Page 9 of 32
OG17.3 | Mastitis and Breast Abscess — SDL Guide
Learning Objectives
- Describe the clinical features of mastitis and breast abscess and differentiate them from breast engorgement
- Explain the pathophysiology of the progression from milk stasis to non-infective mastitis, infective mastitis, and breast abscess
- Outline the diagnostic approach to mastitis and breast abscess including the role of breast milk culture and ultrasound
- State the evidence-based management of mastitis including the rationale for continuing breastfeeding and the appropriate antibiotic regimen
- Describe the indications and technique for incision and drainage of a breast abscess
INSTRUCTIONS
Mastitis is a common and distressing complication of breastfeeding, affecting approximately 10% of lactating women. Left untreated or incorrectly managed — particularly when breastfeeding is stopped — it progresses to breast abscess requiring surgical drainage. This module covers the full spectrum from milk stasis to abscess, with emphasis on the two management principles that most often go wrong in clinical practice: continuing breastfeeding during mastitis, and using an antibiotic that covers Staphylococcus aureus adequately.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 17 — Complications of the Puerperium (textbook)
- WHO, Mastitis: Causes and Management, WHO/FCH/CAH/00.13, 2000 (guideline)
- Williams Obstetrics, 25th ed., Ch. 36 — Puerperal Infections (textbook)
- Shaw's Textbook of Gynaecology, 17th ed. — Breast Complications in the Puerperium (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old primipara on postpartum day 10 calls the postnatal clinic complaining of a painful, red, swollen right breast and a fever of 38.8°C. She is breastfeeding but says the right breast is 'like a rock' and the baby refuses to feed from it. Her mother has advised her to stop breastfeeding immediately and 'rest the breast'. She asks whether she should stop feeding and whether she needs antibiotics. How do you advise her — and what is the single most important instruction that, if missed, puts her at risk of a breast abscess?
WHY THIS MATTERS
Mastitis affects approximately 1 in 10 breastfeeding women and is one of the most common reasons for premature breastfeeding cessation. The two management errors you will most frequently encounter — and must be equipped to correct — are: (1) advising the mother to STOP breastfeeding (which worsens milk stasis and accelerates abscess formation), and (2) prescribing an antibiotic that does not adequately cover Staphylococcus aureus (e.g. ampicillin or co-amoxiclav alone without anti-staphylococcal cover). As a clinician, knowing when mastitis has progressed to abscess — and what to do about it — is an essential inpatient and outpatient skill.
RECALL
Activate prior knowledge:
- Milk stasis and galactopoiesis: From the lactation physiology module — incomplete emptying of the breast raises back-pressure on the alveoli, compresses capillaries, and disrupts tight junctions between alveolar cells. Continued adequate drainage (via effective suckling or expression) prevents this cascade.
- Nipple-areola complex innervation: The nipple-areola is richly innervated; fissures and cracks (from poor latch) breach the epithelial barrier, providing a portal of entry for skin commensals — particularly Staphylococcus aureus.
- Perinatal fever differential: Fever in the puerperium has a structured differential — endometritis, urinary tract infection, wound infection, deep vein thrombosis, mastitis. Context (lactating, breast signs) directs the diagnosis.
- Antibiotic principles: Staphylococcus aureus is typically penicillinase-producing (MRSSA in community = MSSA; MRSA less common). Cloxacillin (a penicillinase-resistant penicillin) and cephalexin (first-generation cephalosporin) provide effective cover.
Clinical Presentation: How Mastitis and Breast Abscess Present
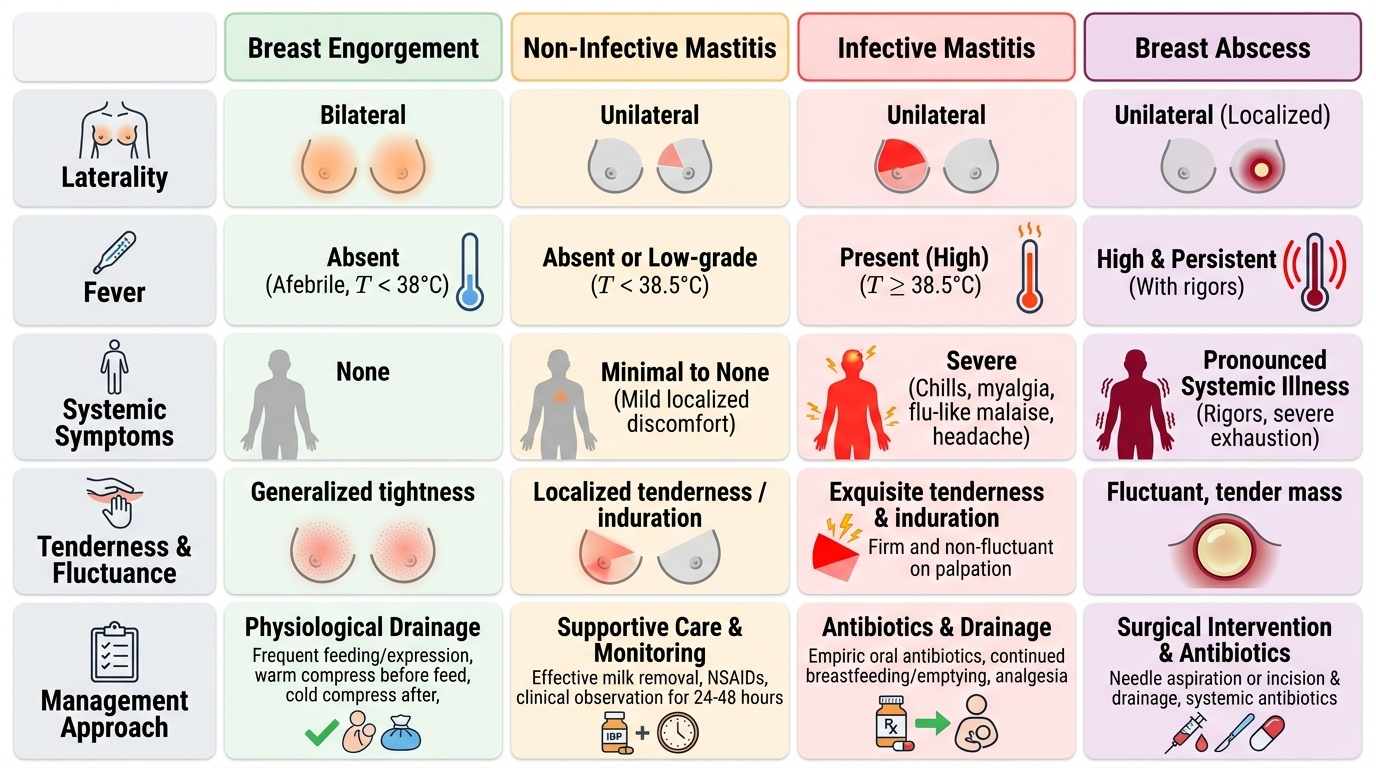
Mastitis is defined as inflammation of the breast parenchyma in a lactating woman, which may or may not be associated with bacterial infection. The clinical distinction between non-infective and infective mastitis is important for management but cannot always be made on clinical grounds alone; in practice, most cases presenting to a clinician with fever and systemic symptoms are treated as infective — with antibiotics — because the consequences of under-treating genuine infective mastitis (progression to abscess) are far more serious than the consequences of prescribing a short antibiotic course for non-infective mastitis. Mastitis affects approximately 10% of breastfeeding women, most commonly in the first 6–12 weeks postpartum. Recognising its characteristic features and distinguishing it from the physiological engorgement of lactogenesis II is a fundamental postnatal ward skill.
The typical clinical presentation of infective lactational mastitis is:
- Timing: Most commonly in the first 6–12 weeks postpartum, with a peak at 2–3 weeks; can occur at any time during lactation
- Laterality: Characteristically unilateral (in contrast to engorgement, which is bilateral)
- Local signs: A wedge-shaped area of erythema, warmth, tenderness, and induration corresponding to one or more affected lobes; the affected segment is firm and exquisitely tender to palpation
- Systemic signs: Fever (often >38.5°C), chills, myalgia, flu-like malaise, headache — distinguishing features from simple engorgement (which is afebrile)
- Breast feeding pattern: The baby may feed poorly from the affected breast (reduced let-down due to pain and oedema compressing ducts); the mother may be reluctant to feed due to discomfort
Breast abscess represents the failure of mastitis treatment — inadequate antibiotic therapy, cessation of breastfeeding (worsening stasis), or delayed presentation. It presents as:
- A localised, fluctuant, tender swelling within the inflamed area
- Skin overlying the abscess may be red, shiny, or oedematous
- High fever, rigors, and pronounced systemic illness
- Possible spontaneous discharge of pus through the skin
The clinical differential must always include breast engorgement (bilateral, afebrile, usually days 2–5 postpartum, no systemic illness) and, in older women or those not breastfeeding, inflammatory breast carcinoma (progressive skin changes — peau d'orange, nipple retraction — without fever, not associated with lactation). The latter is rare but must not be dismissed if mastitis fails to respond to treatment.
Provided image
Pathophysiology: From Milk Stasis to Abscess Formation
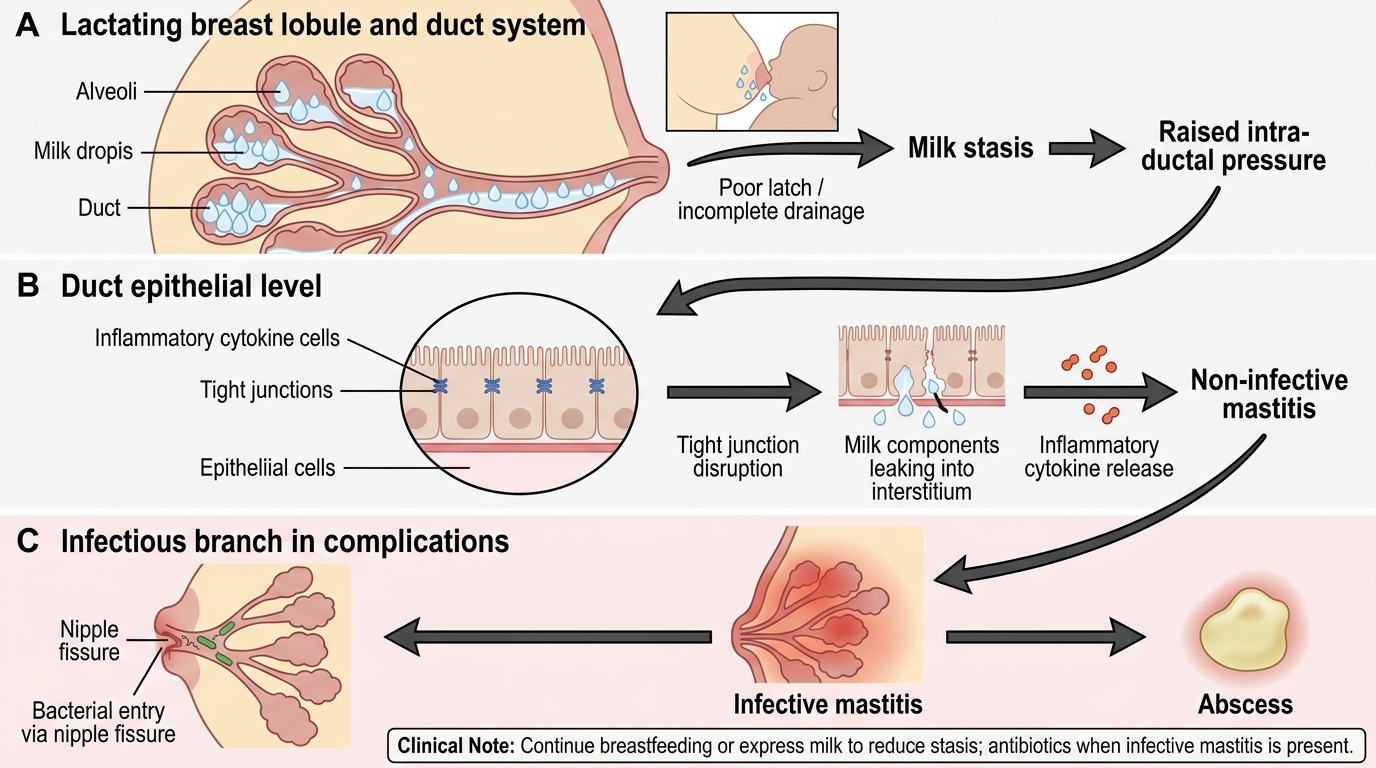
The pathophysiological progression from normal lactation to breast abscess follows a well-defined sequence, and understanding it clarifies why continuing breastfeeding is therapeutic rather than harmful during mastitis.
Stage 1 — Milk stasis: Any factor that impairs complete, regular emptying of the breast leads to milk accumulating within the alveoli and ducts. Common precipitants include: missed feeds or abrupt reduction in feeding frequency; poor latch resulting in incomplete drainage; physical pressure on the breast (tight bra, sleeping position); blocked duct from external compression or thick milk; maternal exhaustion or stress impairing the oxytocin let-down reflex. As milk accumulates, intra-alveolar pressure rises, compressing the pericapillary space and reducing local blood flow.
Stage 2 — Non-infective mastitis (ductal inflammation): Sustained raised pressure disrupts the tight junctions between alveolar epithelial cells, allowing milk proteins (particularly casein) and cellular debris to leak into the periductal connective tissue. This triggers a local inflammatory response — oedema, vasodilatation, and neutrophil infiltration — producing the warmth, erythema, and tenderness of mastitis without bacterial involvement. Milk culture at this stage is sterile or shows only skin commensals in low counts.
Stage 3 — Infective mastitis: The inflamed, congested periductal tissue and the disrupted epithelial barrier provide both a growth substrate and a portal of entry for bacteria. Staphylococcus aureus (the most common causative organism in >90% of cases) colonises the nipple-areola complex and ascends through cracks and fissures in the nipple to infect the stagnant milk and inflamed tissue. Less commonly, Staphylococcus epidermidis or group B Streptococcus are implicated. Milk culture now yields a significant growth (>10³ colony-forming units/mL of a single pathogen).
Stage 4 — Abscess: Untreated or undertreated infective mastitis allows progressive bacterial multiplication and tissue necrosis. A localised collection of pus develops, walled off by surrounding inflammatory tissue — this is the breast abscess. Once formed, an abscess cannot be eradicated by antibiotics alone (penetration into the pus cavity is poor, and bacteria sequestered in avascular necrotic tissue are protected from systemic antibiotics) — drainage is required.
The key mechanistic insight for management: emptying the breast at every stage reduces intra-alveolar pressure, restores epithelial tight junction integrity, removes the bacterial growth medium (stagnant milk), and facilitates antibiotic penetration into periductal tissue. This is why continuing breastfeeding is a therapeutic intervention in mastitis, not merely a recommendation for the infant's benefit.
Progression from Milk Stasis to Breast Abscess
SELF-CHECK
A lactating woman with infective mastitis is advised by a relative to stop breastfeeding to 'rest' the affected breast. Why is this advice harmful?
A. Stopping breastfeeding lowers prolactin and reduces mastitis inflammation
B. Stopping breastfeeding increases milk stasis, raises intra-alveolar pressure, and accelerates abscess formation
C. Stopping breastfeeding causes oxytocin deficiency that worsens breast engorgement
D. Stopping breastfeeding is harmless — the antibiotic alone is sufficient treatment
Reveal Answer
Answer: B. Stopping breastfeeding increases milk stasis, raises intra-alveolar pressure, and accelerates abscess formation
Cessation of breastfeeding during mastitis is counterproductive. The underlying driver of mastitis progression is milk stasis — continued milk production without drainage increases intra-alveolar pressure, maintains the bacterial growth medium, and significantly accelerates progression to abscess formation. The correct management is to continue frequent breastfeeding (or expression if feeding is too painful) to empty the breast regularly, alongside antibiotic therapy. Both measures are required for effective mastitis treatment.
Diagnosis: Clinical and Laboratory Assessment
The diagnosis of mastitis is primarily clinical — a combination of the local breast signs (unilateral erythema, warmth, tenderness, induration) and systemic features (fever ≥38°C, flu-like malaise) in a lactating woman is usually sufficient to initiate treatment without waiting for laboratory results. Investigation is reserved for specific clinical situations: treatment failure, severe systemic illness, or diagnostic uncertainty about whether a collection has formed. Overinvestigating straightforward mastitis delays antibiotic initiation and is not necessary; underinvestigating mastitis that fails to respond at 72 hours risks missing a developing abscess that requires drainage. The decision framework is therefore: initiate empirical treatment immediately on clinical grounds, and investigate selectively based on the clinical response trajectory.
Clinical diagnosis:
The combination of a localised, erythematous, warm, tender breast segment in a breastfeeding woman with fever (≥38°C) and flu-like symptoms is diagnostic of infective mastitis. No investigation is required to begin treatment in a straightforward case.
Breast milk culture:
Indicated in the following situations:
- Mastitis that does not respond to 48–72 hours of standard antibiotic therapy (suggests a resistant organism — consider MRSA, particularly in hospital-acquired or recurrent cases)
- Severe or hospitalised mastitis
- Recurrent mastitis in the same mother
- Mastitis in a neonate who develops signs of infection (potential cross-infection)
Technique: the first milk of the feed is discarded (contaminated with skin flora); the subsequent mid-stream milk from the affected breast is collected directly into a sterile container. A significant growth is defined as >10³ CFU/mL of a single pathogen.
Breast ultrasound:
The most useful investigation when abscess is suspected — differentiates a simple, treatable mastitis (no collection) from an abscess (echo-free or hypoechoic collection with posterior acoustic enhancement). Even experienced clinicians can miss a deep abscess on palpation; early ultrasound reduces the time to drainage and prevents progression of the collection. Ultrasound also guides needle aspiration for smaller (<5 cm) abscesses as an alternative to formal I&D.
Blood tests:
Full blood count (leukocytosis with neutrophilia confirms infection, helps gauge severity) and C-reactive protein may be performed in severe cases or in women who appear systemically unwell. Blood cultures should be taken before antibiotics in women with high fever (≥39°C), rigors, or features suggesting septicaemia.