Page 8 of 14
OG1.4-5 | Caesarean Audit and National OG Programs — SDL Guide (Part 3)
Mechanisms: How Audit and Programmes Reduce Maternal and Perinatal Mortality
The causal pathways through which these audit and programme tools reduce maternal and perinatal mortality are specific and should be understood mechanistically — not as a list to memorise, but as a logical framework that helps you predict when each tool will and will not work.
Robson CS audit operates through the clinical governance cycle: audit identifies the group(s) with unexpectedly high CS rates → root cause analysis reveals the practice factors (e.g., low VBAC acceptance, early intervention in latent phase, defensive CS for fear of litigation) → targeted clinical protocols or training address those factors → re-audit documents improvement or persistent gaps. The mechanism is a feedback loop operating at Delay III (quality of care at the facility). It does not address Delays I or II. Its limitation is that it requires accurate, complete data and a facility culture willing to change practice in response to findings — audit without action is data collection, not quality improvement.
JSY and JSSK address primarily Delays II and III. JSY's cash transfer incentivises the decision to deliver institutionally (a Delay I component — changing the cost-benefit calculation for seeking care) and removes a financial barrier to reaching the facility (Delay II). JSSK eliminates the out-of-pocket cost component of Delay III — a woman who arrives at a facility should no longer face the barrier of being unable to afford drugs, blood, or surgery. The limitation is implementation fidelity: in poorly resourced facilities, drugs and blood may not be available even when they are nominally free, leaving Delay III operative despite JSSK.
Anaemia Mukt Bharat addresses an indirect determinant: anaemia increases the severity of haemorrhagic complications (the leading direct cause of maternal death). By improving baseline haemoglobin before delivery, AMB reduces the case-fatality rate of PPH — a woman with Hb 9 g/dL haemorrhaging 800 mL is at far greater risk than one with Hb 12 g/dL. The mechanism is nutritional preparation of the reproductive-age and pregnant woman population, operating upstream of any individual delivery.
SUMAN addresses quality and rights at Delay III — by mandating minimum standards of care and respectful treatment, it creates a rights framework that should prevent refusal of care, denial of emergency services, and mistreatment, all of which deter women from seeking or remaining in institutional care (Delay I and Delay III feedback loop).
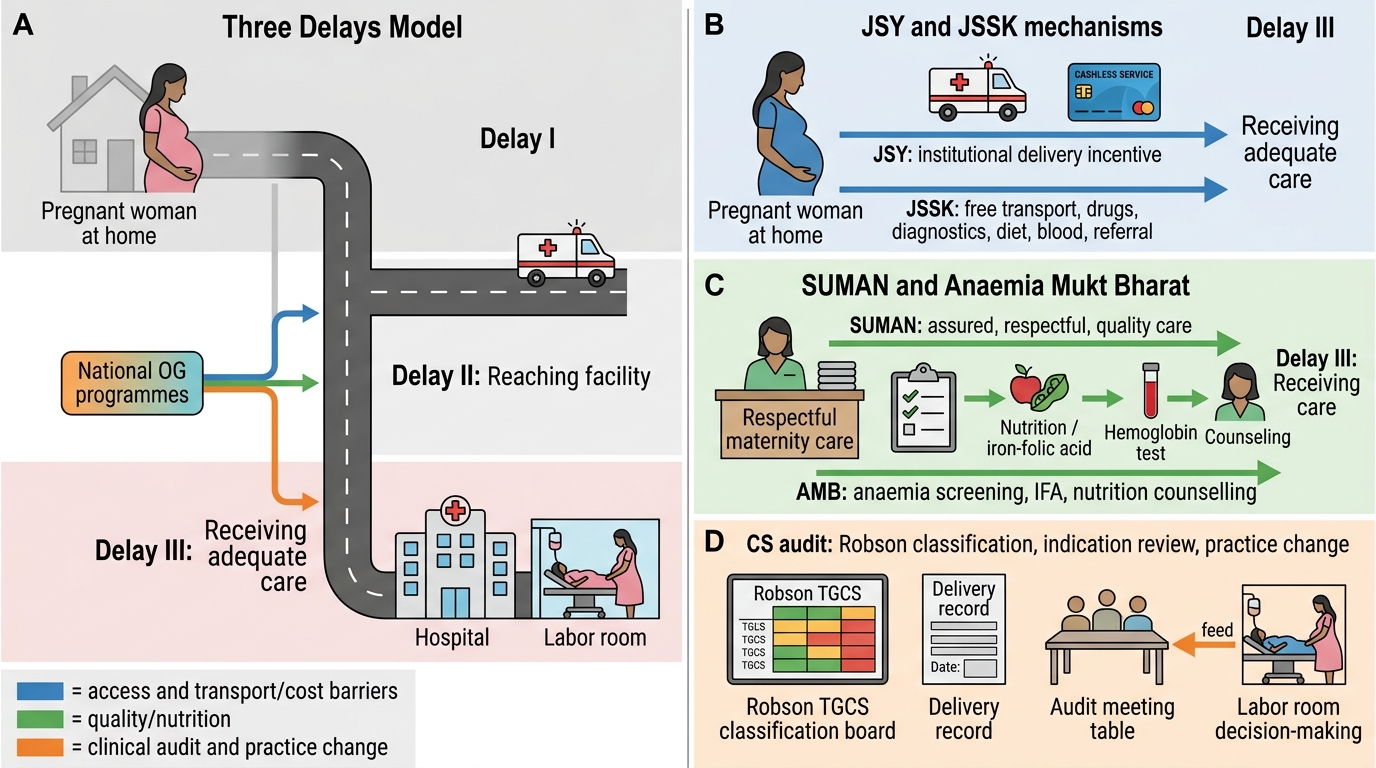
National OG Programmes and the Three Delays Model
Clinical and Applied Significance for the Practising Obstetrician
For the practising obstetrician or medical officer, the practical implications of this module consolidate into four domains of clinical responsibility.
First, documentation and classification: Every delivery must be classified into a Robson group at the time of discharge. In facilities that conduct regular TGCS audits, this means recording parity, previous CS status, presentation, onset of labour, gestational age, and number of fetuses for every patient — not retrospectively, but prospectively as part of the delivery record. Facilities with electronic medical records increasingly automate this classification, but the clinician must ensure the underlying data are accurate. Accurate Robson classification requires knowing whether a CS was pre-labour (elective) or in-labour — a distinction that must be made at the time of the decision, not reconstructed later.
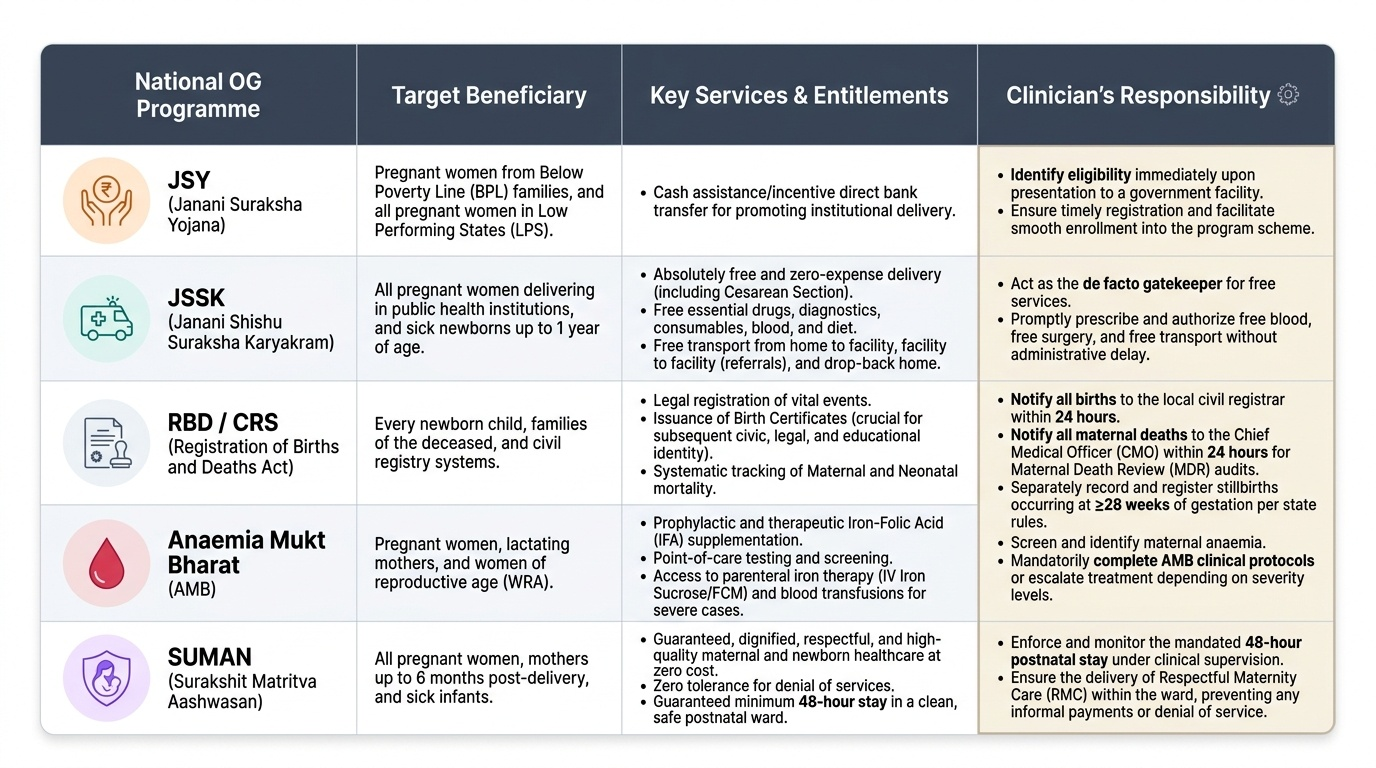
Second, programme enrolment and entitlement: When a woman presents to a government facility in labour, the clinician or the team must identify her entitlements. Is she JSY-eligible? (Is this a BPL woman, or is she in a LPS where JSY is universal?) Does she require JSSK services — free blood, free surgery, free transport? Does she have anaemia requiring AMB protocol completion or treatment escalation? Is she entitled to 48-hour postnatal stay under SUMAN? These are not administrative questions — they are clinical responsibilities, and in many district hospitals, the medical officer is the de facto gatekeeper for these services.
Third, birth and death registration: The RBD Act places specific notification and registration obligations on facility medical officers. All births must be notified within 24 hours to the local civil registrar; the birth certificate is a legal document required for every child's subsequent civic and educational identity. All maternal deaths must be notified to the CMO within 24 hours for MDR purposes. Stillbirths at ≥28 weeks must be separately recorded and registered per state rules.
Fourth, audit participation: The Robson TGCS audit is most effective when clinicians who care for patients also participate in reviewing the audit output. A departmental audit meeting that reviews monthly Robson data creates accountability — clinicians see where their Group 5 CS rate sits relative to a facility attempting VBAC, and this comparative data is often more persuasive than guidelines alone.
Provided image
Self-Assessment
Effective self-assessment at this stage requires you to move from recognition to active recall — close this module and try to answer each prompt from memory before checking. The Robson groups are a common examination target precisely because they require exact definitions, not approximations; getting Group 3 and Group 4 mixed up (spontaneous vs induced multiparous) is the commonest error. National programme details are often tested as scenario-based questions: a given patient is described and you must identify which scheme applies, what she is entitled to, and what your documentation obligation is. Both domains — Robson classification and national programme knowledge — require a level of precision that rewards active self-testing rather than passive review. Use the prompts below to test both domains carefully, then return to the relevant sections for any gaps before proceeding to the cluster assessment.
Robson groups — can you recall?
• Which group does a woman with a previous CS, singleton cephalic at term belong to, regardless of labour onset? (Group 5)
• Which group captures ALL preterm singleton cephalic deliveries, including those with a previous CS? (Group 10)
• Which two groups typically have the highest absolute contribution to the overall CS rate in India? (Groups 2 and 5)
National programmes — can you recall?
• What is the cash entitlement under JSY for a rural woman delivering in an LPS? (Rs 1,400)
• What does JSSK provide beyond what JSY provides? (Free services — drugs, diagnostics, blood, diet, transport — not just cash)
• Which scheme provides a 6×6×6 framework targeting anaemia? (Anaemia Mukt Bharat)
• What minimum ANC visits does SUMAN guarantee? (4 visits)
• What must you do within 24 hours of a maternal death at your facility? (Notify CMO; initiate MDR proforma)
SELF-CHECK
A 30-year-old woman with two previous caesarean sections presents at 38 weeks with a singleton cephalic fetus. She is admitted for her third delivery. Which Robson group does she belong to?
A. Group 3 (multiparous, no previous CS, spontaneous labour)
B. Group 4 (multiparous, no previous CS, induced)
C. Group 5 (previous CS, singleton cephalic, ≥37 weeks)
D. Group 10 (preterm singleton cephalic)
Reveal Answer
Answer: C. Group 5 (previous CS, singleton cephalic, ≥37 weeks)
Group 5 captures ALL women with a previous caesarean section who have a singleton cephalic presentation at ≥37 weeks — regardless of the number of previous sections (one or more), regardless of whether this delivery starts spontaneously or is induced/planned. Group 3 and 4 specifically exclude women with previous CS. Group 10 is for preterm (<37 weeks); this woman is at 38 weeks.
CLINICAL PEARL
Group 5 is the linchpin of CS audit in India. In most Indian tertiary and district hospitals, Group 5 (previous CS, term, singleton cephalic) is the single largest contributor to the overall CS rate — because once a woman has had one CS, the default in most facilities is a repeat elective CS. A facility's Group 5 CS rate can exceed 90%. The evidence-based alternative — trial of labour after caesarean (TOLAC) / vaginal birth after caesarean (VBAC) — is underutilised because of: concerns about uterine rupture risk (0.5–1% in appropriately selected women with one previous lower-segment CS), lack of trained staff for TOLAC monitoring, medicolegal anxiety, and patient expectation of repeat CS. In a Robson audit, an institution targeting CS rate reduction almost always has to address Group 5. The clinical pearl for the examination: 'the group that is large AND has a high CS rate is the group with the greatest potential for improvement' — not the rare group with a 100% CS rate (e.g., Group 9, transverse lie), which, although inevitable, is too small to move the overall rate significantly.