Page 9 of 19
IM9.6-9 | Anaemia Diagnostic Testing — SDL Guide (Part 2)
Iron Studies — Pattern Interpretation for Microcytic Anaemia
Microcytic anaemia is the most common anaemia encountered in clinical practice in India, and the ability to differentiate its major causes — iron deficiency anaemia (IDA), anaemia of chronic disease (ACD), thalassaemia trait, and sideroblastic anaemia — using iron studies is a core diagnostic skill. The iron studies panel consists of four components, each measuring a different aspect of iron metabolism, and they must be interpreted as a pattern rather than as isolated values.
Serum iron measures the amount of iron bound to transferrin in the circulation. Normal range 60–160 µg/dL. Serum iron is LOW in both IDA and ACD, but NORMAL or HIGH in thalassaemia trait and sideroblastic anaemia (body iron stores are normal or increased in both these conditions). A critical limitation of serum iron is its high variability: it is subject to diurnal variation (higher in the morning), is affected by recent meals, and can be elevated by inflammatory states. For these reasons, serum iron alone is an unreliable diagnostic test and must always be interpreted alongside TIBC and ferritin.
Total Iron Binding Capacity (TIBC): The TIBC measures transferrin's ability to bind additional iron — effectively a proxy for the serum transferrin concentration. Normal range 250–370 µg/dL. TIBC is HIGH in IDA (the liver upregulates transferrin synthesis when iron stores are depleted, as a compensatory mechanism to scavenge more circulating iron) and LOW in ACD (transferrin synthesis is suppressed by inflammatory cytokines, especially interleukin-6 and hepcidin). TIBC is NORMAL in thalassaemia trait. This makes TIBC an important discriminator between the two most common causes of low serum iron.
Transferrin saturation (TSAT): Calculated as (serum iron ÷ TIBC) × 100. Normal 20–45%. TSAT is the proportion of transferrin molecules carrying iron at any given time. TSAT <16% is diagnostic of iron-restricted erythropoiesis, a state seen in both IDA and functional iron deficiency in ACD. In IDA, TSAT is typically <10%. In thalassaemia trait, TSAT is normal or elevated.
Serum ferritin: Ferritin is an iron-storage protein; serum ferritin reflects the body's total iron stores. It is the most clinically useful single iron test: ferritin <30 ng/mL is highly specific for iron deficiency (>99% specificity), and ferritin <12 ng/mL is diagnostic of iron deficiency in isolation. However, ferritin is an acute-phase reactant — it is elevated in infection, inflammation, liver disease, and malignancy, even when body iron stores are genuinely depleted. This is the critical limitation: a normal or high ferritin does NOT exclude iron deficiency in a patient with active inflammation. A ferritin of 80 ng/mL in a patient with rheumatoid arthritis may actually represent iron deficiency masked by inflammation. In such settings, soluble transferrin receptor (sTfR) — which rises in iron deficiency but is NOT an acute-phase reactant — or a bone marrow Prussian blue stain resolves the diagnosis.
| Parameter | IDA | ACD | Thalassaemia Trait | Sideroblastic Anaemia |
|---|---|---|---|---|
| Serum iron | Low | Low | Normal | High |
| TIBC | High | Low/Normal | Normal | Normal/Low |
| Transferrin saturation | Low (<16%) | Low (<16%) | Normal/High | High (>30%) |
| Serum ferritin | Low (<30) | Normal/High (>100) | Normal/High | High |
| MCV | Low | Low-normal | Low | Variable |
| RDW | High | Normal | Normal | Variable |
| Peripheral smear | Pencil cells, hypochromic | Normochromic, mild hypochromia | Target cells, stippling | Dimorphic RBCs |
The most common diagnostic challenge in India is distinguishing IDA from thalassaemia trait, particularly β-thalassaemia trait. The Mentzer index (MCV ÷ RBC count) provides a rapid screening tool: index <13 suggests thalassaemia; index >13 suggests IDA. However, Mentzer index has limited accuracy in mixed states and should always be followed by confirmatory haemoglobin electrophoresis — HbA2 elevation >3.5% confirms β-thalassaemia trait. Never start iron supplementation based on microcytosis alone without first confirming that iron stores are actually depleted — doing so causes inappropriate iron loading in thalassaemia patients.
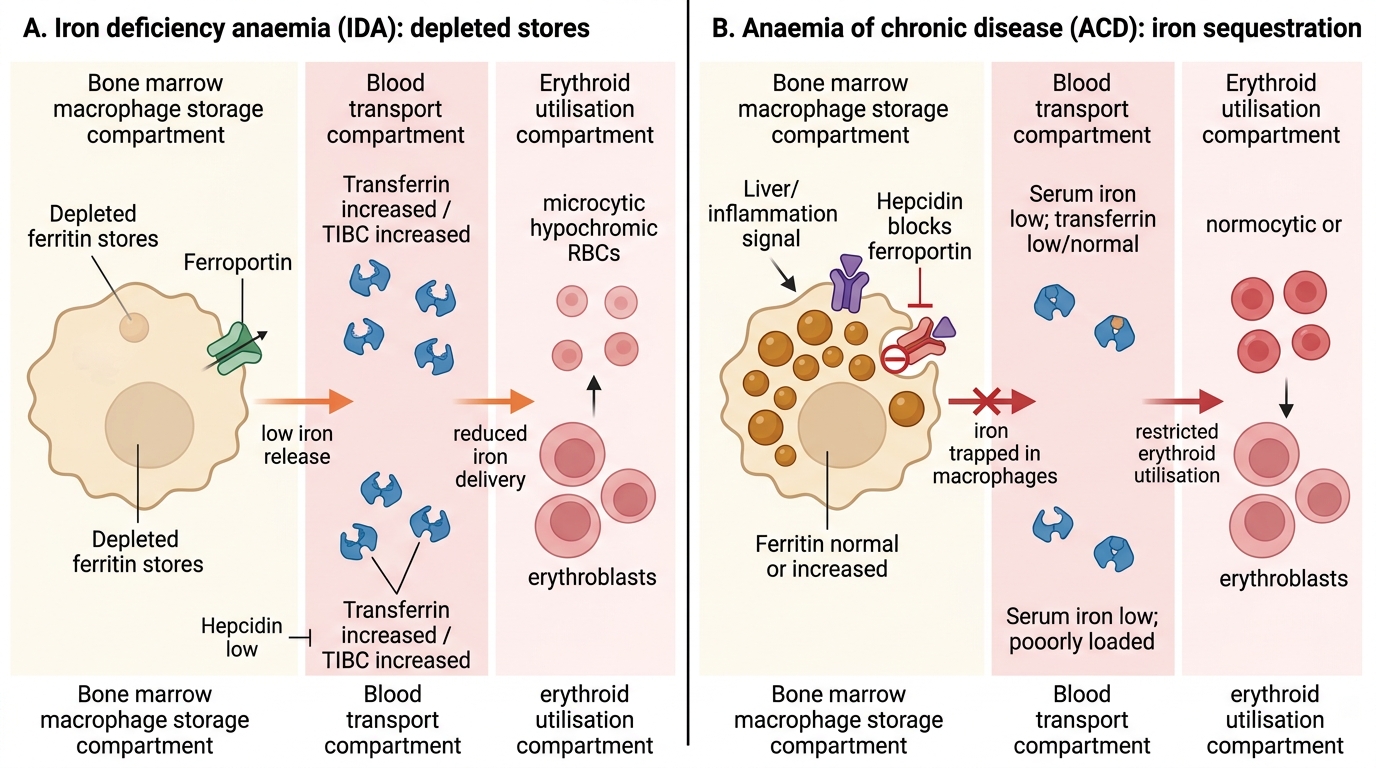
Iron Metabolism in IDA versus ACD
B12, Folate, and Haemolytic Markers — Interpretation
The investigations for macrocytic and haemolytic anaemias require understanding the biochemical pathways that each test reflects, because this determines how to handle borderline results and how to choose confirmatory tests when initial investigations are equivocal.
Serum vitamin B12: Measured by immunoassay. Normal range varies by laboratory but is typically >200 pg/mL (>148 pmol/L). B12 deficiency is strongly suggested by levels <200 pg/mL. Levels 200–300 pg/mL are borderline and require confirmation with metabolic markers. Importantly, serum B12 has poor sensitivity — up to 50% of patients with true B12 deficiency (demonstrated by metabolic markers) may have serum B12 levels in the low-normal range. When clinical suspicion is high — megaloblastic smear, long-term metformin, strict vegetarian diet, autoimmune conditions suggesting pernicious anaemia — a normal serum B12 does NOT exclude deficiency.
Confirmatory metabolic markers for B12 deficiency: Two functional markers confirm B12-deficient metabolism at the cellular level. First, serum methylmalonic acid (MMA): elevated in B12 deficiency (>0.4 µmol/L) because B12 is a required cofactor for methylmalonyl-CoA mutase. MMA is normal in folate deficiency alone. This makes MMA the most specific confirmatory test for B12 deficiency. Second, plasma homocysteine: elevated in both B12 and folate deficiency (>15 µmol/L), because both vitamins are required for remethylation of homocysteine to methionine. Elevated homocysteine with normal MMA therefore suggests folate rather than B12 deficiency. These metabolic markers are particularly useful when serum B12 levels are borderline (200–300 pg/mL).
Serum folate and red cell folate: Serum folate measures recent dietary intake and can be affected by a single day of dietary abstinence. Red cell folate is a better index of chronic folate status (normal >160 ng/mL). Anti-intrinsic factor antibodies (>50% sensitivity, >98% specificity) and anti-parietal cell antibodies (sensitive but less specific) are used to confirm pernicious anaemia as the cause of B12 deficiency, particularly relevant in patients without obvious dietary cause.
Haemolytic markers — the laboratory signature of red cell destruction: Haemolysis is confirmed by the combination of elevated red cell breakdown products and evidence of active bone marrow compensation.
Serum lactate dehydrogenase (LDH): LDH is released from ruptured red cells. Elevated in all haemolytic anaemias. LDH >2× upper limit of normal in severe intravascular haemolysis. Not specific to haemolysis — also elevated in myocardial infarction, liver disease, and tumour lysis — so must be interpreted alongside other markers.
Unconjugated (indirect) bilirubin: Red cell haemoglobin is catabolised to bilirubin by the reticuloendothelial system. Unconjugated bilirubin rises in haemolysis because the liver's conjugation capacity is overwhelmed. Unlike hepatic jaundice, in haemolytic anaemia the conjugated bilirubin is normal, there is no bilirubinuria, and the urine is normal colour unless there is concurrent intravascular haemolysis or liver disease.
Serum haptoglobin: Haptoglobin is an acute-phase protein that binds free haemoglobin released during intravascular haemolysis. The haptoglobin-haemoglobin complex is cleared by the liver. In intravascular haemolysis, haptoglobin is consumed and falls to undetectable levels. Haptoglobin <10 mg/dL (or undetectable) is the most sensitive marker of intravascular haemolysis. Caution: haptoglobin may be falsely elevated in inflammatory states (it is an acute-phase reactant), masking haemolysis; conversely, it is low in liver disease independent of haemolysis.
Plasma free haemoglobin and haemoglobinuria: Free haemoglobin in plasma (pink plasma) and haemoglobin in urine (dark brown-red urine, positive dipstick for blood but absent red cells on microscopy) confirm severe intravascular haemolysis. Haemosiderinuria (haemosiderin in urinary sediment, stained by Prussian blue) reflects chronic intravascular haemolysis such as occurs in paroxysmal nocturnal haemoglobinuria (PNH) and mechanical prosthetic valve haemolysis.
Reticulocyte count in haemolysis: Elevated reticulocyte count (reticulocytosis >3%) confirms that the bone marrow is compensating — an essential positive finding in haemolytic anaemia. Absence of reticulocytosis in a haemolytic picture should prompt consideration of aplastic crisis (e.g., parvovirus B19 infection superimposed on sickle cell disease or hereditary spherocytosis, suppressing marrow erythroid output).
Direct Coombs test (Direct Antiglobulin Test, DAT): Tests for antibody or complement coating on the patient's red cells. A positive DAT confirms autoimmune haemolytic anaemia (AIHA). AIHA can be warm (IgG antibodies reactive at 37°C) or cold (IgM antibodies reactive at 4°C). A negative DAT in haemolytic anaemia directs toward non-immune causes: hereditary spherocytosis, G6PD deficiency, sickle cell disease, thalassaemia, microangiopathic haemolysis.
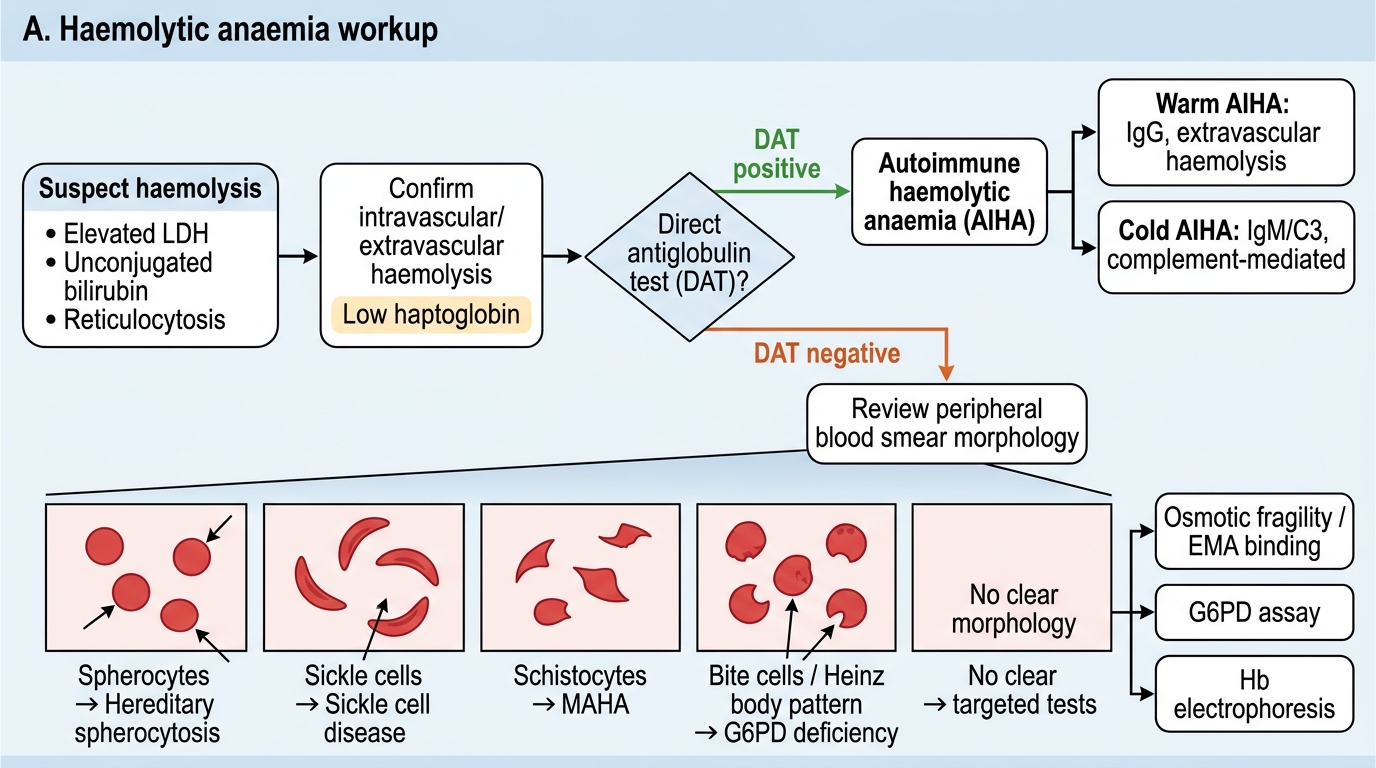
Haemolytic Anaemia Workup
SELF-CHECK
A 22-year-old man of Gujarati origin presents with Hb 8.2 g/dL, MCV 66 fL, RDW 12.8%, serum ferritin 85 ng/mL, serum iron 110 µg/dL, TIBC 260 µg/dL, and transferrin saturation 42%. He has no GI symptoms and no dietary restrictions. What is the MOST appropriate next investigation?
A. Trial of oral iron therapy for 6 weeks to confirm IDA by response
B. Upper GI endoscopy to identify an occult bleeding source
C. Haemoglobin electrophoresis to assess HbA2 level
D. Bone marrow aspiration to assess iron stores
Reveal Answer
Answer: C. Haemoglobin electrophoresis to assess HbA2 level
The investigation pattern here — microcytic anaemia with NORMAL ferritin, NORMAL serum iron, NORMAL TIBC, NORMAL-to-HIGH transferrin saturation, and critically NORMAL RDW — is the classic profile of thalassaemia trait rather than IDA. In IDA, ferritin would be low, TIBC would be high, and RDW would be elevated (reflecting progressive anisocytosis as iron stores deplete unevenly). The Gujarati ethnic background adds further prior probability for β-thalassaemia trait. Haemoglobin electrophoresis is the confirmatory test — HbA2 >3.5% confirms β-thalassaemia trait. Starting oral iron is inappropriate and potentially harmful (iron overload). Endoscopy is indicated for IDA in older patients with GI symptoms. BMA is not required at this stage.
Bone Marrow Aspiration and Biopsy — Indications and Findings
Bone marrow aspiration (BMA) and trephine biopsy are invasive procedures reserved for specific diagnostic situations where peripheral blood and serum investigations have been exhausted, or where marrow pathology is specifically suspected. Understanding the indications ensures that the procedure is ordered when it provides unique diagnostic value and not as a substitute for thoughtful interpretation of simpler tests.
Indications for bone marrow examination in anaemia:
First, unexplained cytopaenia — anaemia (or anaemia combined with thrombocytopaenia or leucopaenia, i.e., pancytopaenia) that remains undiagnosed after thorough peripheral workup. The classic example is aplastic anaemia — pancytopaenia with a hypocellular marrow (marrow cellularity <25%) — which cannot be diagnosed without a trephine biopsy showing the hypocellular marrow architecture.
Second, suspected haematological malignancy — acute leukaemia (blasts >20% on BMA = AML or ALL per WHO criteria), lymphoma with marrow involvement, multiple myeloma (plasma cell >10% on BMA), myelodysplastic syndrome (MDS). In MDS, the marrow shows dysplastic changes including ringed sideroblasts, abnormal megakaryocytes, and dysplastic erythropoiesis, along with cytogenetic abnormalities detectable only on BMA with cytochemistry and karyotyping.
Third, suspected myelofibrosis — the marrow is fibrosed and aspiration typically yields a 'dry tap' (no particles aspirated); diagnosis requires a trephine biopsy with reticulin stain showing increased reticulin fibrosis. The peripheral smear shows a leukoerythroblastic picture (immature white cells and nucleated red cells in peripheral blood) and tear-drop cells (dacrocytes) — a pattern indicating marrow infiltration or fibrosis.
Fourth, suspected bone marrow infiltration — by tuberculosis (granulomas on BMA or trephine with caseating necrosis), metastatic malignancy from solid tumours (breast, prostate, lung), or storage diseases such as Gaucher disease (lipid-laden Gaucher cells with wrinkled tissue-paper cytoplasm on BMA).
Fifth, iron stores assessment when ferritin is unreliable — when serum ferritin is elevated by inflammation (ACD vs IDA differentiation in a patient with chronic disease). Prussian blue staining of BMA smears directly visualises iron stores — absent stainable iron confirms IDA; normal or increased iron confirms ACD or thalassaemia. Ringed sideroblasts (erythroblasts with ≥5 iron granules encircling ≥1/3 of the nucleus on Prussian blue stain) confirm sideroblastic anaemia.
Procedure overview: The posterior superior iliac spine (PSIS) is the standard site in adults. Under local anaesthesia, the Salah needle (aspiration) or Jamshidi needle (trephine biopsy) is advanced through the outer cortex into the marrow cavity. Aspiration yields 1–2 mL of marrow blood; the trephine provides a core of cancellous bone 1–2 cm long for histological assessment. The sternal site may be used for aspiration only (not biopsy) when the PSIS is inaccessible. Complications are rare: local haematoma, infection, and — with sternal aspiration — accidental mediastinal penetration.
Interpretation of BMA: The smear is examined for: (1) cellularity — the M:E (myeloid to erythroid) ratio (normal 3:1–4:1); (2) erythropoiesis — megaloblastic changes in B12 or folate deficiency (large erythroid precursors with open, fine chromatin and asynchronous nuclear-cytoplasmic maturation); (3) myelopoiesis — maturation arrest in acute leukaemia; (4) megakaryocyte morphology; (5) abnormal cells — plasma cells, granulomas, metastatic deposits; (6) iron stores by Prussian blue stain.
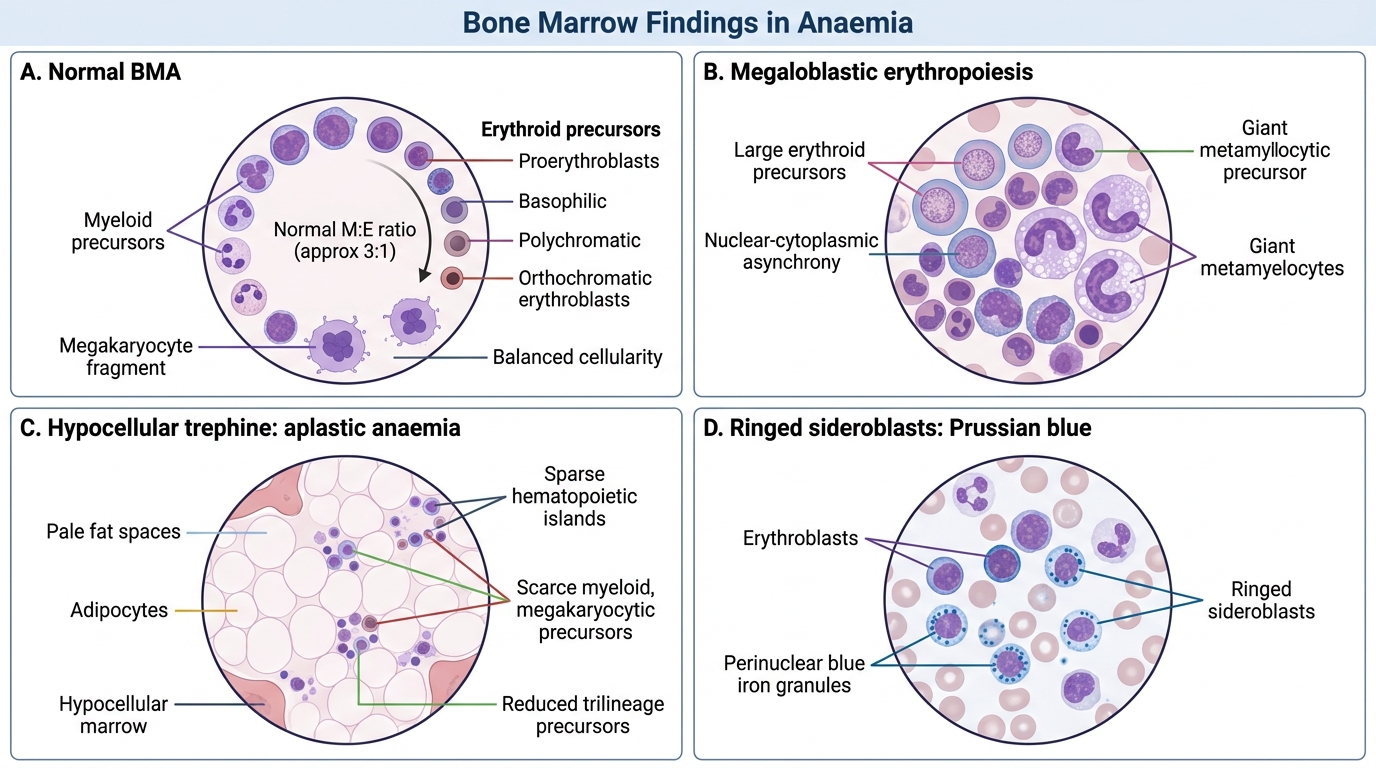
Bone Marrow Findings in Anaemia