Page 10 of 32
OG17.3 | Mastitis and Breast Abscess — SDL Guide (Part 2)
Management of Mastitis: Antibiotics, Continued Breastfeeding, and Supportive Measures
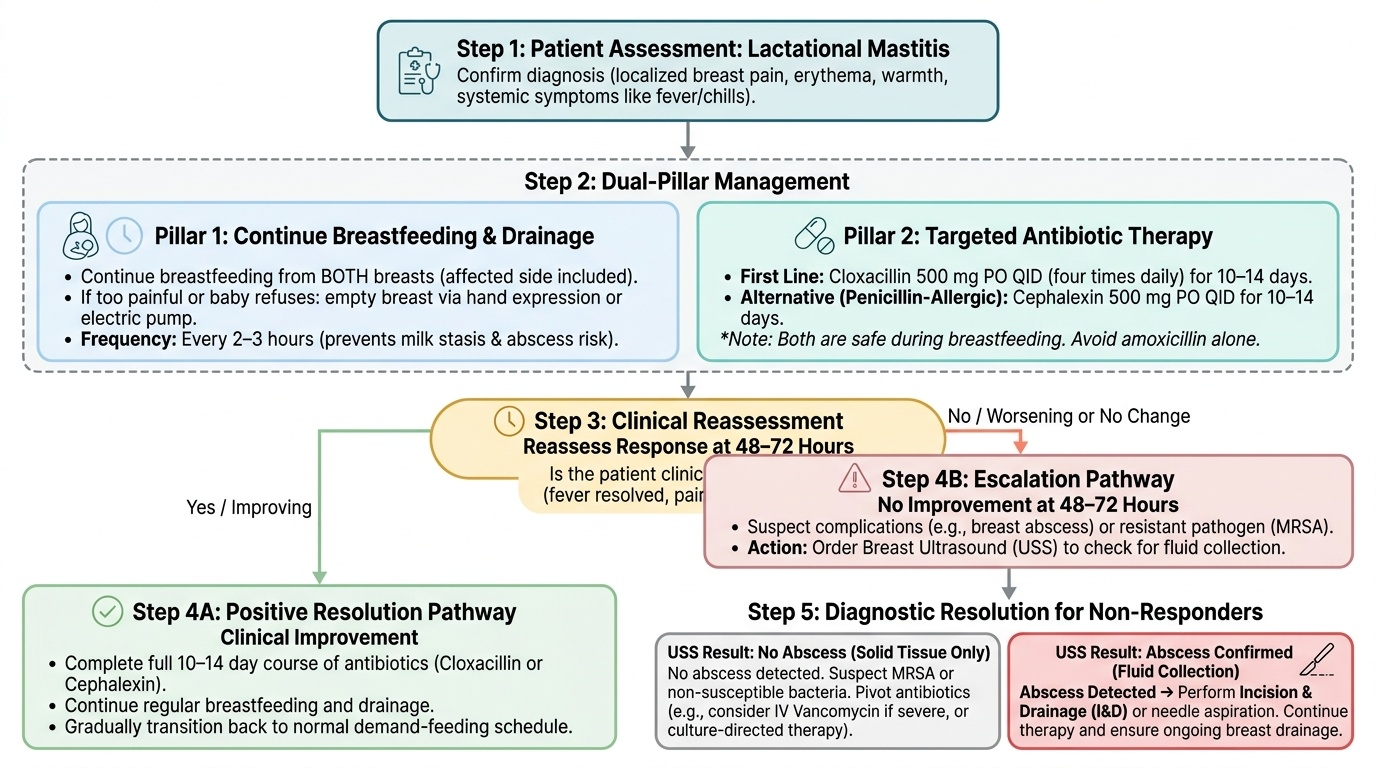
The management of lactational mastitis rests on three simultaneous pillars: effective breast drainage, targeted antibiotic therapy, and supportive measures. All three must be applied together — antibiotics alone without drainage are inadequate, and drainage without antibiotics in infective mastitis risks progression.
Pillar 1 — Continue breastfeeding and ensure adequate drainage:
The evidence-based recommendation from WHO (2000) and all major obstetric guidelines is to continue breastfeeding from both breasts — including the affected breast — throughout mastitis treatment. This is the single most therapeutically important instruction. If feeding from the affected breast is too painful or the baby refuses (due to altered milk taste from infection), the breast must be emptied by hand expression or electric pump at the same frequency as feeds (every 2–3 hours). Effective emptying reduces intra-alveolar pressure, removes the bacterial growth medium, and facilitates antibiotic penetration. Cessation of breastfeeding during mastitis significantly increases the risk of abscess formation.
Pillar 2 — Antibiotic therapy:
The causative organism in >90% of lactational mastitis cases is Staphylococcus aureus, typically a penicillinase-producing (beta-lactamase-producing) community-acquired strain. The antibiotic of choice must provide reliable cover against this organism:
- Cloxacillin (dicloxacillin/flucloxacillin in some regions): 500 mg orally four times daily for 10–14 days. A penicillinase-resistant penicillin — the drug of choice in most settings.
- Cephalexin (cefalexin): 500 mg four times daily for 10–14 days. An acceptable alternative (first-generation cephalosporin with excellent Staph aureus cover); useful if penicillin-allergic patients can tolerate cephalosporins (cross-reactivity ~1–2%).
- Both cloxacillin and cephalexin are safe during breastfeeding (excreted in very low concentrations in breast milk; not harmful to the infant at these levels).
- Avoid: amoxicillin or amoxicillin-clavulanate alone (inadequate against penicillinase-producing Staph in most community settings unless sensitivity data confirm susceptibility).
- MRSA: Suspected in mastitis not responding to 48–72 h of cloxacillin, in hospital-acquired cases, or in known MRSA carriers — requires vancomycin (IV, for severe cases) or trimethoprim-sulfamethoxazole/linezolid (oral, mild-to-moderate). Send milk culture before switching.
- Antibiotic course: minimum 10–14 days — a shorter course increases the risk of abscess and recurrence.
Pillar 3 — Supportive measures:
- Analgesics and anti-inflammatory agents: Ibuprofen (400 mg TID) is preferred — it provides both analgesia AND anti-inflammatory effect (reduces periductal oedema) and is safe during breastfeeding. Paracetamol as an alternative.
- Warm compress before feeds: promotes vasodilation and let-down, facilitates drainage
- Cold compress after feeds: reduces oedema and provides pain relief
- Rest: maternal exhaustion impairs the let-down reflex and exacerbates milk stasis
- Hydration and nutrition: systemic inflammatory response increases metabolic demands
Clinical response to antibiotics should be evident within 48–72 hours (reduction in fever, improved local signs). If no response at 72 hours, reassess: consider ultrasound for occult abscess, milk culture for resistant organism, or review of antibiotic compliance.
Provided image
SELF-CHECK
A 30-year-old breastfeeding mother on day 12 postpartum presents with left breast mastitis. Which of the following is the most appropriate antibiotic?
A. Amoxicillin 500 mg TID for 5 days
B. Cloxacillin 500 mg QID for 10–14 days
C. Metronidazole 400 mg TID for 7 days
D. Azithromycin 500 mg once daily for 3 days
Reveal Answer
Answer: B. Cloxacillin 500 mg QID for 10–14 days
The causative organism in lactational mastitis is Staphylococcus aureus in over 90% of cases, typically a penicillinase-producing strain. Cloxacillin (a penicillinase-resistant penicillin) 500 mg four times daily for 10–14 days is the antibiotic of choice. Amoxicillin alone does not reliably cover penicillinase-producing Staph aureus. Metronidazole covers anaerobes but not Staph. Azithromycin (macrolide) has variable Staph coverage and a 3-day course is inadequate for mastitis.
Management of Breast Abscess: Incision and Drainage
Breast abscess represents failure of mastitis treatment — whether from delayed presentation, an inadequate antibiotic choice, a course that was too short, or — most commonly and most preventably — cessation of breastfeeding that allowed milk stasis to persist and the infective process to advance unchecked. Once pus has collected into a walled-off cavity, antibiotics alone are insufficient because their penetration into an avascular, pus-filled cavity with high bacterial density and an acid microenvironment is negligible. Drainage is the definitive treatment; the antibiotic role at this stage is to treat the surrounding cellulitis and prevent recurrence rather than to eradicate the collection itself. Two drainage modalities are available — the choice between them depends on abscess size, loculation, and clinical context.
Clinical recognition:
An abscess should be suspected when mastitis does not respond to 72 hours of appropriate antibiotics, and confirmed by the presence of fluctuance on palpation (the skin feels boggy and pits, and pressure at one margin causes a 'fluid thrill' at the opposite margin). However, deep abscesses — particularly in large or engorged breasts — may not be clinically fluctuant; ultrasound is essential when abscess is suspected and examination is uncertain.
Drainage options:
1. Needle aspiration (ultrasound-guided): Suitable for smaller (<5 cm diameter), unilocular abscesses; can be repeated if the collection re-accumulates; preserves breast cosmesis and may be performed under local anaesthesia in the outpatient setting. Multiple aspirations may be needed.
2. Incision and drainage (I&D): Required for large, multilocular, or deep abscesses, or those that fail needle aspiration. Performed under local or general anaesthesia. Key technical points:
- Incision at the areolar margin (periareolar incision — parallel to the areola) provides better cosmesis; alternatively, at the point of maximum fluctuance if the abscess is peripheral
- Incision of adequate length to allow complete evacuation of pus
- Break up loculations with a finger or blunt haemostat to ensure all pockets are drained
- Wound irrigated with saline; may be loosely packed with gauze (removed at 24–48 hours) or left open for secondary healing
- Send pus for culture and sensitivity to guide antibiotic adjustment
3. Antibiotics post-drainage: Continue anti-staphylococcal antibiotics for 10–14 days after drainage.
Breastfeeding after abscess:
- Contralateral breast: Continue breastfeeding from the unaffected breast throughout treatment — this maintains supply and benefits the infant.
- Affected breast: If the incision does not involve the areola or main ductal system, breastfeeding or expression can often resume from the affected breast once pain allows (drainage reduces pressure and usually relieves the feeding block). If the incision is periareolar or involves major ducts, temporary cessation from that breast with expression (discarded) may be necessary until the wound heals.
- Milk safety: Pus should not be fed to the infant; however, milk from an unaffected quadrant of the breast (away from the abscess) is generally considered safe.
Self-Assessment: Mastitis Spectrum and Management Decision-Making
This section consolidates your understanding of the mastitis spectrum through case-based reasoning. The key clinical decisions in mastitis management — distinguishing mastitis from engorgement, recognising abscess formation, choosing the right antibiotic and course length, and knowing when to refer for drainage — are high-yield examination topics at the final MBBS level and represent real decisions you will make as a junior doctor on postnatal wards and in outpatient settings. Working through these scenarios requires simultaneously applying the pathophysiology (milk stasis cascade), the diagnostic approach (clinical vs USS vs culture), and the management principles (drain + antibiotics + continue breastfeeding) covered in this module. For each scenario, formulate your answer before reading the explanation — active retrieval is more effective than passive reading for consolidating clinical decision-making skills.
Self-assessment questions:
- A breastfeeding mother on day 9 postpartum has right breast pain, erythema, and a temperature of 38.6°C. She has been taking co-amoxiclav (amoxicillin-clavulanate) for 3 days without improvement. What is the most likely reason for treatment failure, and what is the next step?
- A 25-year-old primipara on day 14 postpartum presents with a 4 × 3 cm fluctuant, tender right breast swelling. She is febrile at 39.2°C. Ultrasound confirms a unilocular collection. Outline the management plan, including the decision between needle aspiration and I&D, continuation of breastfeeding, and antibiotic choice.
- Explain to a medical student why advising a woman with mastitis to 'stop breastfeeding and rest the breast' is pathophysiologically counterproductive.
- What features on the history and examination would suggest mastitis is NOT a simple lactational mastitis and requires further investigation (e.g. inflammatory breast cancer or TB mastitis)?
SELF-CHECK
A breastfeeding mother presents with a 5 × 4 cm fluctuant, tender right breast swelling confirmed on ultrasound as a unilocular abscess. She has been on cloxacillin for 3 days without improvement. What is the most appropriate next management step?
A. Switch antibiotics to vancomycin and continue without drainage
B. Advise the mother to stop breastfeeding and observe for 48 hours
C. Incision and drainage (or ultrasound-guided aspiration) + continue antibiotics + continue breastfeeding from the contralateral breast
D. Mastectomy of the affected breast
Reveal Answer
Answer: C. Incision and drainage (or ultrasound-guided aspiration) + continue antibiotics + continue breastfeeding from the contralateral breast
A confirmed breast abscess that has not resolved on antibiotics requires drainage — either ultrasound-guided needle aspiration (for smaller unilocular abscesses) or formal incision and drainage (for large or multilocular collections). Antibiotics alone cannot penetrate an avascular pus collection. Breastfeeding should continue from the contralateral breast. The ipsilateral breast may resume feeding or expression once the wound allows. Mastectomy is never indicated for lactational breast abscess.
CLINICAL PEARL
Never stop breastfeeding in mastitis — stopping is the most preventable cause of breast abscess. The management instruction that most often goes wrong in clinical practice is advising the mother to 'rest the breast' by stopping feeding. Milk stasis is both the cause and the perpetuating factor in mastitis; removing the drainage mechanism accelerates pus formation. The correct advice is: keep feeding frequently (8–12 times per 24 h), start cloxacillin or cephalexin immediately, use ibuprofen for pain and inflammation, and return if there is no improvement in 48–72 hours. This three-step approach — drain, antibiotics, anti-inflammatory — prevents the vast majority of abscesses.