Page 1 of 14
MI5.{1,3-4} | Anaerobic & Skin/Soft-Tissue Infections — SDL Guide
Learning Objectives
- Enumerate microbial agents causing anaerobic infections and describe their pathogenesis, clinical course, and laboratory diagnosis.
- Explain the etiopathogenesis, clinical course, and laboratory diagnosis of skin and soft tissue infections caused by bacterial, fungal, viral, and parasitic agents.
- Differentiate between infective and non-infective skin lesions and enumerate microbes causing systemic disease with skin involvement.
INSTRUCTIONS
Skin is the body's largest organ and first line of defence. Breaches in its integrity — from injections, trauma, surgery, diabetes, or insect bites — open the door to a wide spectrum of infections ranging from trivial impetigo to life-threatening necrotising fasciitis. In India, the burden is compounded by a tropical climate, high prevalence of diabetes, and endemic conditions like leprosy, scrub typhus, and sporotrichosis.
References
- Ananthanarayan & Paniker's Textbook of Microbiology, Ch 22, 23, 26 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old diabetic man presents to the emergency department with a swollen, erythematous left foot. The wound, which he noticed three days ago after stepping on a nail, now has a foul-smelling discharge with visible crepitus on palpation. His blood pressure is 90/60 mmHg and heart rate is 120 bpm. X-ray shows gas in the soft tissues. What organism is responsible? What is the single most important intervention in the next 30 minutes? And why will antibiotics alone not save this man's foot—or his life?
WHY THIS MATTERS
Skin and soft-tissue infections (SSTIs) span the infection spectrum from superficial (folliculitis, impetigo) to deep and life-threatening (necrotising fasciitis, myonecrosis). The clinical challenge is recognising the 'killer infections'—those requiring surgical debridement within hours, not days. Anaerobic organisms thrive in devitalised tissue and are the architects of gas gangrene, necrotising fasciitis, and tetanus. In India, the combination of diabetes, barefoot walking, and tropical wounds makes this knowledge life-saving.
RECALL
Recall from earlier modules:
- Properties of anaerobes: sensitivity to oxygen, growth below redox potential, relationship to pus without leucocyte response.
- Basic structure of skin: epidermis, dermis, subcutaneous tissue, fascia — each level corresponds to a specific infection type.
- Gram stain interpretation: Gram-positive vs. Gram-negative rods and cocci.
- Concept of synergistic infection: two or more organisms working together to cause greater tissue damage.
Anaerobic Infections — Overview and Classification
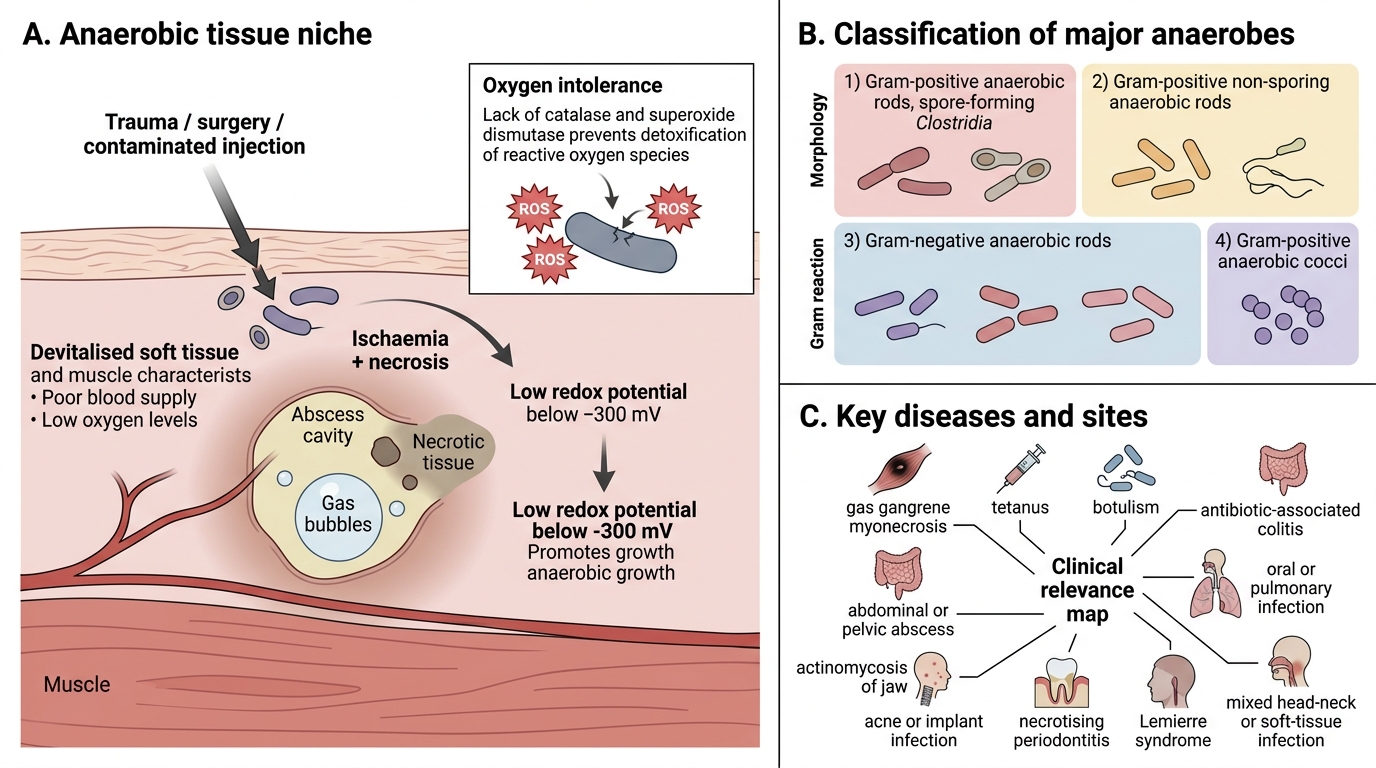
Anaerobic Infections: Niche, Classification, and Clinical Associations
Anaerobes are organisms that cannot tolerate oxygen due to lack of catalase and/or superoxide dismutase; they thrive in devitalised tissue, ischaemic wounds, and abscesses where redox potential falls below –300 mV.
Major anaerobic pathogens:
Gram-positive anaerobic rods (Clostridia — spore-forming):
- Clostridium perfringens — gas gangrene (myonecrosis), food poisoning, post-partum sepsis
- Clostridium tetani — tetanus
- Clostridium botulinum — botulism
- Clostridium difficile — antibiotic-associated colitis (CDAD)
Gram-positive non-sporing anaerobic rods:
- Actinomyces israelii — actinomycosis (jaw, abdomen, pelvis)
- Propionibacterium acnes — acne, post-implant infections
Gram-negative anaerobic rods:
- Bacteroides fragilis — most common anaerobe in clinical specimens; abdominal/pelvic abscesses; capsule resists phagocytosis
- Fusobacterium nucleatum — necrotising periodontitis, Lemierre syndrome
- Prevotella spp. — oral, pulmonary infections
Gram-positive anaerobic cocci:
- Peptostreptococcus spp. — mixed anaerobic infections of soft tissue, head and neck
Gas Gangrene (Clostridial Myonecrosis)
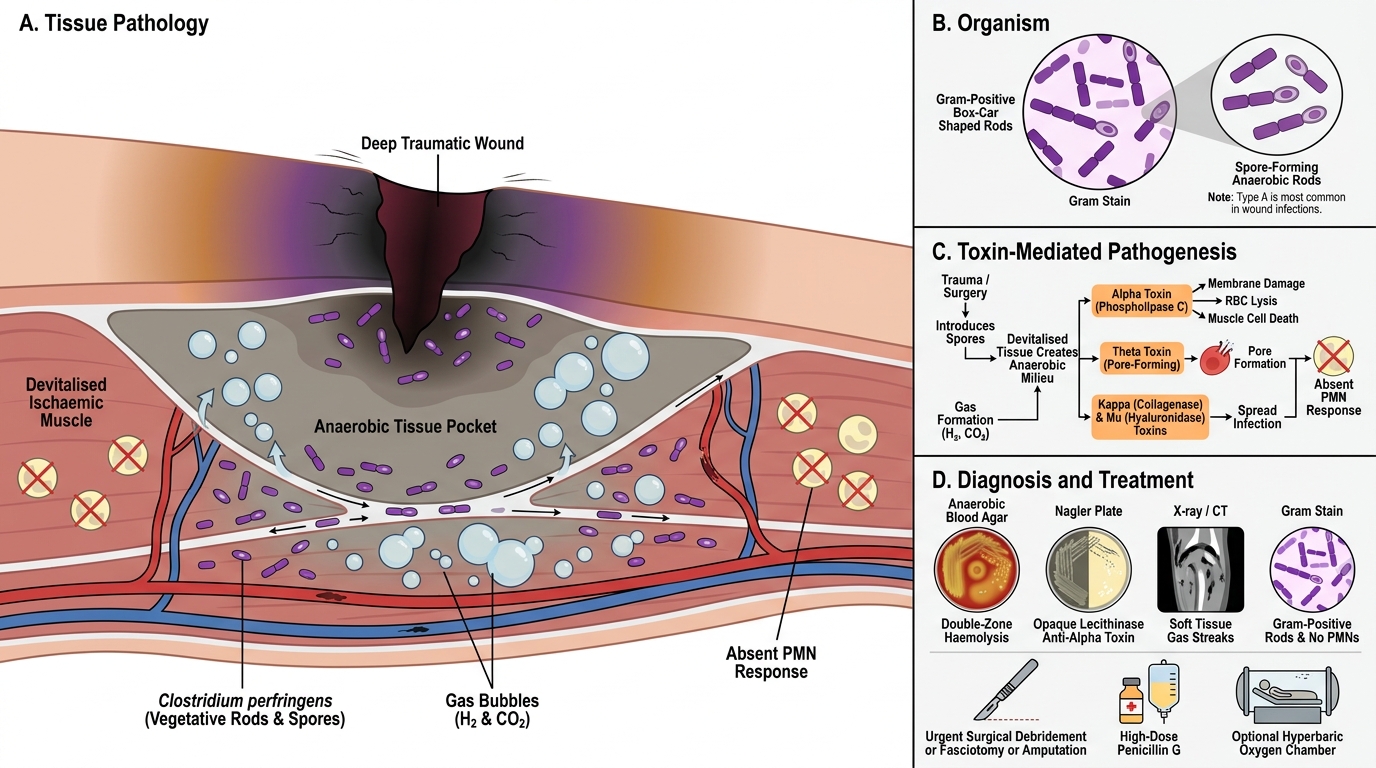
Gas Gangrene: Clostridial Myonecrosis
Clostridium perfringens (type A is most common in wound infections) is a large, Gram-positive, spore-forming, anaerobic rod with a characteristic box-car appearance on Gram stain.
Pathogenesis:
1. Spores introduced into tissue by trauma, surgery, contaminated injection
2. Devitalised, ischaemic tissue provides the anaerobic milieu
3. Vegetative forms produce alpha toxin (lecithinase, phospholipase C) — destroys cell membranes, lyses RBCs, kills muscle cells
4. Other toxins: theta toxin (perfringolysin O — pore-forming); kappa toxin (collagenase); mu toxin (hyaluronidase)
5. Rapid tissue destruction → gas (H₂ + CO₂) in tissue planes → crepitus
6. No leucocyte infiltration in histology — toxins kill PMNs before they can respond
Clinical features: Sudden severe pain at wound site → local oedema → skin discolouration (bronze to black) → crepitus (gas) → sweet-smelling (rancid butter) discharge → systemic toxaemia (fever, tachycardia, haemolysis, renal failure, shock)
Diagnosis:
- Gram stain of wound discharge: Gram-positive rods, no PMNs (key finding)
- Culture: anaerobic blood agar (double-zone haemolysis — inner clear zone [theta toxin] + outer partial zone [alpha toxin])
- Nagler plate: lecithinase activity — opaque zone around colonies inhibited by anti-alpha toxin
- X-ray/CT: gas in soft tissues
Treatment: Surgical debridement (fasciotomy/amputation) + high-dose penicillin G ± hyperbaric oxygen

Nagler Reaction for Clostridium perfringens
CLINICAL PEARL
Absent PMNs + gas = Clostridium: The pathognomonic Gram stain finding in gas gangrene is Gram-positive rods in the ABSENCE of polymorphonuclear leucocytes. Alpha toxin kills leucocytes as fast as they arrive. This is the opposite of most infections where PMNs are abundant. If you see pus (PMNs) with gas, think mixed infection (type I necrotising fasciitis) rather than pure clostridial gas gangrene.
Tetanus — Clostridium tetani
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
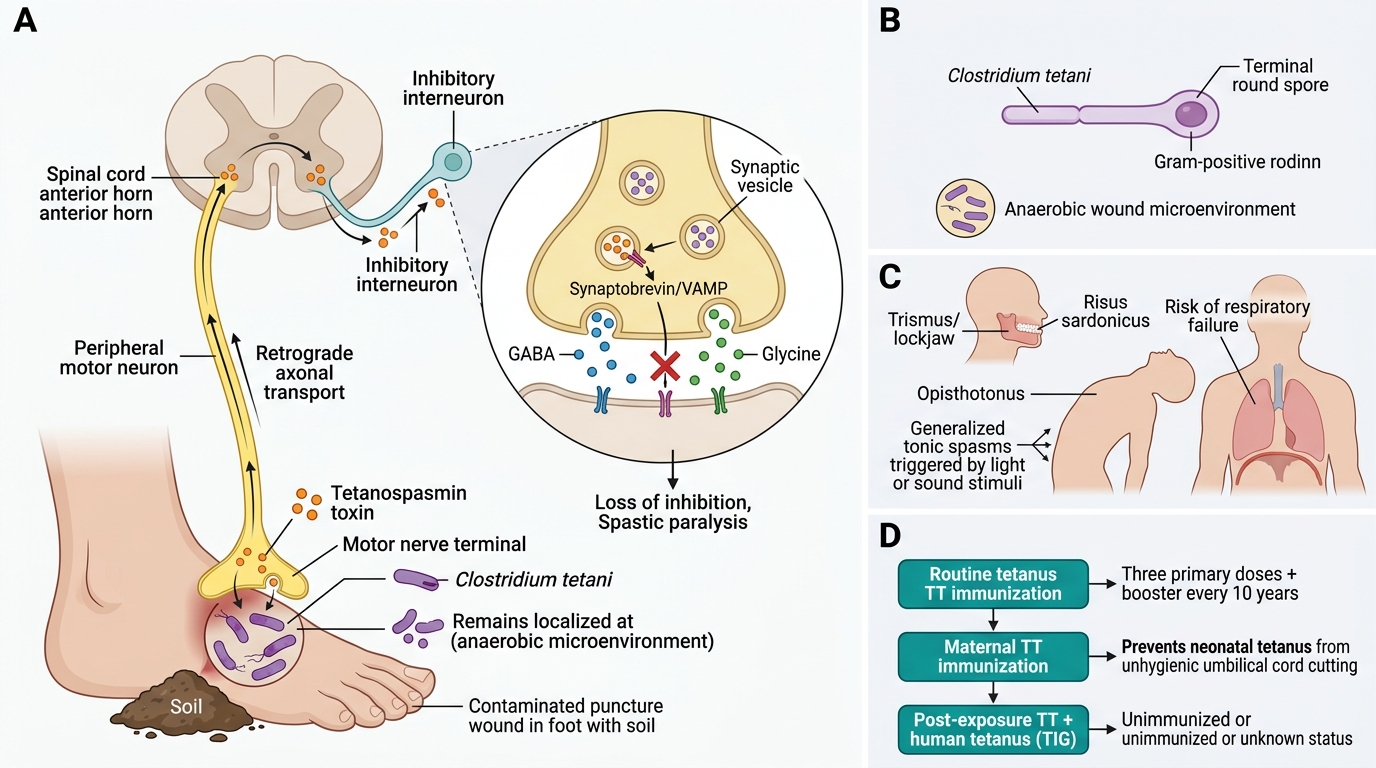
Tetanus: Clostridium tetani Pathogenesis and Prevention
Clostridium tetani is a slender Gram-positive rod with a terminal spore (drum-stick appearance). It is an obligate anaerobe, non-invasive — it stays at the wound site but its toxin travels systemically.
Toxin — Tetanospasmin (TeNT):
- Zinc-dependent metalloprotease
- Travels retrograde along motor neurones to anterior horn cells
- Cleaves synaptobrevin (VAMP) → blocks release of inhibitory neurotransmitters (GABA and glycine)
- Loss of inhibitory tone → spastic paralysis + autonomic instability
Clinical features: Trismus (lockjaw), risus sardonicus (fixed grin), opisthotonus (arching of back), generalised tonic spasms triggered by stimuli, respiratory failure
Diagnosis: Primarily clinical; wound culture rarely positive; mouse neutralisation test for toxin (reference only)
Prevention (key for India):
- Tetanus toxoid (TT): 3 primary doses (universal childhood immunization) + booster every 10 years
- Neonatal tetanus (Clostridium tetani via unhygienic cord cutting): prevented by maternal TT immunization during pregnancy
- Post-exposure: TT + Human tetanus immunoglobulin (TIG) for unimmunized/unknown status