Page 13 of 19
IM9.10-17 | Anaemia Treatment Prevention and Transfusion — SDL Guide (Part 2)
Blood Transfusion — Indications, Components, and Safe Practice
Blood transfusion is a powerful therapeutic intervention that can be life-saving in acute haemorrhage and severe symptomatic anaemia, but it carries real risks and should never be administered without a clear clinical indication. Inappropriate transfusion — giving blood when specific medical therapy would suffice — exposes the patient to avoidable hazards including transfusion-transmitted infections, haemolytic reactions, alloimmunisation, TRALI (transfusion-related acute lung injury), transfusion-associated circulatory overload (TACO), and immune modulation. The principle of restrictive transfusion — transfusing to achieve a haemoglobin sufficient for clinical stability rather than to achieve a normal haemoglobin — has strong evidence supporting it across multiple patient populations (TRICC trial for ICU patients; FOCUS trial for cardiac surgery patients).
Provided image
Indications for blood transfusion (IM9.14):
Acute haemorrhage with haemodynamic instability: When a patient is in haemorrhagic shock (tachycardia, hypotension, pallor, diaphoresis, altered consciousness) from acute blood loss — postpartum haemorrhage, GI haemorrhage, trauma — blood transfusion is the emergency intervention. The haemoglobin may initially appear falsely normal (haemoconcentration before haemodilution), so clinical haemodynamic signs take precedence over haemoglobin number in the acute setting.
Symptomatic anaemia with specific physiological thresholds:
- Haemoglobin <7 g/dL in haemodynamically stable patients without cardiac disease: transfusion is generally indicated if symptoms (dyspnoea at rest, severe fatigue, dizziness) are present and are attributable to the anaemia.
- Haemoglobin <8 g/dL in patients with known cardiovascular disease (coronary artery disease, heart failure, cerebrovascular disease), or in post-operative patients, or in patients who are symptomatic at higher Hb levels.
- Haemoglobin <9–10 g/dL in patients who are haemodynamically compromised by anaemia (e.g., active angina, dyspnoea at minimal exertion).
- Specific clinical contexts where higher thresholds apply: patients with sickle cell disease in acute chest syndrome (target Hb 10 g/dL for simple transfusion or exchange transfusion to reduce HbS%); patients with aplastic anaemia (Hb threshold guided by symptoms); thalassaemia major (chronic regular transfusion programme targeting pre-transfusion Hb ≥9–10 g/dL to suppress ineffective erythropoiesis and prevent organ damage from extramedullary haematopoiesis).
When NOT to transfuse: A haemoglobin of 6.5 g/dL in a young woman with chronic well-compensated IDA who is haemodynamically stable and asymptomatic at rest should be treated with parenteral iron, not transfused. A haemoglobin of 8 g/dL in a patient with megaloblastic anaemia should be treated with B12 or folate replacement, not transfused. Transfusing these patients without addressing the underlying deficiency is not merely ineffective but potentially harmful.
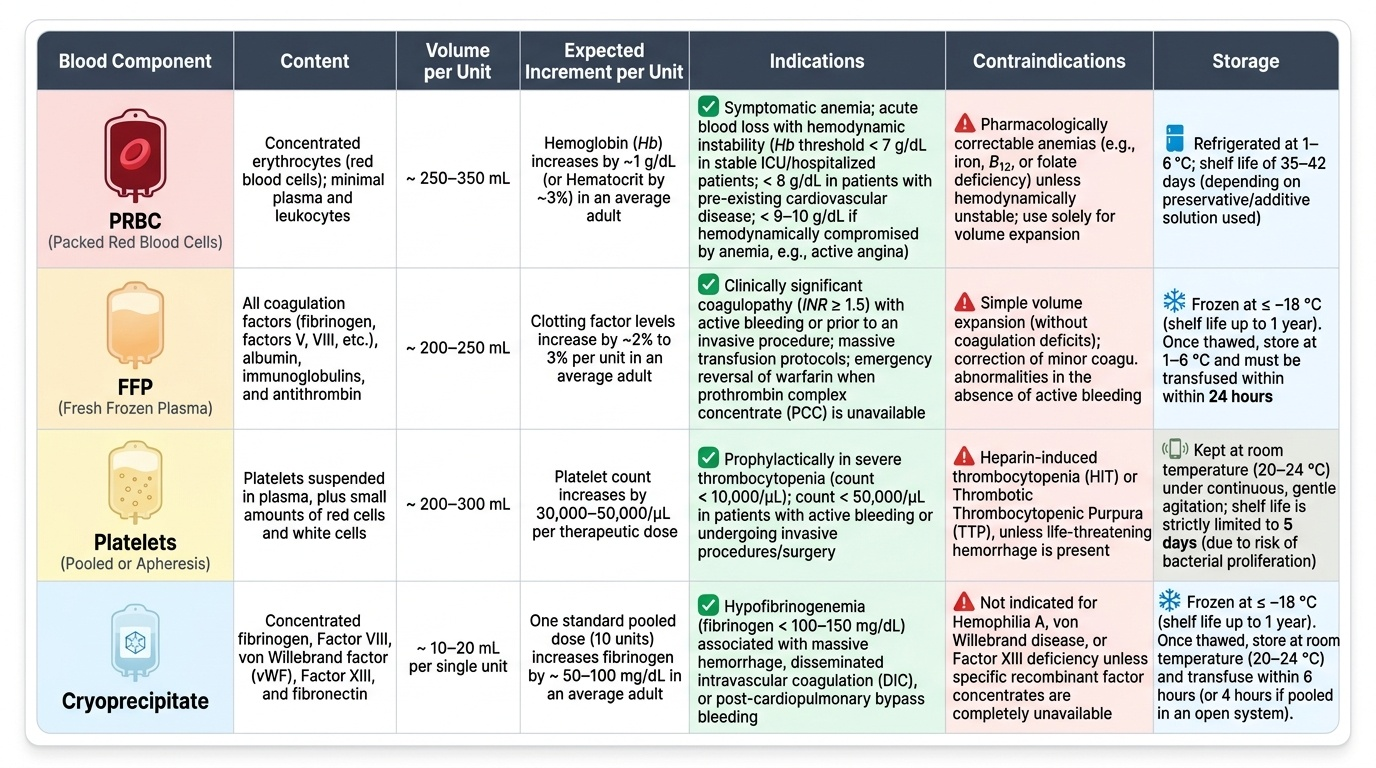
Blood components and their appropriate use (IM9.14):
Packed Red Blood Cells (PRBCs): Each unit contains approximately 200–250 mL of red cells in an additive solution (SAGM), with haematocrit approximately 55–65%. Expected haemoglobin rise: 1–1.5 g/dL per unit in a 70 kg adult. Indications: anaemia requiring red cell replacement. Storage: 2–6°C for up to 35–42 days.
Fresh Frozen Plasma (FFP): Contains all clotting factors. Indications: coagulopathy with active bleeding, reversal of warfarin (if Vitamin K is too slow), DIC with coagulopathy, TTP (plasma exchange), liver disease with factor deficiency. NOT indicated for volume expansion alone.
Platelets: Each platelet concentrate raises count by approximately 5,000–10,000/µL. Indications: thrombocytopaenic bleeding or prophylactic for counts <10,000/µL in stable patients, <20,000/µL before minor procedures, <50,000/µL before major surgery. NOT indicated in TTP or HIT (paradoxically worsens thrombosis).
Cryoprecipitate: Rich in fibrinogen, Factor VIII, vWF, and Factor XIII. Indications: hypofibrinogenaemia (<1.5 g/L) with active bleeding, haemophilia A and vWD where recombinant factors are unavailable.
Pre-transfusion checks and safety protocol (IM9.15): The pre-transfusion safety protocol is designed to prevent the most catastrophic transfusion error — giving the wrong blood to the wrong patient (ABO incompatibility leading to acute haemolytic transfusion reaction, which can be fatal). The mandatory steps are:
- Group and crossmatch: Type the recipient's ABO and RhD blood group; test for alloantibodies; crossmatch the donor unit against the recipient's serum to detect any incompatibility.
- Patient identification check at the bedside: BEFORE connecting the blood pack, verify — at minimum — three patient identifiers (full name, date of birth, hospital number or UID) against the patient's wristband AND the blood pack label AND the crossmatch report. This step must be done by two qualified personnel in most protocols.
- Check unit details: Confirm blood component type, unit number, ABO/RhD group on the pack label, and the expiry date.
- Vital signs: Record baseline temperature, pulse rate, and blood pressure before starting.
- Infusion rate: Start slowly — 10–20 drops/minute for the first 15 minutes while the patient is observed for early signs of a transfusion reaction. If no reaction, increase to the prescribed rate.
- Monitor during transfusion: Check temperature, pulse, BP, and respiratory rate at 15 minutes, 30 minutes, 1 hour, and at the end of each unit.
- Recognise and respond to adverse reactions (see below).
Adverse reactions to blood transfusion and their management:
Acute haemolytic transfusion reaction (AHTR): Most dangerous; usually from ABO incompatibility (wrong blood to wrong patient). Presents within minutes — severe loin pain, fever, rigors, haemoglobinuria, haemodynamic collapse, DIC. Action: STOP the transfusion immediately, maintain IV access, send blood and urine for testing, supportive care (fluid resuscitation, vasopressors, dialysis if AKI develops), report to blood bank.
Febrile non-haemolytic transfusion reaction (FNHTR): Most common reaction; caused by cytokines in stored blood or anti-leukocyte antibodies. Temperature rise >1°C during or within 4 hours of transfusion, with chills. Management: slow or stop transfusion, give paracetamol, resume at slower rate if fever resolves. Use leucodepleted blood products in future transfusions.
Allergic reaction: Urticaria, pruritis, flushing — from recipient antibodies against donor plasma proteins. Management: stop transfusion, give antihistamine (chlorpheniramine), restart at slower rate if symptoms resolve. Anaphylaxis (rare) requires adrenaline (epinephrine) 0.5 mg IM plus IV fluids and airway management.
TRALI (Transfusion-Related Acute Lung Injury): Presents as acute respiratory distress within 6 hours of transfusion, bilateral pulmonary infiltrates on CXR, without evidence of cardiac overload. Mechanism: donor anti-HLA or anti-neutrophil antibodies. Management: stop transfusion, supportive oxygen; TRALI typically resolves within 96 hours with supportive care.
TACO (Transfusion-Associated Circulatory Overload): Presents as hypertension, pulmonary oedema, respiratory distress within 6 hours. Risk is highest in elderly patients, CKD, or pre-existing heart failure. Prevention: transfuse slowly (over 4 hours per unit), give frusemide between units in high-risk patients.
SELF-CHECK
A 55-year-old woman is being transfused her second unit of packed red blood cells for symptomatic IDA (Hb 6.1 g/dL). Fifteen minutes into the second unit, she develops a temperature of 38.9°C (from a baseline of 37.1°C), rigors, and complains of lower back pain. Her blood pressure has fallen from 120/80 to 90/60 mmHg. What is the MOST appropriate IMMEDIATE action?
A. Give paracetamol and slow the infusion rate; this is a febrile non-haemolytic reaction
B. Give IV antihistamine (chlorpheniramine); this is an allergic reaction
C. Stop the transfusion immediately, maintain IV access with normal saline, and send blood and urine samples to the blood bank for testing
D. Increase the infusion rate to complete the unit quickly and monitor for further deterioration
Reveal Answer
Answer: C. Stop the transfusion immediately, maintain IV access with normal saline, and send blood and urine samples to the blood bank for testing
The combination of fever, rigors, lower back pain, and haemodynamic deterioration (BP fall) during transfusion is the classic presentation of an acute haemolytic transfusion reaction (AHTR) — most commonly caused by ABO incompatibility from patient identification error. This is a medical emergency. The transfusion must be STOPPED immediately. IV access is maintained with normal saline. Blood samples (the patient's and the blood pack unit) must be sent to the blood bank for re-crossmatch, and urine must be checked for haemoglobinuria. Supportive management includes IV fluids, vasopressors if needed, close monitoring for DIC, and dialysis if AKI develops. Paracetamol and slowing the infusion are appropriate for FNHTR, which does NOT cause haemodynamic compromise or back pain. An allergic reaction presents with urticaria and pruritis, not back pain and hypotension. Never increase the rate of a reaction-complicated transfusion.
Patient Communication, Counselling, and Shared Decision-Making
Effective patient communication in anaemia management is not an optional add-on to clinical care but a determinant of treatment outcome. A patient who does not understand why she needs to take iron tablets for 6 months after her haemoglobin normalises will stop at 3 months — and present again with IDA within a year. A patient who fears the side effects of iron (black stools, constipation) and was not forewarned will discontinue the medication and interpret the side effects as a disease progression. NMC competencies IM9.12 (communicating diagnosis and treatment) and IM9.13 (incorporating patient preferences) and IM9.16 (counselling for anaemia prevention) are explicitly patient-centred competencies, and they reflect the shift in medical education toward the biopsychosocial model of care.
Provided image
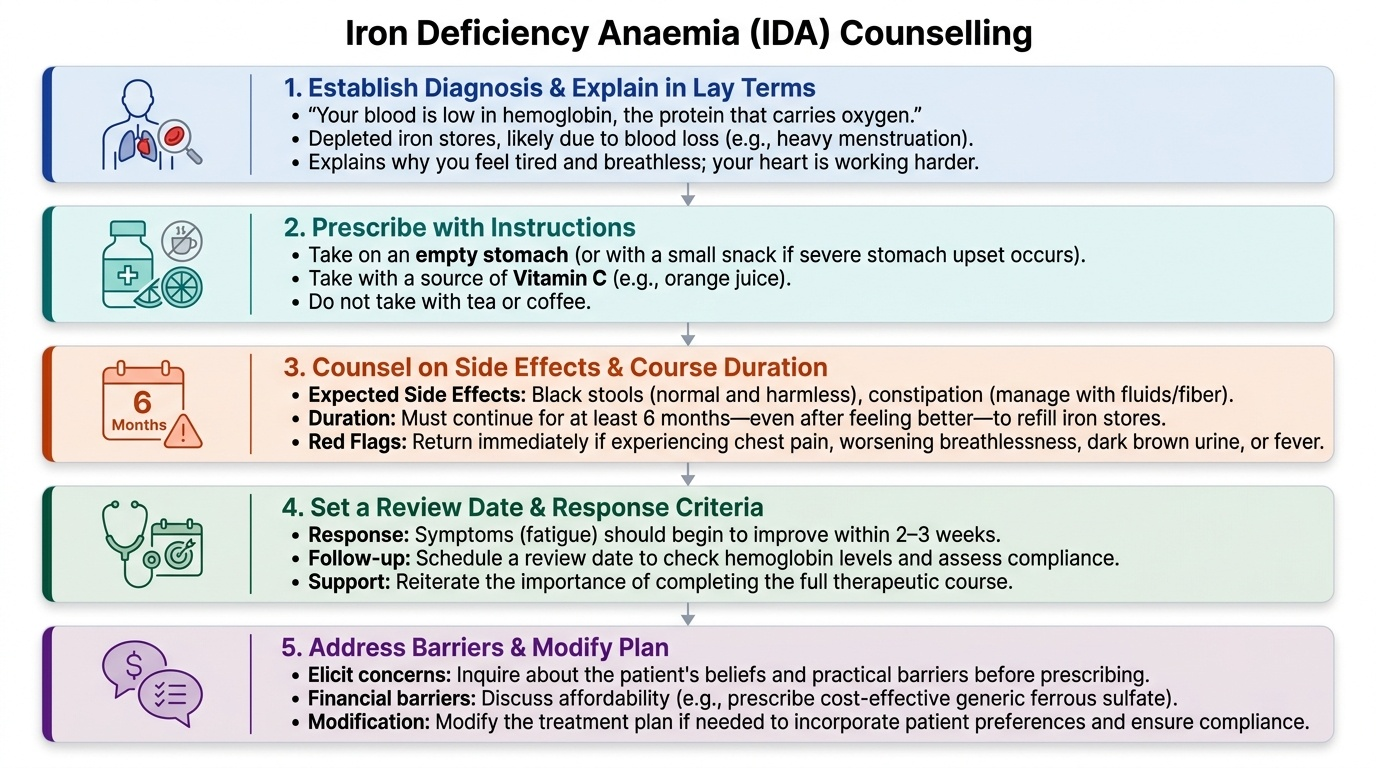
Communicating the diagnosis requires three components: (1) what is wrong (the diagnosis in lay terms), (2) what caused it (the aetiology, in plain language), and (3) what will happen if untreated versus treated (the clinical course and expected response). For IDA: "Your blood does not have enough haemoglobin — the protein that carries oxygen. This is because your iron stores have been depleted, most likely because of heavy menstrual bleeding over many months. This makes your heart work harder and explains why you feel so tired and breathless. The good news is that this is completely treatable with iron tablets, and most people start to feel better within 2–3 weeks. However, you will need to take the tablets for at least 6 months — even after you start feeling better — to refill your body's iron stores."
Counselling about iron therapy should cover: (1) how to take iron (timing relative to meals, with vitamin C, away from tea/coffee); (2) expected side effects (black stools — normal and harmless; constipation — manage with fluids and fibre; occasional nausea — take with a small snack if severe); (3) red flags that warrant return (worsening breathlessness, chest pain, dark brown urine, fever); (4) the importance of completing the full course even after symptoms improve; (5) dietary advice to prevent recurrence.
Incorporating patient preferences (IM9.13) involves eliciting the patient's concerns, beliefs, and practical barriers before prescribing. Common barriers in India: (1) cost — generic ferrous sulphate is available free at government health facilities and inexpensive at pharmacies; (2) work and social constraints — a daily morning tablet on an empty stomach may be impractical for a manual labourer who leaves for work before eating; in this case, a bedtime dose (which also improves tolerability) may be more realistic; (3) cultural beliefs — some patients believe that 'iron tablets cause the blood to become too thick' or that a particular diet can 'clean the blood'; these beliefs should be respectfully addressed; (4) previous adverse experience — a patient who stopped iron due to constipation in a prior pregnancy may benefit from a stool softener co-prescription and reassurance.
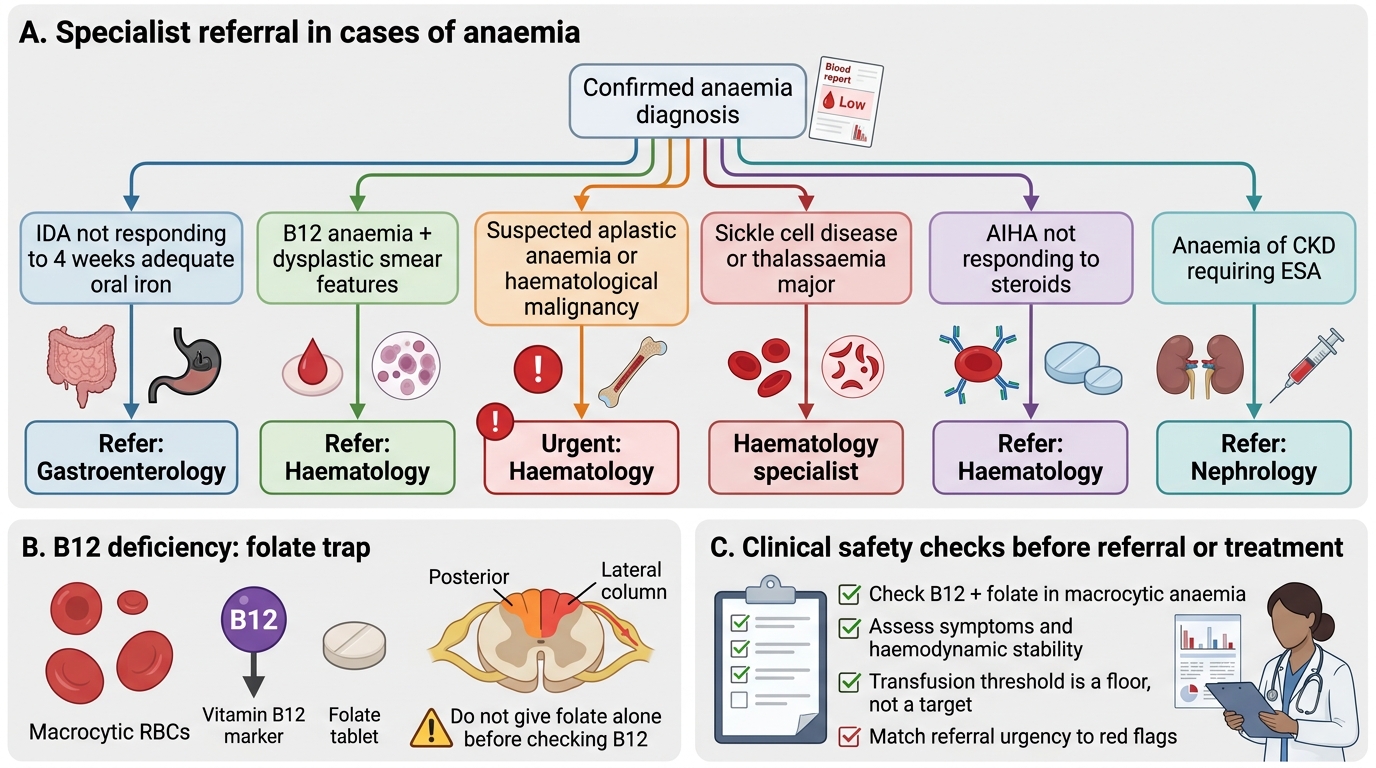
Specialist referral (IM9.17) is indicated when: (1) the cause of IDA is not identified after initial workup (consider haematology/gastroenterology referral for further investigation); (2) anaemia is refractory to replacement therapy (haematology referral to exclude a primary haematological disorder); (3) the haemoglobin fails to respond appropriately to B12 treatment (consider underlying haematological malignancy, especially if there is dysplastic morphology on smear); (4) aplastic anaemia or suspected haematological malignancy is identified (urgent haematology referral); (5) a patient with sickle cell disease or thalassaemia major requires specialised management (hydroxyurea, exchange transfusion, chelation therapy, or transplant consideration); (6) a patient with autoimmune haemolytic anaemia fails to respond to first-line steroids; (7) anaemia in the context of CKD requires nephrologist input for ESA dosing and iron status management.
Self-Assessment: Management Decisions in Anaemia
You have now covered the full spectrum of anaemia management — from cause-specific replacement therapy (iron, B12, folate) through national prevention programmes (AMB, WIFS, antenatal IFA) and blood transfusion practice (indications, component selection, pre-transfusion checks, adverse reaction recognition) to patient communication and specialist referral criteria. This self-assessment section presents clinical scenarios that test your ability to integrate these competencies into complete, contextually appropriate management decisions.
Scenario A: A 22-year-old strict vegetarian student presents with Hb 6.8 g/dL, MCV 109 fL, oval macrocytes and hypersegmented neutrophils on smear, serum B12 18 pg/mL (severely low), folate normal, and no neurological symptoms. She is haemodynamically stable with heart rate 96/min and BP 110/70. What is the complete management plan?
Analysis: This is severe megaloblastic anaemia from B12 deficiency (strict vegetarian diet). Haemodynamically stable — no indication for blood transfusion. Management: (1) IM hydroxocobalamin 1000 µg daily for 7 days (loading phase), then weekly for 4 weeks, then monthly for 3–6 months to replenish stores; dietary advice — add dairy products and eggs to the diet (lacto-ovo vegetarian provides adequate B12), or if remaining vegan, commit to lifelong oral cyanocobalamin supplementation; (2) Monitor for hypokalaemia during the first week of treatment (potassium shifts into proliferating erythroid cells — check electrolytes at day 3–5, supplement if needed); (3) Check iron stores — concurrent iron deficiency (common in women of reproductive age on vegetarian diets) will blunt the Hb response; add oral iron if ferritin is low; (4) Repeat Hb at 2 and 6 weeks to confirm response (expected Hb rise 1–2 g/dL per week once reticulocytosis peaks); (5) Counsel on dietary B12 sources and lifelong supplementation need if diet is unlikely to change. No transfusion is indicated — the anaemia is severe but chronic and compensated.
Scenario B: A 48-year-old woman with end-stage renal disease on haemodialysis three times weekly has Hb 8.1 g/dL, normocytic normochromic anaemia, ferritin 320 ng/mL, TSAT 18%, and EPO level undetectable. What is the management?
Analysis: Anaemia of CKD due to EPO deficiency. TSAT 18% is borderline — close to the threshold of iron-restricted erythropoiesis (<20% in CKD patients on ESA per KDIGO). Management: (1) Start erythropoiesis-stimulating agent (ESA) — epoetin alfa or darbepoetin alfa; target Hb 10–11.5 g/dL (KDIGO); avoid Hb >13 g/dL (associated with increased cardiovascular events and stroke in the CHOIR and TREAT trials); (2) IV iron (iron sucrose or ferric carboxymaltose) given intravenously during haemodialysis — oral iron is poorly absorbed in CKD and IV iron is standard of care in dialysis patients; target TSAT >20% and ferritin >200 ng/mL before and during ESA therapy; (3) Monitor Hb monthly; (4) Exclude other reversible causes of anaemia — B12 and folate deficiency, blood loss from HD circuit, hyperparathyroidism suppressing marrow (check PTH). Transfusion is not indicated in a stable CKD patient — transfusion in dialysis candidates causes alloimmunisation, which reduces the chance of successful renal transplant matching.
Scenario C: A 35-year-old woman with rheumatoid arthritis on hydroxychloroquine presents with Hb 9.8 g/dL, MCV 78 fL, ferritin 160 ng/mL, TSAT 13%, CRP 48 mg/L. She is asymptomatic from the anaemia at rest. Should she be transfused? Should she receive oral iron?
Analysis: Mild normocytic-to-microcytic anaemia in active rheumatoid arthritis — this is a mixed picture of ACD (ferritin elevated, TIBC likely low) with possible functional iron deficiency (TSAT 13% below the 16% threshold). She is asymptomatic — no indication for transfusion. Oral iron is unlikely to be fully effective in ACD because hepcidin blocks intestinal absorption. The correct approach: (1) Optimise disease control — if rheumatoid disease is poorly controlled, addressing the inflammatory driver is the most effective anaemia treatment; referral to rheumatology for treatment escalation; (2) Check soluble transferrin receptor to confirm functional iron deficiency component; if confirmed, a trial of IV iron (bypasses the hepcidin absorption block) is appropriate; (3) ESA can be considered if Hb falls below 10 g/dL and is attributable primarily to inadequate erythropoiesis rather than iron deficiency alone; (4) Review for other causes — NSAIDs causing occult GI blood loss (check stool occult blood).
Specialist Referral Pathways in Anaemia
CLINICAL PEARL
Two high-yield clinical pearls for anaemia management:
First, the folic acid trap in B12 deficiency: never prescribe folic acid alone to treat macrocytic anaemia without first confirming or excluding B12 deficiency. Folic acid will partially correct the blood count abnormalities of B12 deficiency — the patient feels better, the haemoglobin rises, and the clinician and patient believe the problem is solved — while B12-deficient metabolism continues to damage the posterior and lateral spinal cord columns (subacute combined degeneration of the cord, presenting as progressive sensory ataxia, loss of proprioception, Lhermitte's sign, and paraparesis). By the time the neurological deficit is noticed, it may be only partially reversible. The prevention is simple: always check B12 AND folate in macrocytic anaemia, treat both if both are deficient, and never start folate without knowing the B12 status.
Second, the transfusion threshold is a floor, not a target: the decision to transfuse should be driven by clinical symptoms and haemodynamic status, not by a haemoglobin number alone. A haemoglobin threshold of 7 g/dL for stable non-cardiac patients is a threshold below which transfusion is usually indicated — but the presence of symptoms, acute haemorrhage, or cardiovascular disease shift that threshold upward. Conversely, a patient with Hb 6.5 g/dL who is asymptomatic, haemodynamically stable, and whose cause of anaemia is being adequately treated should receive specific treatment, not blood.