Page 12 of 32
OG18.{1,3} | Newborn Assessment and Birth Asphyxia — SDL Guide
Learning Objectives
- Describe the components of the APGAR score, the correct method of assessment at 1 and 5 minutes, and the clinical interpretation of each score range
- Distinguish APGAR score from Bishop score in terms of parameters, context, and purpose
- Describe the New Ballard Score criteria for gestational age estimation and state when it is clinically indicated
- Outline a systematic head-to-toe newborn examination, identifying normal variants and red flags
- Define birth asphyxia and describe its pathophysiology including the sequence from primary to secondary apnoea and multi-organ consequences
- Identify the antenatal and intrapartum risk factors for birth asphyxia
- Describe the approach to documentation, communication, and follow-up for a neonate with suspected birth asphyxia
INSTRUCTIONS
The assessment of the newborn at birth is one of the most time-critical clinical skills in obstetric practice. The APGAR score, performed at 1 and 5 minutes of life, determines whether the neonate requires immediate resuscitation. Understanding what each of its five parameters measures — and equally, what it does not — is fundamental. This module also covers maturity assessment, the systematic newborn examination, and the pathophysiology of birth asphyxia, building the conceptual foundation for the resuscitation skills module that follows.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 18 — The Newborn (textbook)
- Williams Obstetrics, 25th ed., Ch. 32 — The Newborn Infant (textbook)
- Ballard JL et al, New Ballard Score, expanded to include extremely premature infants. J Pediatr 1991;119:417–423 (journal)
- Apgar V, A proposal for a new method of evaluation of the newborn infant. Curr Res Anesth Analg 1953;32:260–267 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A term baby is delivered by emergency caesarean section for fetal distress. At birth, the baby is limp, blue, and not crying. The obstetrician calls out: 'APGAR!' — and you need to assess it immediately. You score it mentally: no cry (respiratory effort 0), central cyanosis (colour 1), no active movement (tone 0), no response to stimulation (reflex 0), heart rate 80 bpm (HR 1) — APGAR 2/10 at 1 minute. What does this tell you, what happens next, and how does this differ from a baby who scores 5/10? This module gives you the framework to answer those questions with precision — and to do so under time pressure, at the resuscitation trolley.
WHY THIS MATTERS
Newborn assessment at birth is an obstetric responsibility — before the paediatrician arrives, it is the delivering obstetrician or midwife who performs the APGAR, initiates resuscitation if needed, and makes the first call about whether the neonate is well or compromised. The APGAR score is not merely a number to document: it is a structured clinical decision tool that directs immediate management. Beyond the delivery room, the systematic newborn examination identifies life-threatening congenital anomalies (cardiac defects, palatal clefts, developmental hip dysplasia) in the first 24 hours — a window in which early intervention dramatically changes outcomes. And recognising birth asphyxia — its causes, its organ consequences, and its documentation — is essential for clinical management and, in a medicolegal context, for accurate and defensible clinical records.
RECALL
Before proceeding, activate prior knowledge:
- Fetal circulation and transition at birth: Recall the foramen ovale (right-to-left shunt, closes functionally at birth), ductus arteriosus (connects pulmonary artery to aorta; closes with oxygen exposure and prostaglandin fall), and the drop in pulmonary vascular resistance as the lungs inflate with air. These transitions are disrupted by asphyxia.
- Bishop score (NOT APGAR): The Bishop score assesses cervical favourability for induction — its five parameters are dilatation, effacement, station, consistency, and position (score 0–13). This is entirely different from the APGAR score. This distinction is a known examination trap.
- Gestational age definitions: Term = 37–42 completed weeks; preterm = <37 weeks; post-term = ≥42 weeks. Maturity assessment is used when gestational age is uncertain.
- Definitions of low birth weight: LBW <2500 g; VLBW <1500 g; ELBW <1000 g. Small-for-gestational-age (SGA) = weight <10th centile for gestational age.
Orientation: Why Newborn Assessment Matters in Obstetric Practice
The transition from fetal to neonatal life is one of the most physiologically demanding events in human biology. In the fetus, gas exchange occurs across the placenta; at birth, the lungs must inflate with air within the first few breaths, the pulmonary vascular resistance must fall precipitously to allow blood flow through the lungs, and the foramen ovale and ductus arteriosus must functionally close as oxygenated blood from the lungs begins to circulate systemically. This transition takes seconds to minutes — and when it fails, the consequences for the neonatal brain and other organs are measured in minutes. The obstetrician and attending midwife are the first clinicians present at this transition, and their ability to recognise whether it is proceeding normally or failing is directly life-saving.
Newborn assessment encompasses three time-sensitive domains that the obstetric team must master:
- Immediate assessment (birth to 5 minutes): Is the baby breathing? Is the heart rate adequate? Is tone present? — the APGAR assessment framework guides these questions and determines whether resuscitation is required.
- Maturity assessment (first 12–96 hours): What is the gestational age? — the Ballard score provides an independent estimate when antenatal dating is uncertain, which is common in India where antenatal ultrasound access is uneven.
- Systematic newborn examination (within 24 hours of birth): Are there congenital anomalies, birth injuries, or physiological variants that require immediate action or parental counselling?
The APGAR score, developed by anaesthesiologist Virginia Apgar in 1952, is the universal tool for rapid newborn assessment at 1 and 5 minutes. Its five parameters — scored 0–2 each — provide a structured, reproducible, and communicable summary of the newborn's immediate physiological status. It is not a diagnosis of birth asphyxia (a common misconception), but it is the trigger for resuscitation and the first line of clinical documentation of the newborn's condition at birth.
Assessment of Gestational Maturity: The Ballard Score
The New Ballard Score (NBS), published by Ballard et al. in 1991, is the standard tool for estimating gestational age from physical and neuromuscular examination of the neonate. It is particularly valuable when antenatal ultrasound-based gestational age estimation is unavailable, uncertain, or discrepant — a situation common in resource-limited settings. It can be applied from 12 to 96 hours after birth and covers gestational ages from 20 to 44 weeks.
The score comprises two domains — neuromuscular maturity and physical maturity — each with six criteria, scored on a scale from -1 to 5 (or -1 to 4 for some items). The total score ranges from -10 (extreme prematurity, 20 weeks) to +50 (post-term, 44 weeks), with each 2-point increase in total score corresponding to approximately 1 week of gestational age.
Neuromuscular maturity criteria (6 items):
- Posture: The resting posture of a premature infant is extended (hypotonic); a term infant lies in a flexed posture (flexion tone increases with maturity)
- Square window (wrist): Angle between forearm and palm when the wrist is flexed — decreases with maturity (90° at 20 weeks to 0° at term)
- Arm recoil: Passive extension then release of the elbow — recoil strength increases with maturity
- Popliteal angle: Extension of the knee from the flexed hip — angle decreases (tighter popliteal fossa) with increasing maturity
- Scarf sign: Horizontal movement of the infant's elbow across the chest toward the opposite shoulder — the term infant resists beyond the midline
- Heel-to-ear manoeuvre: Passive approximation of the foot to the ear — resistance increases with maturity
Physical maturity criteria (6 items): Skin texture (gelatinous → smooth → peeling at term), lanugo (abundant in preterm → sparse at term), plantar creases (none → full sole coverage), breast bud size, ear cartilage (pinna recoil), and genitalia (testicular descent/labia development).
The NBS is less accurate for extremely premature infants (<26 weeks) where the range of error is wider (±1–2 weeks). It should be interpreted alongside obstetric dating and postnatal growth parameters.
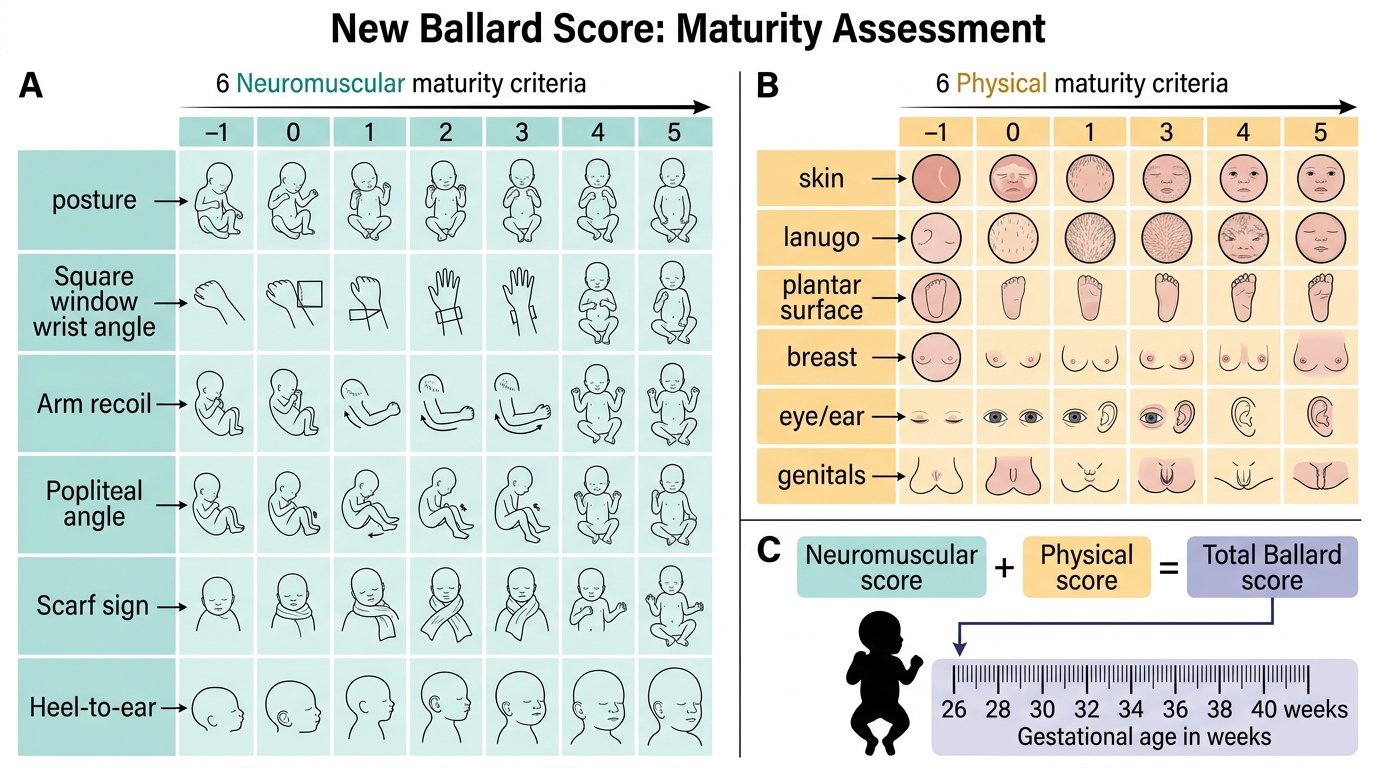
New Ballard Score for Neonatal Maturity Assessment
The APGAR Score: Assessment at Birth
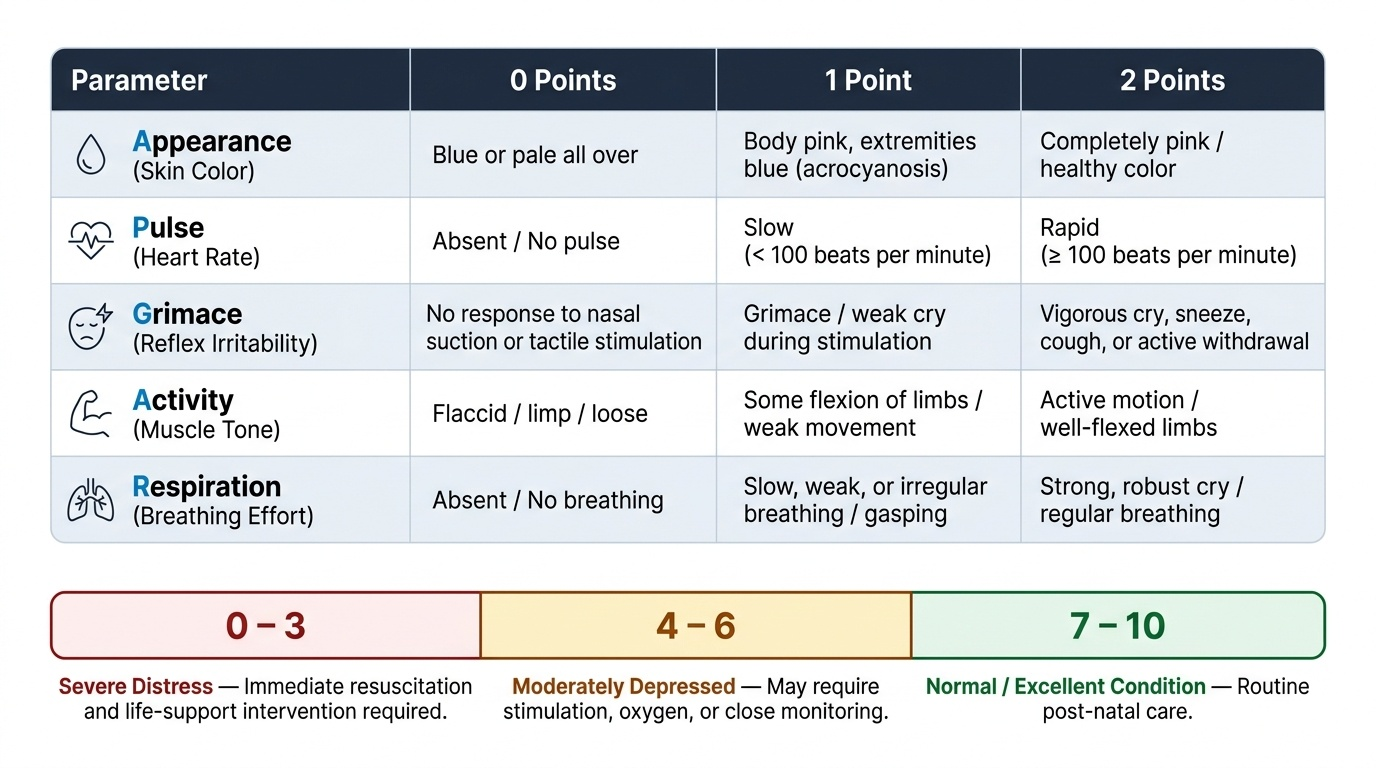
The APGAR score is a five-parameter clinical assessment of the newborn's physiological status, performed at 1 minute and 5 minutes after birth. Each parameter is scored 0, 1, or 2; the maximum possible score is 10. Proposed by anaesthesiologist Virginia Apgar in 1952, the score was designed to standardise the evaluation of the newborn's condition immediately after delivery and to provide a consistent, reproducible basis for deciding whether resuscitation was needed. The acronym APGAR stands for its five parameters: Appearance (colour), Pulse (heart rate), Grimace (reflex irritability), Activity (muscle tone), and Respiration. The five parameters collectively assess the three physiological systems that must function for neonatal survival: oxygenation (colour and respiration), perfusion (heart rate), and neurological integrity (tone and reflex response). Each can be assessed without equipment in under 60 seconds, making the APGAR a practical bedside tool for even the most resource-limited delivery environment.
The five parameters scored at each assessment:
| Parameter | 0 | 1 | 2 |
|---|---|---|---|
| Appearance (colour) | Blue/pale all over | Blue extremities, pink body | Pink all over |
| Pulse (heart rate) | Absent | <100 bpm | ≥100 bpm |
| Grimace (reflex irritability) | No response to stimulation | Grimace only | Cry, cough, or sneeze |
| Activity (muscle tone) | Limp | Some flexion of extremities | Active movement |
| Respiration | Absent | Slow, irregular, weak cry | Regular, good cry |
Timing and interpretation:
- 1-minute APGAR: Reflects the immediate condition at birth and identifies neonates requiring resuscitation. A 1-minute score of 0–3 indicates severe depression requiring immediate resuscitation. A score of 4–6 indicates moderate depression with possible need for stimulation and oxygen. A score of 7–10 is reassuring and generally requires only routine care.
- 5-minute APGAR: Reflects the response to initial resuscitation measures and is a better predictor of neonatal outcome and neurological prognosis than the 1-minute score. A 5-minute score that remains below 7 indicates an infant requiring ongoing assessment and possible escalation. Scores should be reassessed every 5 minutes thereafter if still below 7.
Important limitations — APGAR is NOT equivalent to birth asphyxia:
A low APGAR score has multiple causes beyond hypoxia — prematurity (normally lower tone and reflexes), sedation from maternal opioids or general anaesthesia, congenital neuromuscular disease, or primary cardiac arrhythmia. Conversely, some infants with documented birth asphyxia (cord gas pH <7.0, base excess <-12) may have APGAR scores >6 at 5 minutes. The APGAR score is therefore a trigger for action, not a standalone diagnosis of birth asphyxia. Cord blood gas values (pH, pCO₂, base excess) are the objective biochemical criterion.
IMARK: Never confuse APGAR with Bishop. Bishop score (0–13) assesses cervical favourability for induction using five obstetric parameters (dilatation, effacement, station, consistency, position). APGAR (0–10) assesses newborn status using five physiological parameters. Both are 5-parameter scores in obstetrics, but they apply to entirely different clinical contexts.
Provided image
SELF-CHECK
A term neonate is assessed at 1 minute of life: heart rate 90 bpm, weak irregular respiratory effort, limp with no active movement, grimace only to nasal catheter stimulation, body pink but extremities blue. What is the APGAR score?
A. APGAR 4 (HR=1, Resp=1, Tone=0, Reflex=1, Colour=1)
B. APGAR 5 (HR=1, Resp=1, Tone=0, Reflex=1, Colour=1) — same
C. APGAR 3 (HR=1, Resp=1, Tone=0, Reflex=0, Colour=1)
D. APGAR 6 (HR=2, Resp=1, Tone=0, Reflex=1, Colour=2)
Reveal Answer
Answer: A. APGAR 4 (HR=1, Resp=1, Tone=0, Reflex=1, Colour=1)
HR 90 bpm = score 1 (not absent, but <100). Weak irregular respiration = score 1. Limp tone = score 0. Grimace only = score 1. Body pink, extremities blue (acrocyanosis) = score 1. Total = 1+1+0+1+1 = 5. Note: options A and B both give 5; the question tests correct parameter assignment. A score of 5 at 1 minute indicates moderate depression requiring stimulation, supplemental oxygen, and close monitoring.