Page 7 of 14
OG1.4-5 | Caesarean Audit and National OG Programs — SDL Guide (Part 2)
Janani Suraksha Yojana (JSY) and Janani Shishu Suraksha Karyakram (JSSK)
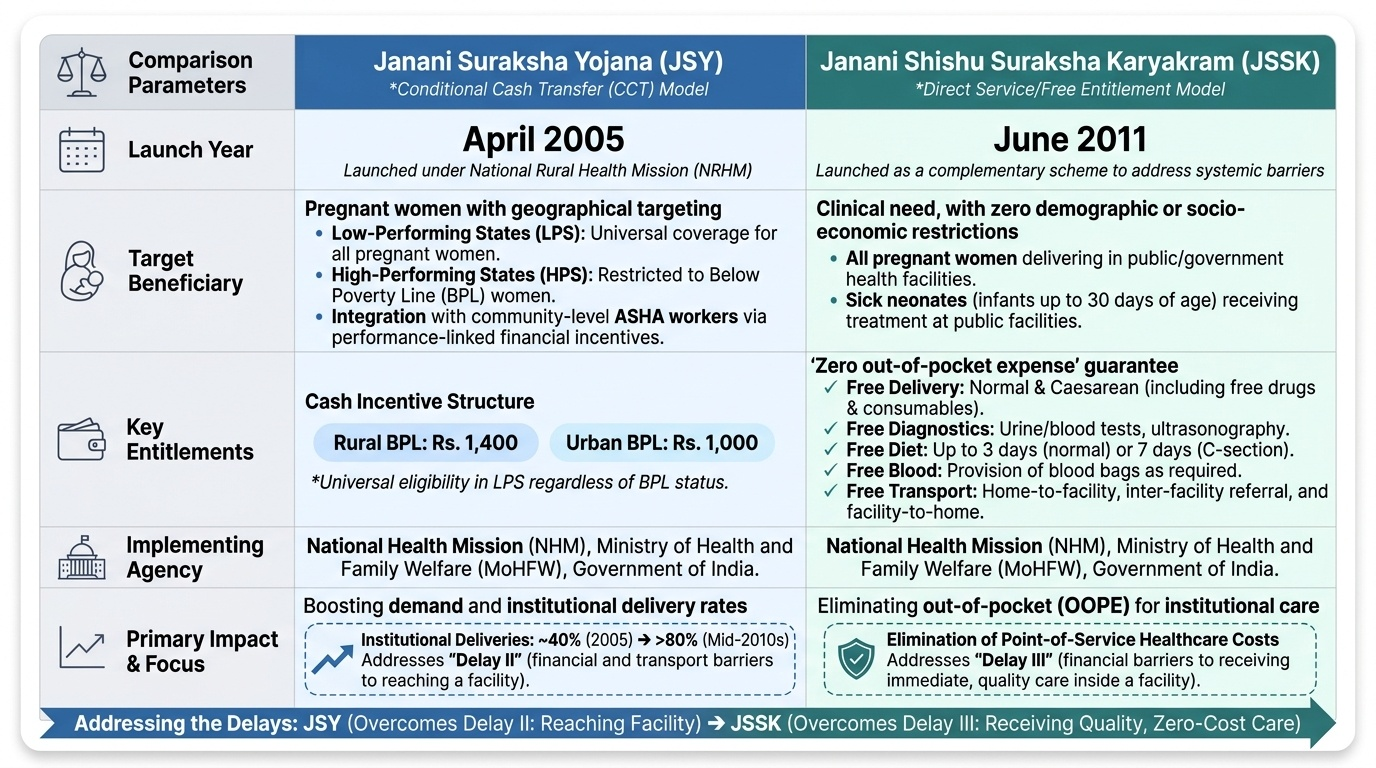
Janani Suraksha Yojana (JSY) was launched in April 2005 as a component of the National Rural Health Mission (NRHM), now part of the National Health Mission (NHM). It is a conditional cash transfer scheme that provides a direct cash incentive to pregnant women who deliver in a government health facility or accredited private institution, with the goal of increasing institutional delivery rates and thereby reducing maternal and neonatal mortality. JSY targets below-poverty-line (BPL) women and is applicable universally in low-performing states (LPS: eight Empowered Action Group states — UP, Uttarakhand, Bihar, Jharkhand, MP, Chhattisgarh, Assam, Rajasthan — and J&K, Orissa), with BPL restriction in high-performing states (HPS).
The cash entitlement structure under JSY is: Rs 1,400 for rural BPL women and Rs 1,000 for urban BPL women in HPS; in LPS, the benefit is universal regardless of BPL status. The ASHA (Accredited Social Health Activist) receives a performance-linked incentive for facilitating institutional delivery, which creates a community-level mobilisation mechanism. Evaluations have credited JSY with a substantial proportion of India's increase in institutional delivery rates from approximately 40% (pre-JSY, 2005) to over 80% by the mid-2010s.
Janani Shishu Suraksha Karyakram (JSSK) was launched in June 2011 as a complementary scheme that moves beyond the cash transfer model to provide free entitlements — eliminating out-of-pocket costs for pregnant women and sick neonates in government health facilities. The key JSSK entitlements are:
• Free and zero-expense delivery (normal and caesarean), including free drugs and consumables.
• Free diagnostics: blood tests, urine tests, ultrasonography.
• Free diet during stay (up to 3 days for normal delivery, 7 days for CS).
• Free provision of blood as required.
• Free transport from home to facility and back, and between facilities on referral.
• Exemption from all user charges.
For sick neonates (up to 30 days of age), JSSK provides: free treatment at government facilities, free diagnostics, free drugs and consumables, free provision of blood, and free transport. The combined JSY–JSSK framework addresses Delay II (financial and transport barriers to reaching a facility) and part of Delay III (out-of-pocket cost barriers to receiving care once at the facility).
Provided image
SELF-CHECK
A woman from a BPL family in rural Uttar Pradesh (a low-performing state) delivers at a government PHC. Under JSY, which statement is correct?
A. She receives Rs 1,000 cash incentive as UP is a low-performing state
B. She is not eligible because JSY is only for high-performing states
C. She receives the cash incentive universally in LPS regardless of BPL card status
D. She must have completed all 4 ANC visits to receive the JSY benefit
Reveal Answer
Answer: C. She receives the cash incentive universally in LPS regardless of BPL card status
In Low-Performing States (LPS), including UP, the JSY cash incentive is available universally to all pregnant women who deliver institutionally, regardless of BPL card status. The cash amount for rural delivery in LPS is Rs 1,400 (for rural areas). BPL restriction applies only in High-Performing States.
Birth and Death Registration: RBD Act and Civil Registration System
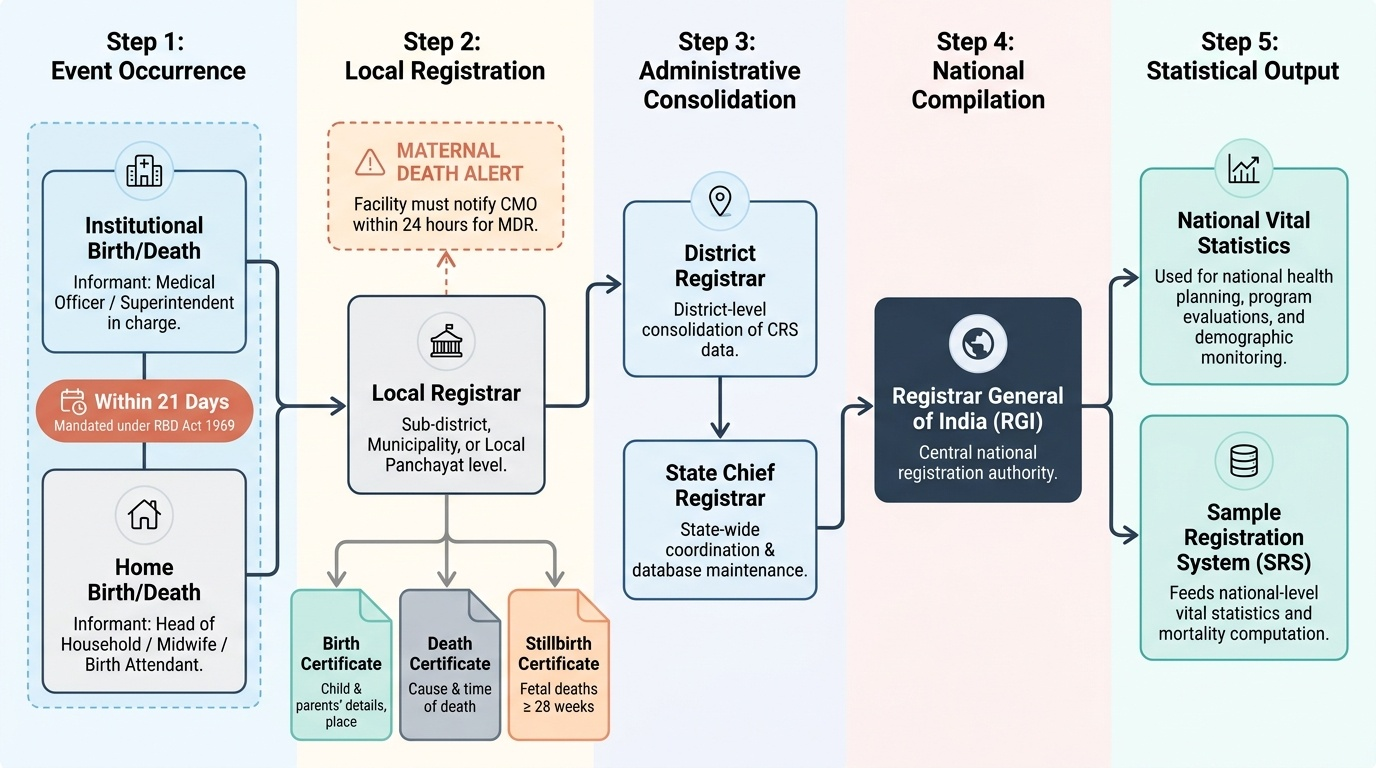
The Registration of Births and Deaths (RBD) Act 1969 is the central legislation mandating the registration of every birth and death in India. The Act establishes the Civil Registration System (CRS), operated through a network of registrars — the Chief Registrar at the national level (the Registrar General of India), State Registrars, and local registrars at district and sub-district levels. The CRS is the primary system for generating legal proof of birth (birth certificate) and death (death certificate), and it feeds data into the Sample Registration System (SRS) for vital statistics computation. Understanding the CRS is essential for the clinical practitioner because the RBD Act places specific, time-bound obligations on the medical officer in charge of any institution where a birth or death occurs — obligations that are legally enforceable and that also provide the data foundation for all national vital statistics, maternal death reviews, and programme evaluations.
For obstetric practice, the key registration obligations are:
• Birth registration: Every birth must be reported to the local registrar within 21 days (in most states; some state-specific rules apply). In government hospitals, the medical officer or superintendant is the designated informant for institutional births. For home births, the head of household or midwife is the informant. The birth certificate records: child's name, date, time and place of birth, parents' names and details, and the attending birth attendant.
• Death registration: Every death — including stillbirths at ≥28 weeks — must be registered. For maternal deaths, registration triggers the Maternal Death Review (MDR) notification obligation: the facility must notify the Chief Medical Officer (CMO) within 24 hours.
• Still birth registration: In many states, stillbirths (fetal deaths at ≥28 weeks) are separately notifiable and registered; a stillbirth certificate is issued. This is distinct from a live birth certificate and a death certificate.
Under-registration of births and deaths — particularly in rural areas and among marginalised communities — remains a public health challenge in India, contributing to gaps in vital statistics. Improving the completeness of CRS data is a priority under the National Health Mission, with facility-based birth and death reporting now linked to the HMIS digital platform. As a clinician in a government facility, timely and accurate completion of birth and death notification forms is a legal obligation under the RBD Act — non-compliance is a punishable offence under the Act.
Provided image
Anaemia Mukt Bharat and SUMAN
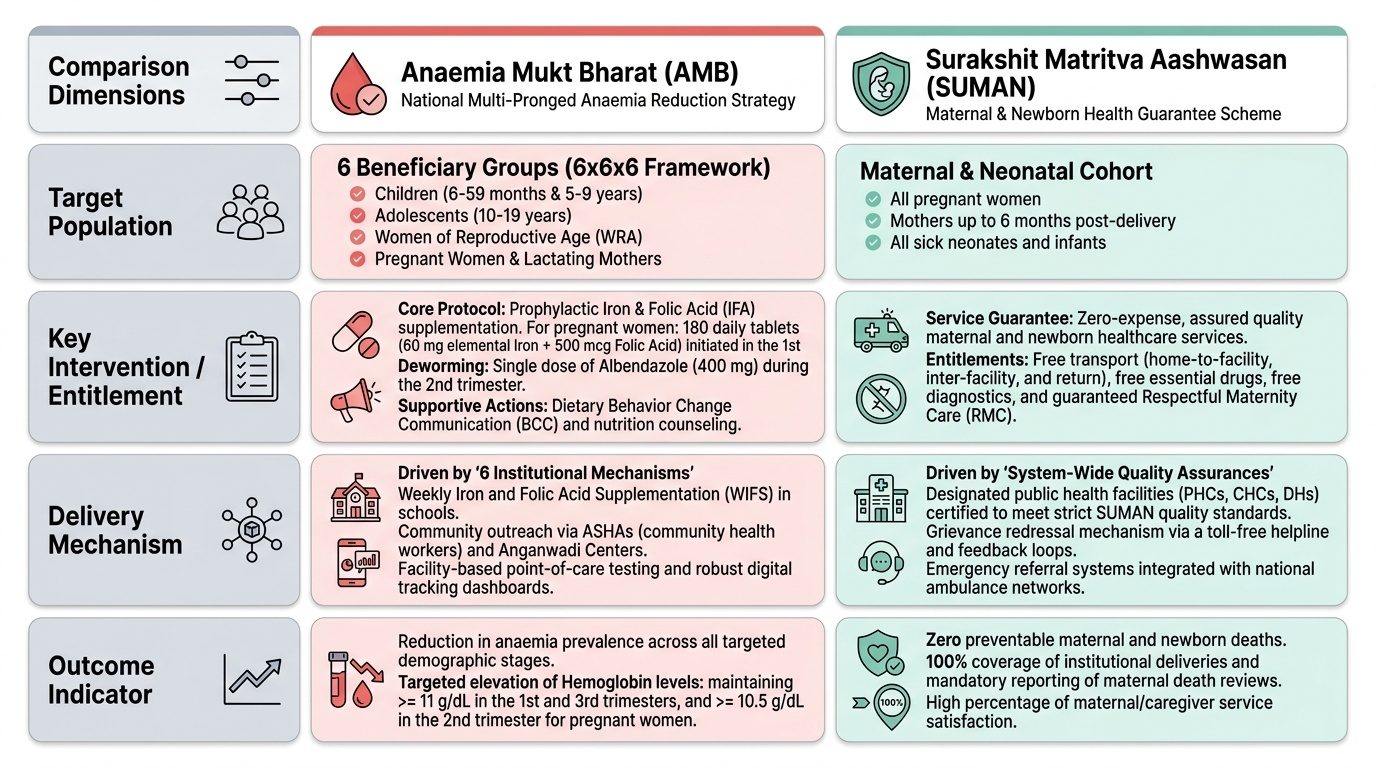
Anaemia Mukt Bharat (AMB) — launched in 2018 under the NHM — is a national multi-pronged strategy targeting anaemia reduction across the life course, with particular focus on women of reproductive age, pregnant and lactating women, adolescent girls, and children. Anaemia in pregnancy (haemoglobin <11 g/dL in the first and third trimesters, <10.5 g/dL in the second trimester) is a major indirect cause of maternal death — it aggravates the consequences of postpartum haemorrhage, reduces cardiac reserve, impairs immune function, and increases the risk of preterm labour and low birthweight.
The AMB strategy targets anaemia prevalence through six key interventions, organised as the '6×6×6' framework: six target beneficiary groups (children 6–59 months, 5–9 years, 10–19 years/adolescents, women of reproductive age, pregnant women, lactating mothers) × six interventions (prophylactic iron and folic acid supplementation, deworming, behaviour change communication on diet, use of IFA testing and testing platforms at facilities, treatment protocols, and nutrition counselling) × six institutional mechanisms (testing at health facilities, supply chain for IFA, community volunteers, school health, WIFS — Weekly Iron and Folic Acid Supplementation for adolescents, and digital tracking). For pregnant women, the specific AMB protocol is 180 daily IFA tablets (60 mg elemental iron + 500 µg folic acid) beginning as early as possible in the first trimester, with deworming (albendazole 400 mg, single dose, second trimester).
SUMAN (Surakshit Matritva Aashwasan) was launched in October 2019 as a minimum standard guarantee scheme ensuring that every pregnant woman and sick newborn accessing a government health facility receives assured, dignified, and respectful care — free of cost and with no denial. The core SUMAN commitments are organised as 'what every woman is entitled to receive':
• At least 4 ANC visits (1 in the first trimester, 1 in the second, 2 in the third), with a minimum set of investigations at each visit.
• Skilled birth attendance at every delivery, with availability of emergency obstetric care (EmOC).
• Postnatal care for at least 48 hours after institutional delivery.
• Free access to safe blood transfusion, caesarean section, and any other obstetric procedure required.
• Respectful maternity care — freedom from verbal or physical abuse, discrimination, or coercion; the right to privacy and confidentiality; and informed consent for all procedures.
SUMAN builds on JSSK's free-services framework by adding a quality and rights dimension — making care not just free but guaranteed to meet minimum standards. Under SUMAN, facilities must display a 'SUMAN charter' visibly listing all entitlements.
Provided image
SELF-CHECK
Which of the following BEST describes the key difference between JSY and JSSK?
A. JSY provides cash to the ASHA; JSSK provides cash to the mother
B. JSY is a cash transfer incentive for institutional delivery; JSSK provides free services and eliminates out-of-pocket costs at government facilities
C. JSY is for BPL women only; JSSK is for all women regardless of economic status
D. JSY covers antenatal care costs; JSSK covers only delivery costs
Reveal Answer
Answer: B. JSY is a cash transfer incentive for institutional delivery; JSSK provides free services and eliminates out-of-pocket costs at government facilities
The fundamental distinction is: JSY is a conditional cash transfer (money given to the woman/ASHA after institutional delivery), while JSSK is a free-services guarantee (eliminating the need to pay for drugs, diagnostics, blood, diet, and transport at the facility). Both operate in public facilities, but JSSK extends to all women who deliver there, not just BPL. JSY covers some antenatal and postnatal visits, not just delivery.