Page 2 of 14
MI5.{1,3-4} | Anaerobic & Skin/Soft-Tissue Infections — SDL Guide (Part 2)
Skin and Soft-Tissue Infections — Bacterial
Bacterial Skin and Soft-Tissue Infections by Tissue Depth
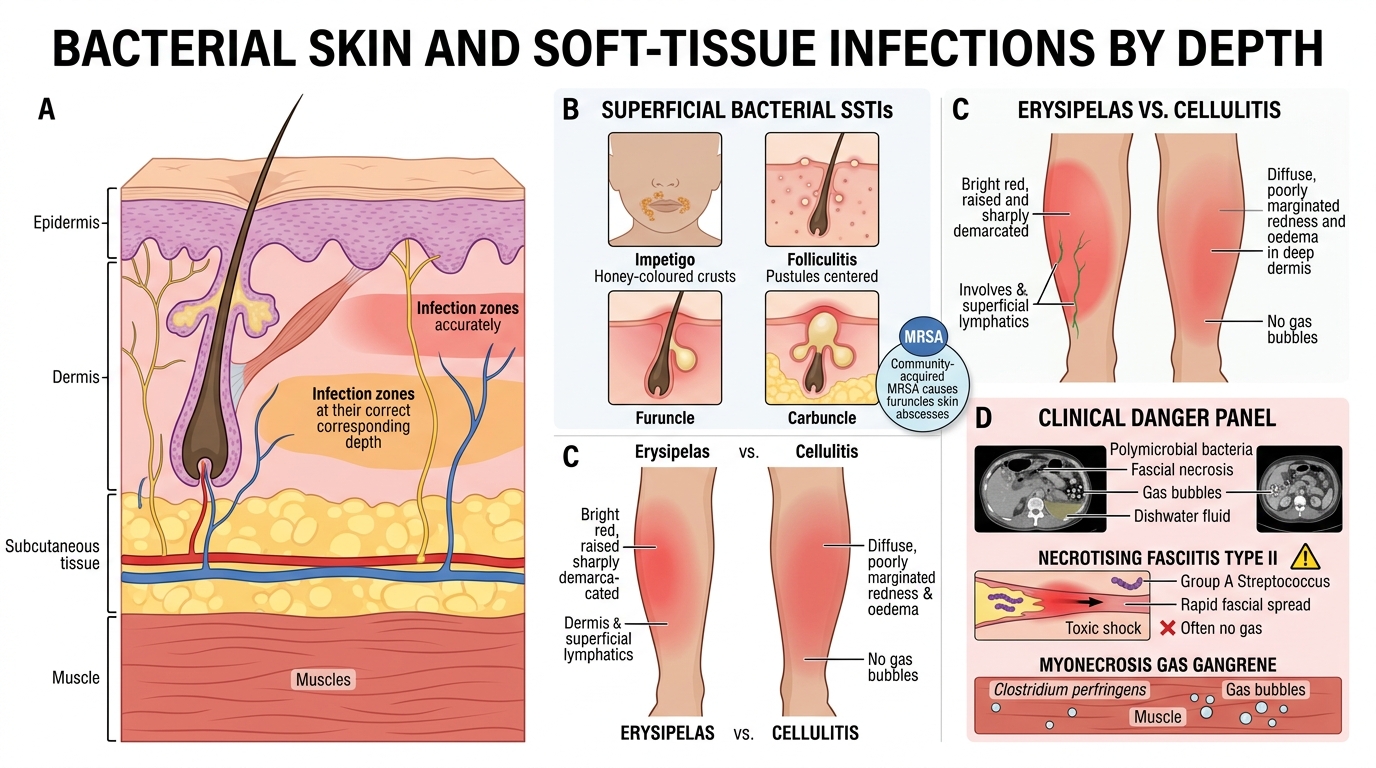
Bacterial SSTIs classified by depth of tissue involved:
Superficial (epidermis/dermis):
- Impetigo: S. aureus (bullous — exfoliatin toxin) or S. pyogenes (crusted); honey-coloured crusts on face in children; non-scarring; treat with topical mupirocin or oral penicillin
- Folliculitis: S. aureus in hair follicles; superficial pustules; sycosis barbae in beard area
- Furuncle / Carbuncle: deeper S. aureus infection; carbuncle = multiple follicles + subcutaneous extension; risk of bacteraemia in diabetics
- Erysipelas: S. pyogenes (Group A Strep); sharply demarcated, raised, bright-red plaque; involves upper dermis + superficial lymphatics; face/leg; treat with penicillin
- Cellulitis: S. aureus or S. pyogenes; involves deeper dermis and subcutaneous tissue; diffuse, poorly marginated redness + oedema; no gas; treat with IV nafcillin or cloxacillin
Deep / Fascia / Muscle:
- Necrotising fasciitis type I: Polymicrobial (anaerobes + facultatives); diabetes, peripheral vascular disease predispose; rapidly spreading necrosis; gas on CT; "dishwater" fluid from wound; requires emergency surgical debridement
- Necrotising fasciitis type II: Mono-microbial — Group A Strep (S. pyogenes); "flesh-eating bacteria"; toxic shock syndrome toxin; extremely rapid; often no gas
- Myonecrosis (gas gangrene): C. perfringens — as above
MRSA (Methicillin-Resistant S. aureus):
- Community-acquired CA-MRSA causes furuncles, skin abscesses; treat with trimethoprim-sulfamethoxazole, doxycycline, or vancomycin
- Hospital-acquired HA-MRSA: surgical wound infections, IV line infections
SELF-CHECK
A young boy has multiple honey-coloured crusted lesions around the nose and mouth after a minor abrasion. No fever, no deep tissue involvement. Gram stain of the crust shows Gram-positive cocci in chains. What is the most likely diagnosis and its causative organism?
A. Bullous impetigo caused by Staphylococcus aureus (exfoliatin toxin)
B. Non-bullous impetigo caused by Streptococcus pyogenes
C. Erysipelas caused by Streptococcus pyogenes
D. Folliculitis caused by Staphylococcus aureus
Reveal Answer
Answer: B. Non-bullous impetigo caused by Streptococcus pyogenes
Honey-coloured crusted lesions on the face in a child after minor trauma is the classic presentation of non-bullous impetigo caused by Streptococcus pyogenes (Group A Strep) or sometimes S. aureus. Gram-positive cocci in chains point to Streptococcus. Bullous impetigo (option A) is caused by S. aureus exfoliatin toxin and presents with intact flaccid bullae, not crusts. Erysipelas (option C) involves the dermis with a sharply raised border, not surface crusts.
Fungal, Viral, and Parasitic Skin Infections
Fungal and Viral Skin Infections: Clinical and Diagnostic Features
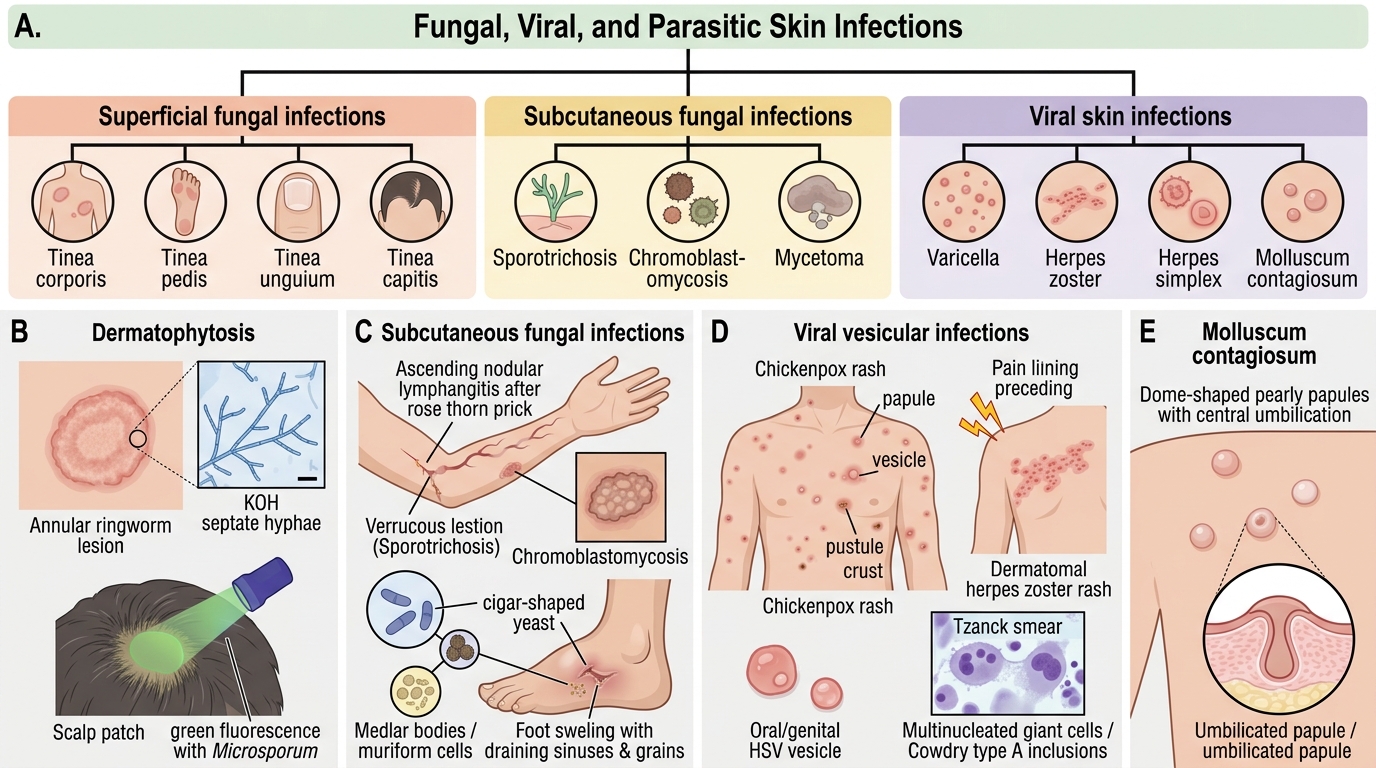
Dermatophytoses (Superficial fungal infections):
- Trichophyton, Microsporum, Epidermophyton spp.; affect keratinised layers (stratum corneum, hair, nails)
- Tinea corporis (ringworm body), tinea pedis (athlete's foot), tinea unguium (onychomycosis), tinea capitis (scalp ringworm)
- Diagnosis: KOH preparation — branching, septate hyphae; Wood's lamp (green fluorescence with Microsporum); culture on Sabouraud Dextrose Agar (SDA)
Subcutaneous fungal infections:
- Sporotrichosis (Sporothrix schenckii) — rose thorn prick → nodular lymphangitis (ascending nodules along lymphatics on arm); KOH — 'cigar-shaped' yeast; treat with itraconazole
- Chromoblastomycosis (Fonsecaea spp.) — verrucous skin lesions; tissue shows Medlar bodies (muriform cells) — brown, thick-walled, sclerotic cells
- Mycetoma — Madura foot; can be actinomycetoma (Nocardia, Actinomyces) or eumycetoma (Madurella); grains (granules) in discharge
Viral skin infections:
- Varicella (Chickenpox): VZV; centripetal distribution; successive crops; papule → vesicle → pustule → crust; Tzanck smear: multinucleated giant cells (Cowdry type A inclusions)
- Herpes Zoster: VZV reactivation; dermatomal; severe pain precedes rash
- Herpes simplex (HSV 1/2): oral/genital vesicles; Tzanck smear positive; PCR for definitive diagnosis
- Molluscum contagiosum: Poxvirus; dome-shaped papules with central umbilication; Henderson-Patterson (molluscum) bodies on HE stain
- Measles (Rubeola): Koplik spots (pathognomonic buccal mucosa) → maculopapular rash; systemic
Parasitic skin infections:
- Scabies: Sarcoptes scabiei mite; burrows in finger webs, wrists; intense night itch; skin scraping + microscopy = mite/eggs/scybala
- Cutaneous larva migrans: Ancylostoma braziliense hookworm larvae — serpiginous tracks in skin; barefoot walking on contaminated sand/soil
Infective vs. Non-Infective Skin Lesions (MI5.4)
Infective vs. Non-Infective Skin Lesions
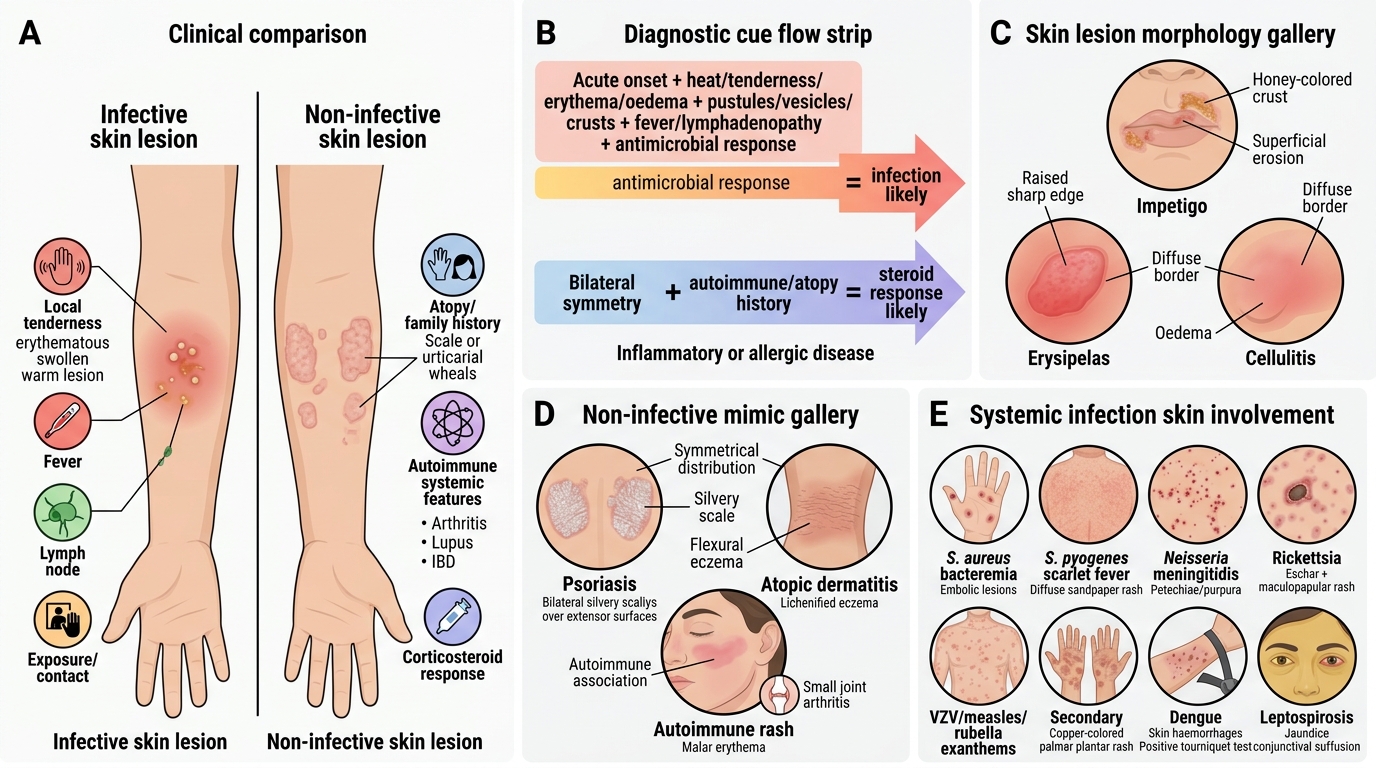
Differentiating infective from non-infective skin disease is a key clinical skill:
Features suggesting infection:
- Acute onset
- Localised heat, tenderness, erythema, oedema
- Pustules, vesicles, crusts
- Fever, lymphadenopathy
- Response to antimicrobials
- Identified contact/exposure history (epidemiological link)
Features suggesting non-infective aetiology (inflammatory/allergic/autoimmune):
- Bilateral, symmetrical distribution
- Associated with systemic features of autoimmune disease (arthritis, lupus, IBD)
- Response to corticosteroids
- Personal/family history of atopy, psoriasis
Systemic infections with prominent skin involvement (microbes causing systemic disease + skin):
- S. aureus — bacteraemia → embolic skin lesions, Janeway lesions (infective endocarditis)
- S. pyogenes — scarlet fever (erythrogenic toxin → diffuse sandpaper rash)
- Neisseria meningitidis — purpuric/petechial rash (meningococcaemia)
- Rickettsia spp. — eschar + maculopapular rash (scrub typhus, Rocky Mountain spotted fever)
- VZV, measles, rubella — exanthems
- Secondary syphilis (T. pallidum) — copper-coloured palmar/plantar rash
- Dengue — skin haemorrhages, positive tourniquet test
- Leptospirosis — jaundice + conjunctival suffusion

Skin Lesion Morphology in Common Infections
SELF-CHECK
A patient develops ascending nodular skin lesions on the dorsum of his right hand and forearm following a thorn prick while gardening. The lesions are non-tender and painless. KOH preparation of material from a nodule shows cigar-shaped yeast forms. What is the diagnosis?
A. Chromoblastomycosis caused by Fonsecaea pedrosoi
B. Sporotrichosis caused by Sporothrix schenckii
C. Mycetoma caused by Madurella mycetomatis
D. Cutaneous larva migrans caused by Ancylostoma braziliense
Reveal Answer
Answer: B. Sporotrichosis caused by Sporothrix schenckii
The classic triad for sporotrichosis: (1) trauma with a thorn or plant material, (2) ascending nodular lymphangitis along the arm, (3) cigar-shaped or fusiform yeast on KOH/culture. Sporothrix schenckii is a dimorphic fungus — mould in soil/environment, cigar-shaped yeast at 37°C in tissue. Treatment: itraconazole for 3–6 months. Chromoblastomycosis shows Medlar bodies (muriform cells) in tissue. Mycetoma forms triad of swelling + sinuses + grains.
CLINICAL PEARL
Necrotising fasciitis — the 'dishwater' clue: The intraoperative finding of non-purulent, thin, grey-brown 'dishwater' fluid emerging from fascial planes, with absence of frank pus and easy blunt dissection through necrotic fascia, confirms necrotising fasciitis. This is a surgical emergency — every hour of delay worsens mortality. The clinical triad: pain out of proportion to skin findings + skin necrosis + systemic toxicity = NF until proven otherwise.