Page 12 of 19
IM9.10-17 | Anaemia Treatment Prevention and Transfusion — SDL Guide
Learning Objectives
- Prescribe and counsel patients on replacement therapy for iron deficiency (oral and parenteral iron), B12 deficiency (IM and oral), and folate deficiency, including dose, duration, expected response, and side effects (IM9.10)
- Describe the national programmes for anaemia prevention including AMB, WIFS, and antenatal IFA supplementation, with specific populations, doses, and frequencies (IM9.11)
- Communicate the diagnosis and treatment plan for anaemia to patients in clear, accessible language addressing key side effects, adherence, and follow-up (IM9.12)
- Incorporate patient preferences, beliefs, and practical barriers into individualised anaemia management decisions (IM9.13)
- Describe the indications for blood transfusion and appropriate use of blood components including PRBC, FFP, platelets, and cryoprecipitate (IM9.14)
- Describe and apply the pre-transfusion safety checks and recognise and manage common transfusion adverse reactions (IM9.15)
- Counsel patients on dietary and behavioural strategies to prevent nutritional anaemia (IM9.16)
- Identify clinical situations in anaemia management requiring specialist referral and justify the appropriate referral pathway (IM9.17)
INSTRUCTIONS
Anaemia is common in Indian clinical practice, and its correct management depends on cause-specific treatment, appropriate use of blood transfusion, patient communication, and knowledge of national prevention programmes. This module builds from the treatment decisions for individual patients through the population-level programme context in which every Indian physician operates. It also addresses the patient communication and shared decision-making skills that determine whether the technically correct treatment is actually received.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 99 — Anaemia and Polycythaemia (textbook)
- API Textbook of Medicine, 10th ed. — Anaemia chapter (textbook)
- National Health Mission — WIFS Programme Guidelines, Ministry of Health and Family Welfare, India (guideline)
- KDIGO Clinical Practice Guideline for Anaemia in Chronic Kidney Disease, 2012 (update 2019) (guideline)
- British Society for Haematology Guideline on Blood Transfusion (guideline)
- Anaemia Mukt Bharat (AMB) Implementation Framework, POSHAN Abhiyaan, Ministry of Health and Family Welfare (national_programme)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman from a rural district in Madhya Pradesh presents to the district hospital with extreme fatigue, palpitations, and presyncope. Her haemoglobin is 4.8 g/dL — severely anaemic by any definition. She has been taking ferrous sulphate tablets prescribed at an antenatal visit, but only intermittently because they cause nausea. She is not pregnant now but has had three pregnancies in four years. The junior doctor on duty wants to transfuse her immediately. The senior consultant asks: is transfusion the right treatment here? The Hb is 4.8, but the anaemia is iron deficiency — it developed slowly and the patient is haemodynamically stable. Transfusing packed red cells provides a temporary fix and carries real risks — infection, transfusion reactions, sensitisation — while doing nothing to replenish her depleted iron stores. The correct treatment is parenteral iron, with transfusion reserved only if she develops haemodynamic compromise. This decision — when to transfuse versus when to treat the underlying cause and allow the marrow to respond — is one of the most clinically consequential in the management of anaemia. It is also one of the most frequently got wrong, in both directions: unnecessary transfusions in compensated chronic anaemia, and delayed transfusion in acute haemorrhagic shock. This module builds the framework to get it right every time.
WHY THIS MATTERS
Anaemia management is one of the highest-impact skills a final-year MBBS student can develop, because anaemia is ubiquitous in Indian clinical practice — affecting patients in every speciality, from the anaemic diabetic with ACD to the obstetric patient with severe IDA to the haematology ward patient with aplastic anaemia awaiting transplant. India also has extensive national programmes for anaemia prevention — POSHAN 2.0, ANAEMIA MUKT BHARAT under the National Health Mission, WIFS (Weekly Iron and Folic Acid Supplementation) — that every practitioner should know and counsel patients about. Beyond pharmacological replacement, the skills of patient communication (IM9.12, IM9.13, IM9.16) are explicitly examined at the NMC level, because a technically correct treatment plan that the patient does not understand or accept will fail. And blood transfusion — with its indications, component selection, pretransfusion checks, and adverse reaction management — is a core procedural competency with direct patient safety implications.
RECALL
Recall that anaemia is classified morphologically by MCV (microcytic/normocytic/macrocytic) and kinetically by RPI (hypo- vs hyperproliferative). The correct treatment depends entirely on the correct diagnosis. Recall the major mechanisms: iron deficiency anaemia (IDA) arises from inadequate intake, impaired absorption, or chronic blood loss; megaloblastic anaemia from deficiency of vitamin B12 or folate, both essential for DNA synthesis in rapidly dividing erythroid precursors; anaemia of chronic disease (ACD) from hepcidin-mediated iron sequestration and erythropoiesis suppression by inflammatory cytokines; haemolytic anaemia from premature red cell destruction; aplastic anaemia from bone marrow failure. Each mechanism has a specific, matched treatment. Treating IDA with B12 is ineffective; treating ACD with iron alone is insufficient; transfusing a megaloblastic patient without also replacing the deficient vitamin corrects the haemoglobin temporarily but does nothing for the neurological complications of B12 deficiency. The principle of mechanism-specific treatment underpins everything in this module.
Clinical Presentations Requiring Treatment Decisions
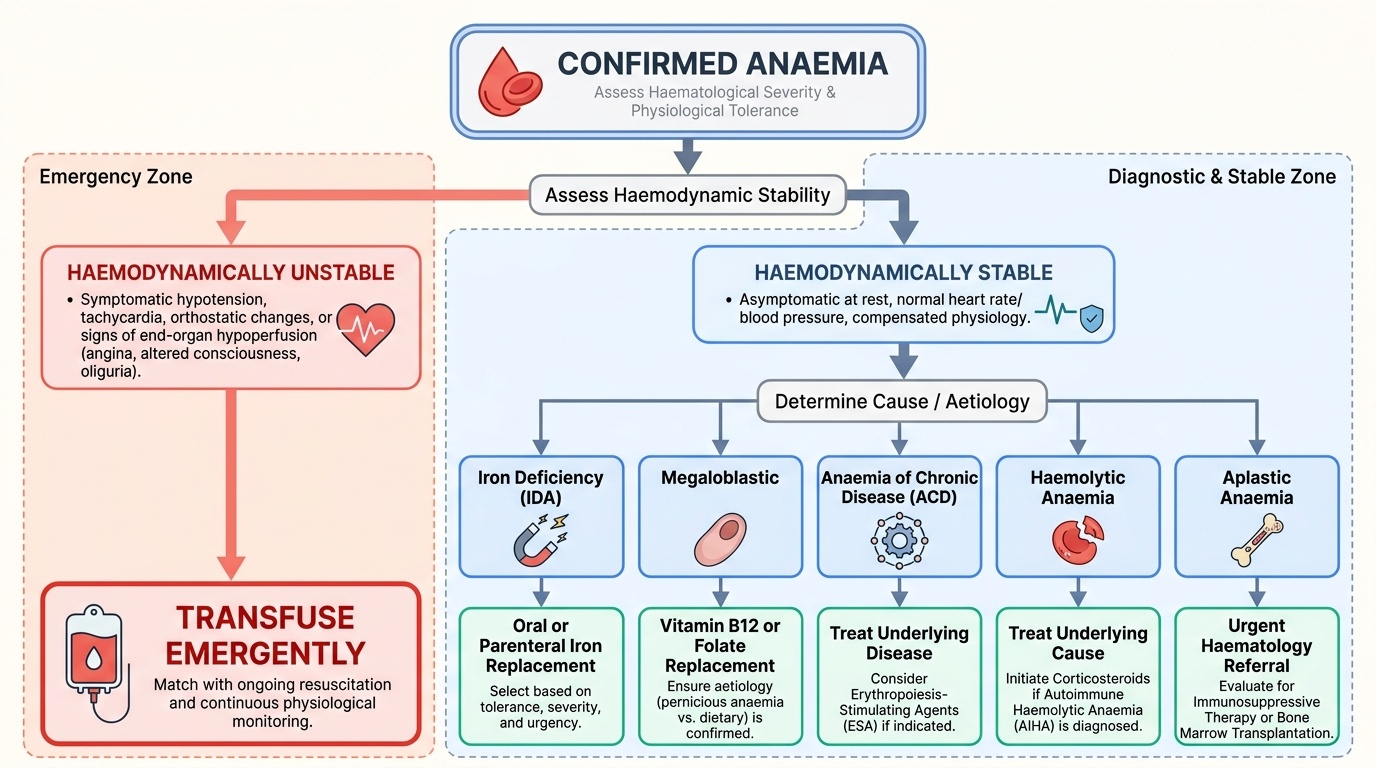
Before choosing a treatment, the clinician must assess two independent but complementary dimensions: haematological severity (how low is the haemoglobin and how quickly is it falling) and physiological tolerance (how well is the patient compensating cardiovascularly for the anaemia). These two dimensions together — not haemoglobin number alone — determine whether the patient needs urgent intervention, and what form that intervention should take.
Provided image
Haematological severity is stratified by haemoglobin level: mild (Hb 10.0–12.9/11.9 g/dL for men/women), moderate (7.0–9.9 g/dL), severe (<7.0 g/dL), and very severe (<4.0 g/dL, sometimes called critical anaemia). The rate of fall matters as much as the absolute level — a haemoglobin that has fallen from 14 to 7 g/dL over 24 hours (acute haemorrhage) is a clinical emergency; the same haemoglobin reached over 6 months (chronic IDA) may be well tolerated by a resting patient with a normal resting heart rate and no orthostatic symptoms.
Physiological compensation for anaemia involves increased cardiac output (tachycardia, increased stroke volume), rightward shift of the oxygen-haemoglobin dissociation curve (facilitated by elevated 2,3-DPG), redistribution of blood flow to vital organs, and increased oxygen extraction at the tissues. These mechanisms are robust in young, previously healthy individuals but are severely limited in patients with coronary artery disease, heart failure, severe chronic lung disease, or cerebrovascular disease. A 70-year-old man with triple-vessel coronary disease may develop angina at a haemoglobin of 9 g/dL, whereas a young woman with chronic haemolytic anaemia may be asymptomatic at the same level.
The treatment decision framework therefore follows: (1) Identify the cause of anaemia (morphological and aetiological classification, as covered in the previous modules); (2) Assess haemodynamic stability — heart rate, blood pressure, orthostatic hypotension, signs of end-organ hypoperfusion (altered consciousness, oliguria, angina); (3) Match treatment to mechanism — replacement therapy for deficiency states; (4) Decide whether transfusion is needed emergently (haemodynamic compromise) or whether time can be allowed for specific treatment (replacement therapy) to work; (5) Engage the patient in understanding the diagnosis and the treatment plan — this is not a supplementary step but a core component of competent anaemia care.
The most common errors in this decision framework are: transfusing a haemodynamically stable patient with chronic compensated anaemia when specific treatment would suffice; prescribing iron without first confirming iron deficiency (and thereby loading iron in thalassaemia trait); and discharging a patient with a prescription without any counselling about why the treatment is needed, how to take it, expected side effects, and when to return.
Replacement Therapy — Iron, B12, and Folate
Replacement therapy for deficiency-state anaemias is the most commonly performed treatment for anaemia in India. Prescribing it correctly — including the right preparation, right dose, right route, right duration, and appropriate counselling — is a core competency at the NMC level (IM9.10, IM9.16).
Provided image
Iron replacement therapy:
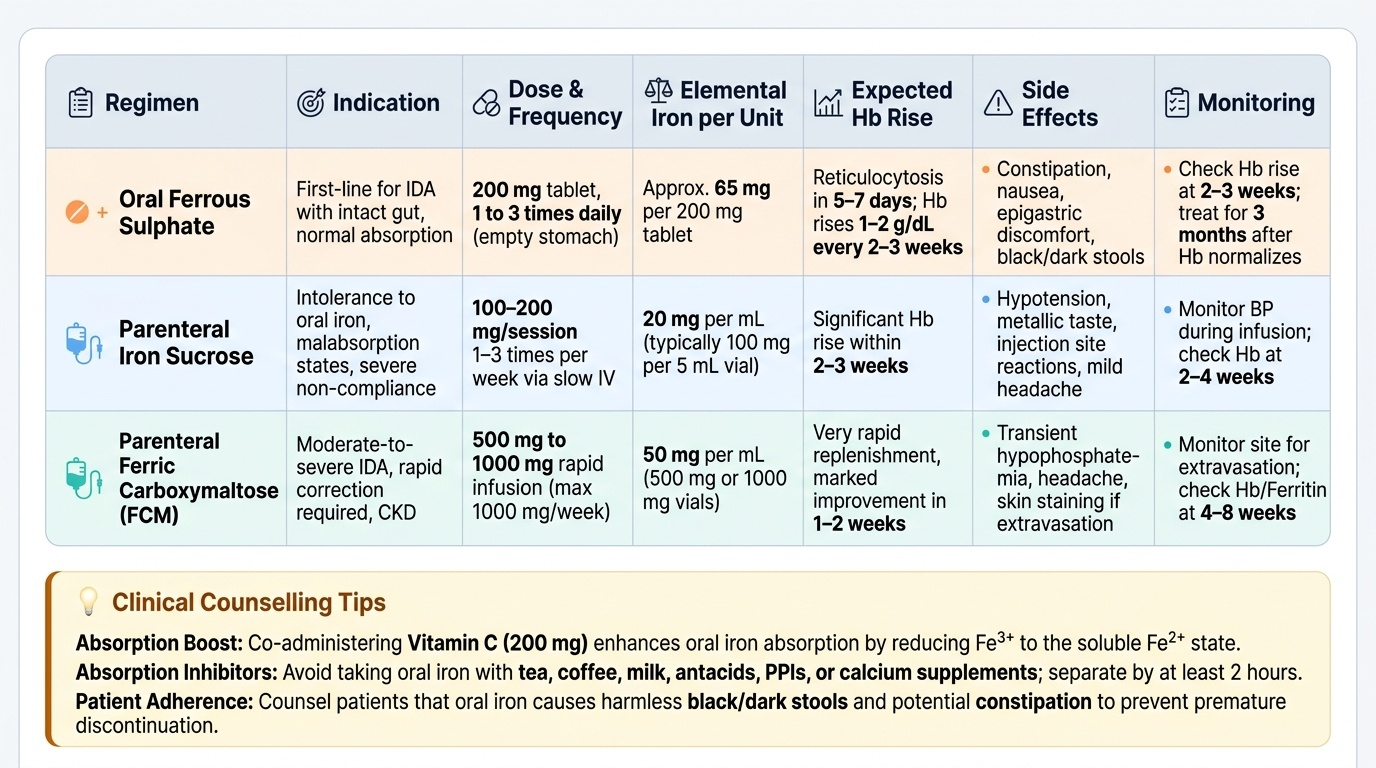
Oral iron is the first-line treatment for IDA when the gut is intact and absorption is expected to be normal. The standard preparation is ferrous sulphate 200 mg (containing approximately 65 mg of elemental iron) given orally, once daily on an empty stomach (absorption is approximately 30% better in the fasting state than with food). The recommended elemental iron dose for treatment of IDA in adults is 150–200 mg elemental iron per day, typically achieved with one ferrous sulphate 200 mg tablet two to three times daily. Alternatively, ferrous gluconate and ferrous fumarate are gentler on the GI tract but contain less elemental iron per tablet. A practical point of crucial importance for patient counselling: vitamin C (ascorbic acid, 200 mg) taken simultaneously enhances iron absorption by reducing Fe³⁺ to the more soluble Fe²⁺ form and by acidifying the local gastric environment. Conversely, tea, coffee, milk, antacids, proton pump inhibitors, and calcium supplements all reduce iron absorption and should be taken several hours apart from iron.
Common side effects of oral iron that must be explained to patients before prescribing: constipation and hard stools (very common — recommend dietary fibre and adequate fluid intake), nausea and epigastric discomfort (reduced by taking iron with a small amount of food, though this reduces absorption), black or dark stools (harmless — explain this to prevent alarm), and temporary staining of teeth (with liquid preparations — drink through a straw). Failure to explain these effects is the single most common reason patients discontinue iron therapy prematurely.
Expected response to oral iron: Reticulocytosis appears within 5–7 days of starting therapy (the first objective marker of marrow response). Haemoglobin begins rising within 2 weeks. The haemoglobin should rise by approximately 1–2 g/dL every 2–3 weeks with adequate dosing. Duration of therapy: 3 months after haemoglobin normalisation is the standard recommendation to replenish iron stores — the common error is stopping iron as soon as the haemoglobin reaches normal (stores remain depleted). In iron-refractory IDA (no Hb rise >1 g/dL after 4 weeks of adequate oral iron), consider: non-compliance, ongoing blood loss, malabsorption (coeliac disease, H. pylori gastritis), incorrect diagnosis (thalassaemia), or a need for parenteral iron.
Parenteral iron is indicated when: (1) oral iron is not tolerated or absorbed (malabsorption syndromes, post-bariatric surgery, inflammatory bowel disease); (2) rapid repletion is required (pre-operative optimisation, end-stage renal disease on haemodialysis); (3) ongoing losses exceed what oral iron can replace; (4) patient non-compliance with oral iron is documented. The available formulations in India include ferric carboxymaltose (FCM), iron sucrose, and low-molecular-weight iron dextran. FCM has the advantage of allowing large doses (750–1000 mg) to be given as a single infusion. The required total dose is calculated using the Ganzoni formula: total iron deficit (mg) = weight (kg) × (target Hb − actual Hb) × 2.4 + 500 (mg for stores). Parenteral iron carries a risk of acute hypersensitivity reactions (anaphylaxis, especially with iron dextran); a test dose is given first with resuscitation facilities immediately available.
Vitamin B12 replacement:
The standard treatment for B12 deficiency, especially when neurological complications are present or absorption is impaired, is intramuscular (IM) cyanocobalamin or hydroxocobalamin. A typical regimen for treatment of confirmed deficiency: 1000 µg IM daily for 7 days (loading phase), then 1000 µg IM weekly for 4 weeks, then 1000 µg IM monthly for life (if the cause is absorptive failure, as in pernicious anaemia or post-gastrectomy). For dietary B12 deficiency in vegetarians without absorption problems, oral cyanocobalamin 500–1000 µg daily is effective because approximately 1% of oral B12 is absorbed passively without intrinsic factor, even in pernicious anaemia — making high-dose oral B12 a viable alternative for patients who cannot tolerate injections. The haematological response is rapid: reticulocytosis peaks at 5–7 days; haemoglobin normalises within 6–8 weeks. Neurological recovery is slower and may be incomplete — this underscores the importance of diagnosing and treating B12 deficiency before neurological involvement (subacute combined degeneration of the cord) occurs. An important clinical trap: if B12 deficiency and concurrent iron deficiency are both present (as often seen in malabsorptive conditions), the haemoglobin response to B12 replacement may be blunted unless iron is also supplemented — because the rapidly responding erythroid precursors will outstrip iron supply. Hypokalemia can develop as a side effect of B12 replacement (potassium is taken up rapidly by newly proliferating erythroid cells) — monitor electrolytes, especially in severely anaemic patients.
Folic acid replacement:
Folic acid deficiency is treated with oral folic acid 5 mg once daily for 4 months (or longer if the underlying cause persists). Folic acid is an important preventive supplement: 5 mg folic acid per day is recommended periconceptionally (from 3 months before conception to the end of the first trimester) to prevent neural tube defects (NTDs) — spina bifida and anencephaly. The standard recommendation in India, aligned with WHO guidance, is 400 µg (0.4 mg) daily for women without prior NTD history and 5 mg daily for women with a prior NTD-affected pregnancy or other risk factors. A critical point: never give folic acid alone to treat macrocytic anaemia without first excluding B12 deficiency. Folic acid can partially correct the haematological abnormalities of B12 deficiency while allowing subacute combined degeneration of the spinal cord to progress silently — this is the classic neurological catastrophe of empirical folate therapy.
SELF-CHECK
A 35-year-old woman with confirmed iron deficiency anaemia (Hb 8.2 g/dL) is started on ferrous sulphate 200 mg three times daily. After 4 weeks she returns with Hb 8.0 g/dL — essentially unchanged. She denies missing any doses. Which is the MOST important next step?
A. Switch to parenteral iron immediately as oral iron has failed
B. Add vitamin C 200 mg with each dose and check for ongoing blood loss, malabsorption, or incorrect diagnosis
C. Double the dose of ferrous sulphate to 400 mg three times daily
D. Arrange a bone marrow aspiration to exclude aplastic anaemia
Reveal Answer
Answer: B. Add vitamin C 200 mg with each dose and check for ongoing blood loss, malabsorption, or incorrect diagnosis
Before declaring oral iron failure and escalating to parenteral iron, the clinician must systematically check for modifiable causes of non-response: (1) Is absorption impaired? Check for coeliac disease (anti-endomysial antibodies, anti-tTG), H. pylori gastritis, inflammatory bowel disease, or any PPI use (reduces gastric acid needed for iron reduction); (2) Is there ongoing blood loss exceeding replacement? Check stool occult blood; (3) Is the diagnosis correct? Thalassaemia trait, ACD, and sideroblastic anaemia do not respond to iron; (4) Is vitamin C being co-administered to enhance absorption? Doubling the dose increases side effects without improving absorption efficiently. BMA is not indicated at this stage. Parenteral iron is appropriate after these reversible factors have been addressed and found absent.
National Anaemia Prevention Programmes and Prophylaxis
India has a high burden of nutritional anaemia that is largely preventable, and the national programmes for anaemia prevention are both a competency requirement (IM9.11) and a reflection of the public health context in which every Indian physician practises. Understanding these programmes allows the clinician to counsel patients appropriately and to identify which populations should be receiving which preventive interventions.
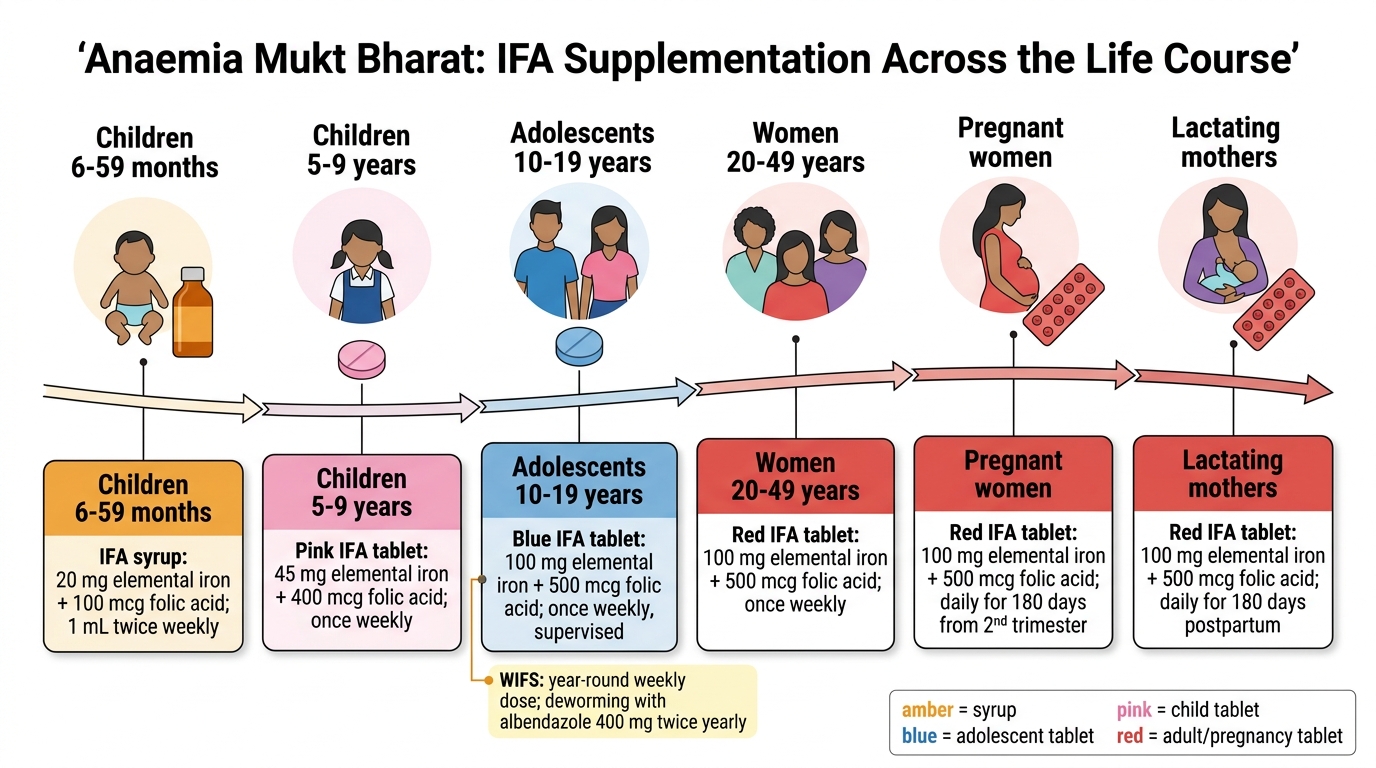
Anaemia Mukt Bharat (AMB) — the umbrella strategy: Launched in 2018 as a component of POSHAN Abhiyaan (National Nutrition Mission), AMB addresses anaemia across all life stages through a 6×6×6 strategy — targeting six population beneficiary groups (children 6–59 months, children 5–9 years, adolescents 10–19 years, pregnant women, lactating mothers, and women of reproductive age 15–49 years) through six interventions (prophylactic iron and folic acid supplementation, deworming, addressing non-nutritional causes of anaemia, testing and treating malaria where applicable, and behaviour change communication) delivered through six institutional platforms (health and wellness centres, school health programmes, antenatal care, ICDS, nutrition rehabilitation, digital tools for tracking).
Weekly Iron and Folic Acid Supplementation (WIFS) Programme: WIFS is one of the cornerstone AMB interventions, targeting school-going adolescents and adolescents out of school. Under WIFS, adolescents receive weekly supervised doses of Iron Folic Acid (IFA) tablets — specifically 100 mg elemental iron plus 500 µg folic acid — once weekly, year-round. The weekly (rather than daily) schedule is used because it improves adherence and reduces gastrointestinal side effects, while evidence from meta-analyses (Cochrane, 2011 and updates) shows that weekly supplementation achieves haemoglobin improvements comparable to daily dosing in populations with high anaemia prevalence. The IFA tablets are distributed through schools and AWC (Anganwadi Centres). Supervised consumption on one day per week (typically Monday) is the recommended approach to ensure compliance. Biannual albendazole deworming (400 mg single dose, twice yearly) is co-administered because intestinal helminthiasis (Ascaris, hookworm) causes significant iron loss and impairs absorption.
Iron and Folic Acid supplementation during pregnancy: Under the National Iron Plus Initiative (NIPI) within the NHM framework, all pregnant women receive IFA supplementation starting at 12 weeks of gestation (or as early as the first ANC visit): one tablet of 100 mg elemental iron + 500 µg folic acid daily throughout pregnancy and for 180 days postpartum. The rationale is that iron requirements increase dramatically in pregnancy — from 18 mg/day in non-pregnant women to approximately 27–30 mg/day in the third trimester — and dietary sources alone are almost never sufficient in the Indian context. Folic acid supplementation prevents neural tube defects (the critical window being periconceptional — ideally started 3 months before conception). Haemoglobin is measured at each ANC visit (at 12–14, 18–20, 26–28, and 32–34 weeks); if Hb falls below 11 g/dL, treatment doses of oral iron are added.
Universal salt iodisation addresses coexisting iodine deficiency (a cofactor in thyroid dysfunction that can worsen anaemia) through mandatory iodisation of edible salt under the National Iodine Deficiency Disorders Control Programme (NIDDCP).
Dietary counselling for anaemia prevention (IM9.16) is a communication skill component of the competency. Key messages for patient counselling: increase consumption of iron-rich foods — dark leafy vegetables (spinach, fenugreek), legumes (dal, rajma), sesame seeds, jaggery; consume vitamin C-rich foods (amla, citrus, tomato) simultaneously with iron-rich meals to enhance non-haem iron absorption; avoid tea and coffee with meals; cook in iron utensils where practical; ensure adequate protein intake (red meat, fish, eggs, pulses) for haem iron and complete protein. For B12: dairy products and eggs are adequate for lacto-ovo vegetarians; strict vegans need B12-fortified foods or supplementation.
Anaemia Mukt Bharat IFA Schedule Across the Life Course
SELF-CHECK
Under the National Iron Plus Initiative, which iron and folic acid supplementation is recommended for ALL adolescent girls (10–19 years) attending school in India?
A. Daily ferrous sulphate 200 mg plus folic acid 5 mg throughout the school year
B. Weekly IFA tablet containing 100 mg elemental iron plus 500 µg folic acid, year-round under supervision
C. Monthly parenteral iron injection plus oral folic acid 5 mg for 3 months
D. Iron supplementation only when haemoglobin falls below 11 g/dL on routine screening
Reveal Answer
Answer: B. Weekly IFA tablet containing 100 mg elemental iron plus 500 µg folic acid, year-round under supervision
The WIFS (Weekly Iron and Folic Acid Supplementation) programme under Anaemia Mukt Bharat prescribes weekly IFA tablets containing 100 mg elemental iron plus 500 µg folic acid, given year-round to adolescent girls (10–19 years) through schools. The weekly schedule improves adherence and tolerability compared to daily dosing, while achieving comparable haemoglobin improvement in populations with high baseline anaemia prevalence. Supervised consumption on one day per week (typically Monday) ensures compliance. Biannual deworming with albendazole 400 mg is co-administered. Daily dosing at treatment doses (ferrous sulphate 200 mg three times daily) is for treatment of confirmed IDA, not universal prophylaxis in adolescents.