspected aetiology: iron studies (serum ferritin, serum iron, TIBC, transferrin saturation) for microcytic anaemia; B12 and folate levels for macrocytic anaemia; reticulocyte count and haemolytic markers (LDH, bilirubin, haptoglobin, Coombs test) for haemolytic anaemia; bone marrow aspiration and biopsy for unexplained anaemia or marrow failure syndromes. The third tier — aetiological investigations — identifies the root cause: upper and lower gastrointestinal endoscopy for IDA in adults; haemoglobin electrophoresis for thalassaemia and haemoglobinopathy; red cell enzyme assay (G6PD activity) for enzyme-deficiency haemolysis; renal function tests and erythropoietin levels for anaemia of chronic kidney disease.
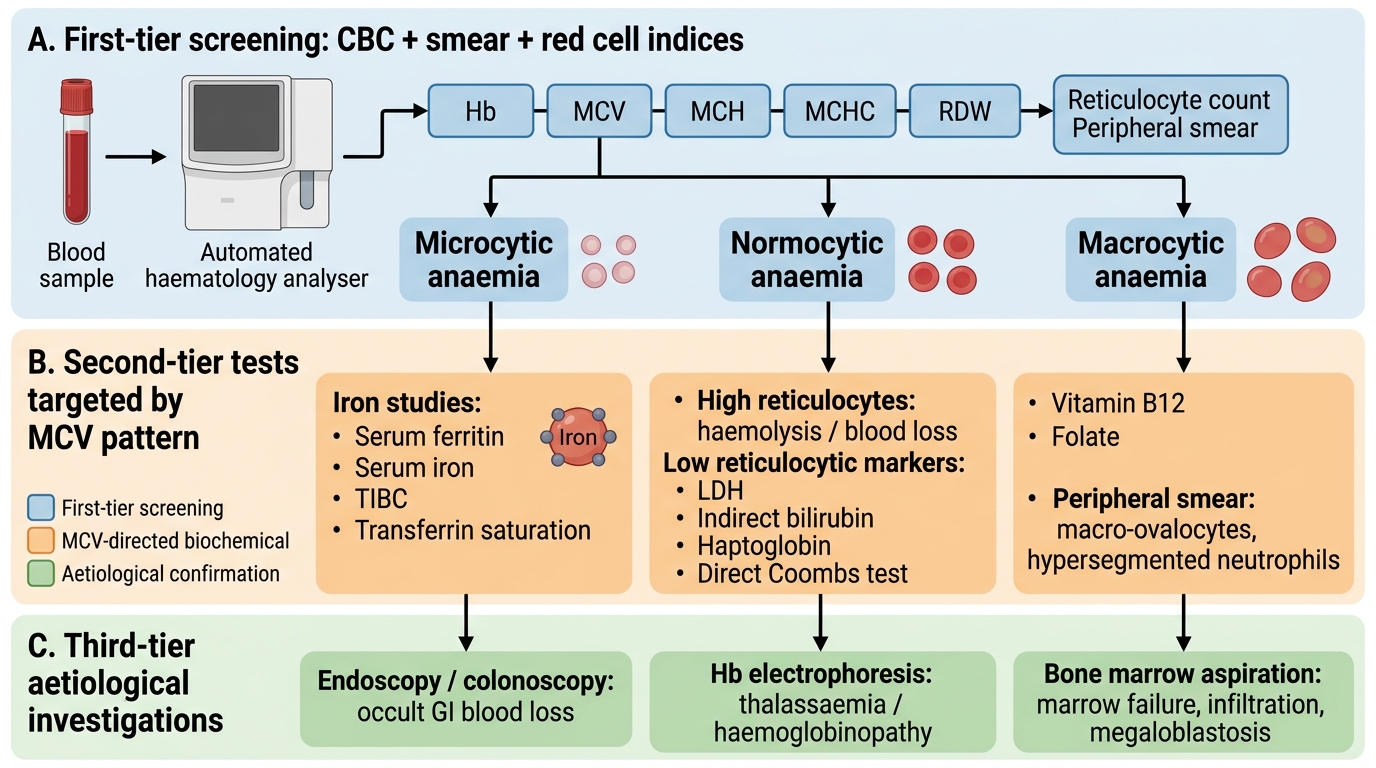
Tiered Diagnostic Algorithm for Anaemia
The Haemogram and Red Cell Indices — Governing Principles
The complete blood count (CBC) or haemogram is the starting point of every anaemia investigation. Understanding what each component measures at the cellular and physiological level — not merely the normal range — is what allows the clinician to extract maximum information from a single test. The modern automated haematology analyser counts cells by impedance (Coulter principle) or light scatter, measures haemoglobin by cyanmethaemoglobin colorimetry, and calculates all derived indices mathematically. Knowing this prevents the common error of dismissing the haemogram as merely a blood count.
Provided image
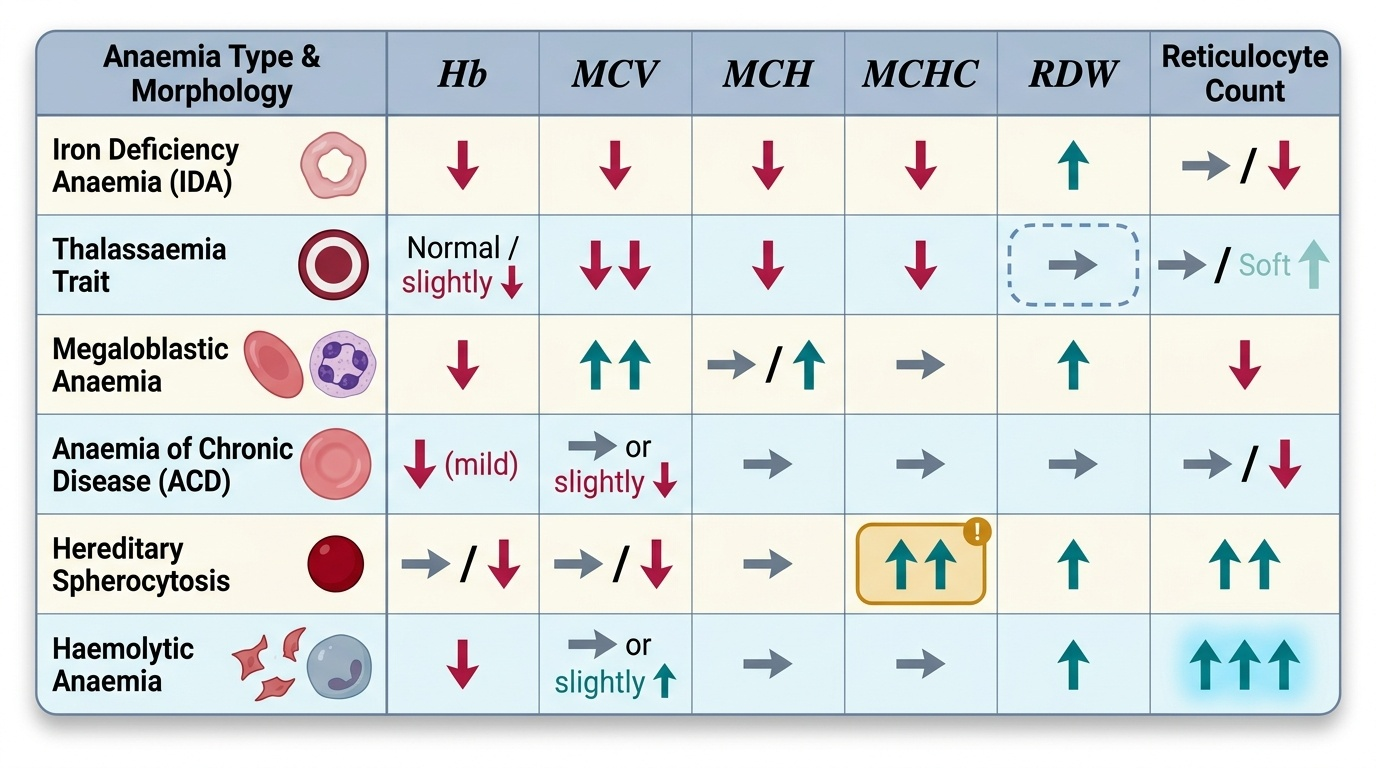
Haemoglobin (Hb): The primary measure of anaemia severity. In adults, anaemia is defined as Hb <13.0 g/dL in men and <12.0 g/dL in women (WHO criteria). In pregnancy, <11.0 g/dL is used. Severity grading: mild (Hb 10.0–12.9 g/dL in men, 10.0–11.9 g/dL in women), moderate (7.0–9.9 g/dL), severe (<7.0 g/dL), very severe (<4.0 g/dL). The haemoglobin value alone does not indicate the cause; context and indices are essential.
Mean Corpuscular Volume (MCV): The average volume of a red cell in femtolitres (fL). Reference range 80–100 fL. MCV <80 fL = microcytosis (causes: IDA, thalassaemia, ACD, sideroblastic anaemia); MCV >100 fL = macrocytosis (causes: B12 deficiency, folate deficiency, MDS, reticulocytosis — reticulocytes are larger than mature red cells); MCV 80–100 fL = normocytic (causes: acute blood loss, haemolytic anaemia, aplastic anaemia, ACD). The MCV is an average and can therefore be misleadingly normal in mixed deficiency (iron plus B12 or folate), where the microcytic and macrocytic populations cancel each other out. This is the MCV-averaging trap.
Mean Corpuscular Haemoglobin (MCH): The average haemoglobin content per red cell in picograms. Normal range 27–33 pg. MCH is low in microcytic hypochromic states such as IDA and thalassaemia. MCH is the most stable red cell index and changes less with sample storage artefact.
Mean Corpuscular Haemoglobin Concentration (MCHC): The average haemoglobin concentration per unit volume of packed red cells, in g/dL. Normal range 32–36 g/dL. MCHC is LOW in IDA and thalassaemia (hypochromia). Crucially, MCHC is HIGH (>36 g/dL) in hereditary spherocytosis — spherocytes are small, dense, and uniformly haemoglobin-concentrated — making an elevated MCHC a key diagnostic flag for this condition. MCHC is also raised in sickle cell disease during sickling.
Red Cell Distribution Width (RDW): A measure of the variability in red cell size (anisocytosis). Normal range 11.5–14.5%. RDW is ELEVATED in IDA (rises early, before MCV falls), B12 and folate deficiency, and haemolytic anaemias. RDW is NORMAL in thalassaemia trait and ACD. This is diagnostically powerful: the combination of LOW MCV plus HIGH RDW points strongly toward IDA; LOW MCV plus NORMAL RDW points toward thalassaemia trait. This distinction is clinically critical in India where both conditions are highly prevalent and may appear identical on Hb level alone.
Reticulocyte Count and Reticulocyte Production Index (RPI): The reticulocyte count (normal 0.5–1.5% or 25,000–75,000 cells/µL) reflects the bone marrow's erythropoietic output. The reticulocyte production index (RPI) corrects for the degree of anaemia and early reticulocyte release: RPI = (reticulocyte count% × patient Hct / normal Hct) / maturation factor (1.0 at Hct ≥40%, 1.5 at 30–39%, 2.0 at 20–29%, 2.5 at <20%). RPI <2 = hypoproliferative (marrow not responding — iron deficiency, B12 or folate deficiency, aplastic anaemia, ACD, CKD); RPI ≥2 = hyperproliferative (marrow responding appropriately — haemolysis, acute blood loss with iron-replete marrow). The RPI is the kinetic bridge between the haemogram and the peripheral smear.
Peripheral Blood Smear — Technique and Morphological Interpretation
The peripheral blood smear (PBS) remains the single most informative test in anaemia diagnostics, providing morphological information that no automated analyser can replicate. A skilled smear reader can diagnose iron deficiency, megaloblastic anaemia, hereditary spherocytosis, haemolytic anaemia, malarial parasitaemia, leukaemia, and many other conditions from a single well-prepared slide. The key is understanding what to look for and why specific morphological features arise — because morphology reflects the underlying pathophysiology directly.
Smear preparation and reading technique: Blood is collected in an EDTA tube and a thin smear made within 1–2 hours of collection. The smear is stained with Leishman's stain or May-Grünwald-Giemsa (MGG). The reading area is the monolayer zone — the area where red cells are just touching but not overlapping each other. In the thick head and thin tail zones of the smear, cells are distorted and morphological interpretation is unreliable. Under oil immersion (100×), at least 100–200 red cells should be systematically examined before reporting.
Key red cell morphological features and their diagnostic significance:
Microcytes with central pallor >1/3 of cell diameter (hypochromia): IDA, thalassaemia, ACD, sideroblastic anaemia. In IDA specifically, cells are also elongated — pencil cells (elongated elliptocytes) are a feature specific to iron deficiency. In thalassaemia trait, the smear characteristically shows target cells (codocytes): cells with a central dense spot surrounded by a pale ring and a dense periphery (like a shooting target), arising from excess membrane relative to haemoglobin content. Basophilic stippling (punctate blue dots in red cells from ribosomal RNA aggregates) is also seen in thalassaemia and in heavy metal poisoning (lead).
Macrocytes — cells larger than the nucleus of a small lymphocyte. In megaloblastic anaemia from B12 or folate deficiency, macrocytes are characteristically oval (oval macrocytes), not round. The most specific smear finding for megaloblastic anaemia is the hypersegmented neutrophil — a neutrophil with ≥5 lobes, or any neutrophil with ≥6 lobes. Even a single 6-lobed neutrophil on the smear should raise suspicion of megaloblastic anaemia. This finding precedes macrocytosis by weeks and may be the first objective laboratory abnormality. Round macrocytes are seen in liver disease and alcohol use.
Spherocytes — small, round, densely staining cells lacking central pallor: seen in hereditary spherocytosis (numerous and uniform in appearance) and autoimmune haemolytic anaemia (AIHA) (spherocytes among a background of polychromasia). Spherocytes arise because membrane loss (through complement or antibody-mediated damage, or membrane protein defects in HS) with preserved haemoglobin content creates a small, round, dense cell with high MCHC.
Sickle cells (drepanocytes) — elongated, crescent-shaped cells: diagnostic of sickle cell disease (HbSS) or detectable in sickle cell trait under severe deoxygenation. Also look for boat-shaped (oat-cell) variants and irreversibly sickled cells in chronic disease.
Schistocytes (fragmented red cells) — helmet cells, triangle cells, and other fragments: pathognomonic of microangiopathic haemolytic anaemia (MAHA) — caused by thrombotic thrombocytopenic purpura (TTP), haemolytic uraemic syndrome (HUS), disseminated intravascular coagulation (DIC), and malignant hypertension. Schistocytes on the smear mandate immediate checking of platelets, LDH, creatinine, and coagulation profile.
Polychromasia — bluish-grey tinge to some red cells due to residual RNA: corresponds to reticulocytes released prematurely. Marked polychromasia = markedly elevated reticulocyte count = haemolysis or haemorrhage with active marrow response.
Intraerythrocytic parasites — ring forms of Plasmodium falciparum (multiple rings per cell, 'appliqué' forms at the red cell margin); P. vivax (enlarged cells with Schüffner's dots). Peripheral smear remains the gold standard for malaria diagnosis in resource-limited settings.
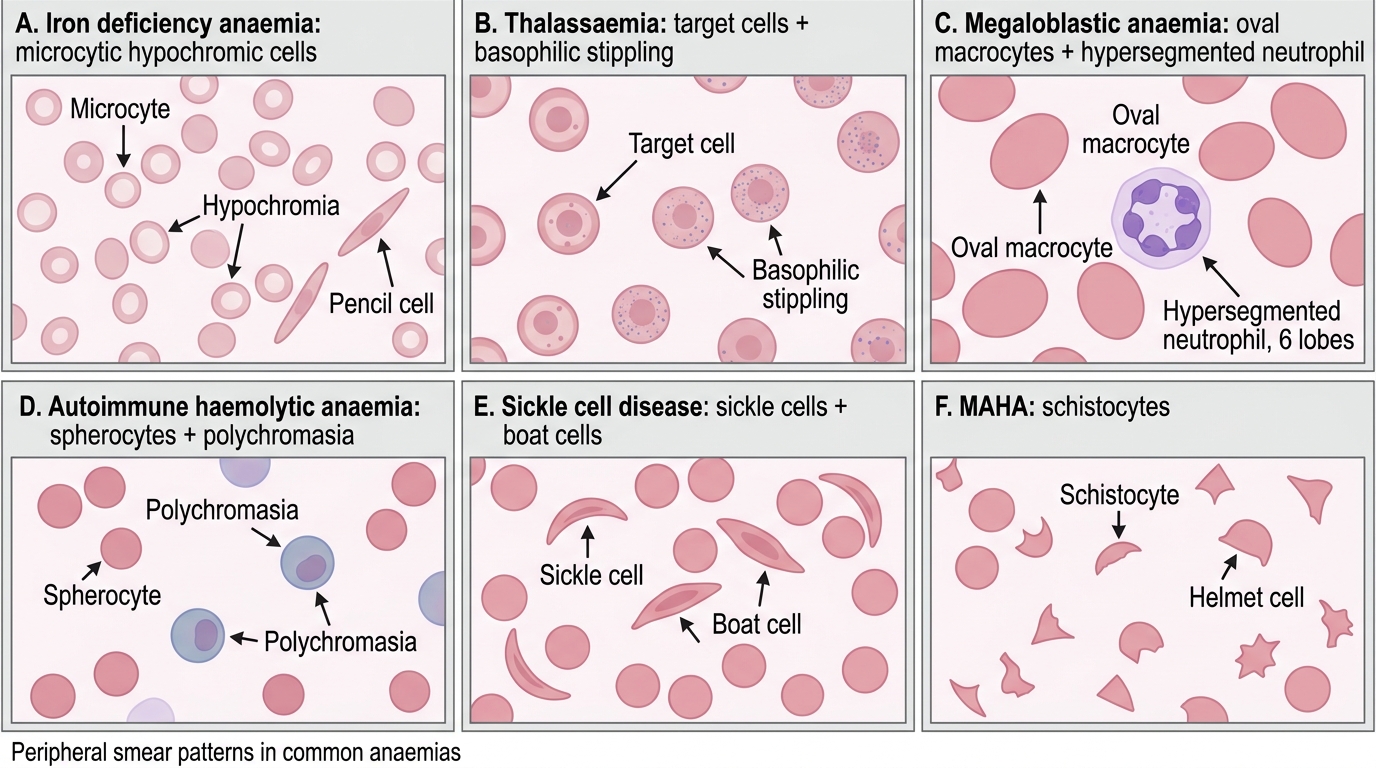
Peripheral Smear Patterns in Anaemia
SELF-CHECK
A 45-year-old vegetarian woman with type 2 diabetes on metformin for 8 years presents with fatigue. Her CBC shows Hb 9.8 g/dL and MCV 98 fL. The peripheral smear shows oval macrocytes and two neutrophils with 6 nuclear lobes each. What is the MOST likely underlying mechanism?
A. Folate deficiency from poor dietary intake alone
B. Vitamin B12 deficiency from metformin-induced impairment of ileal absorption
C. Iron deficiency from chronic subclinical menstrual loss
D. Myelodysplastic syndrome from prolonged metformin exposure
Reveal Answer
Answer: B. Vitamin B12 deficiency from metformin-induced impairment of ileal absorption
Metformin inhibits the ileal absorption of vitamin B12 by competing with the intrinsic factor-B12 complex for the cubam receptor, causing B12 deficiency after several years of use. A vegetarian diet also reduces dietary B12 intake. The combination of oval macrocytes and hypersegmented neutrophils (any neutrophil with ≥6 lobes or ≥5% with ≥5 lobes) is highly specific for megaloblastic anaemia from B12 or folate deficiency. In a metformin user of 8 years, B12 deficiency is the most likely single mechanism — confirmed by serum B12 level and, if borderline, serum methylmalonic acid. Iron deficiency causes microcytosis, not macrocytosis. MDS can cause macrocytosis but is a diagnosis of exclusion in an otherwise well patient with a clear risk factor for B12 deficiency.