Page 13 of 32
OG18.{1,3} | Newborn Assessment and Birth Asphyxia — SDL Guide (Part 2)
Systematic Newborn Examination: Head-to-Toe Assessment
A systematic newborn examination should be completed within the first 24 hours of birth and documented in the case record. It serves three essential purposes: to identify life-threatening or surgically significant congenital anomalies requiring immediate intervention (cardiac defects, oesophageal atresia, palatal clefts, neural tube defects), to document the newborn's baseline physiological status, and to provide parents with accurate information and reassurance about their baby. The examination follows a reproducible head-to-toe sequence that ensures no region is omitted — deviation from a structured sequence is a common cause of missed diagnoses. In practice, the examination is conducted in a warm environment under a radiant heater, with the baby undressed and the parent present. Abnormal findings must be communicated to the neonatology team immediately; normal variants (such as Mongolian spots, milia, or erythema toxicum) must be distinguished from pathological signs and explained to parents to prevent unnecessary anxiety.
General assessment:
- Colour: Central cyanosis (tongue and mucosa blue) = abnormal; acrocyanosis (blue extremities, pink trunk) is normal in the first hours
- Tone: Term infants should be in a flexed posture with active resistance to passive extension; limp or extended posture is abnormal
- Cry: Strong cry = reassuring; high-pitched cry may indicate raised intracranial pressure; weak or absent cry = depression or neuromuscular problem
- Birthweight: Record and plot on centile chart; identify SGA (<10th centile) or LGA (>90th centile)
Head:
- Anterior fontanelle: Diamond-shaped, soft, flat; bulging = raised ICP; sunken = dehydration. Closes at 12–18 months.
- Posterior fontanelle: Triangular, small; closes by 6–8 weeks
- Sutures: Overriding sutures after delivery = normal moulding (resolves within days); craniosynostosis = premature fusion
- Caput succedaneum: Oedema of the scalp presenting part, crosses suture lines, resolves in 1–2 days; distinguished from cephalhaematoma (subperiosteal haemorrhage, does NOT cross suture lines, may calcify, resolves over weeks)
Eyes, ears, mouth:
- Check for subconjunctival haemorrhage (normal, birth trauma), red reflex (absence may indicate cataract or retinoblastoma)
- Ear pinna cartilage recoil (maturity indicator); low-set ears may indicate chromosomal anomaly
- Palate: Always check the hard and soft palate by inspection and digital palpation — a bifid uvula suggests a submucous cleft that will not be visible on inspection alone. Cleft palate requires early surgical planning and feeding support.
Cardiovascular:
- Auscultate for murmurs; note that many physiological murmurs are present in the first 24–48 hours as the ductus arteriosus closes. A harsh pansystolic murmur or a murmur with haemodynamic compromise warrants echocardiography.
- Femoral pulses: absent or weak femoral pulses + weak arms suggest coarctation of the aorta — a duct-dependent lesion that may decompensate within days
Abdomen and umbilicus:
- Umbilical cord: normally has two arteries and one vein; single umbilical artery is associated with renal anomalies
- Liver: palpable 1–2 cm below right costal margin is normal; splenomegaly = consider congenital infection (TORCH)
- Abdominal distension: consider intestinal atresia, Hirschsprung's disease
Hips: Barlow (dislocation provocation) and Ortolani (reduction test) manoeuvres for developmental dysplasia of the hip (DDH); a positive clunk = developmental dysplasia. Risk factors: female sex, first-born, breech presentation, family history.
Spine and genitalia:
- Inspect full length of spine for neural tube defects (spina bifida, meningomyelocele — covered or open lesion)
- Genitalia: note ambiguous genitalia (requires urgent karyotype and endocrinology assessment — do NOT assign sex until evaluated); check for hypospadias, undescended testes, labial fusion
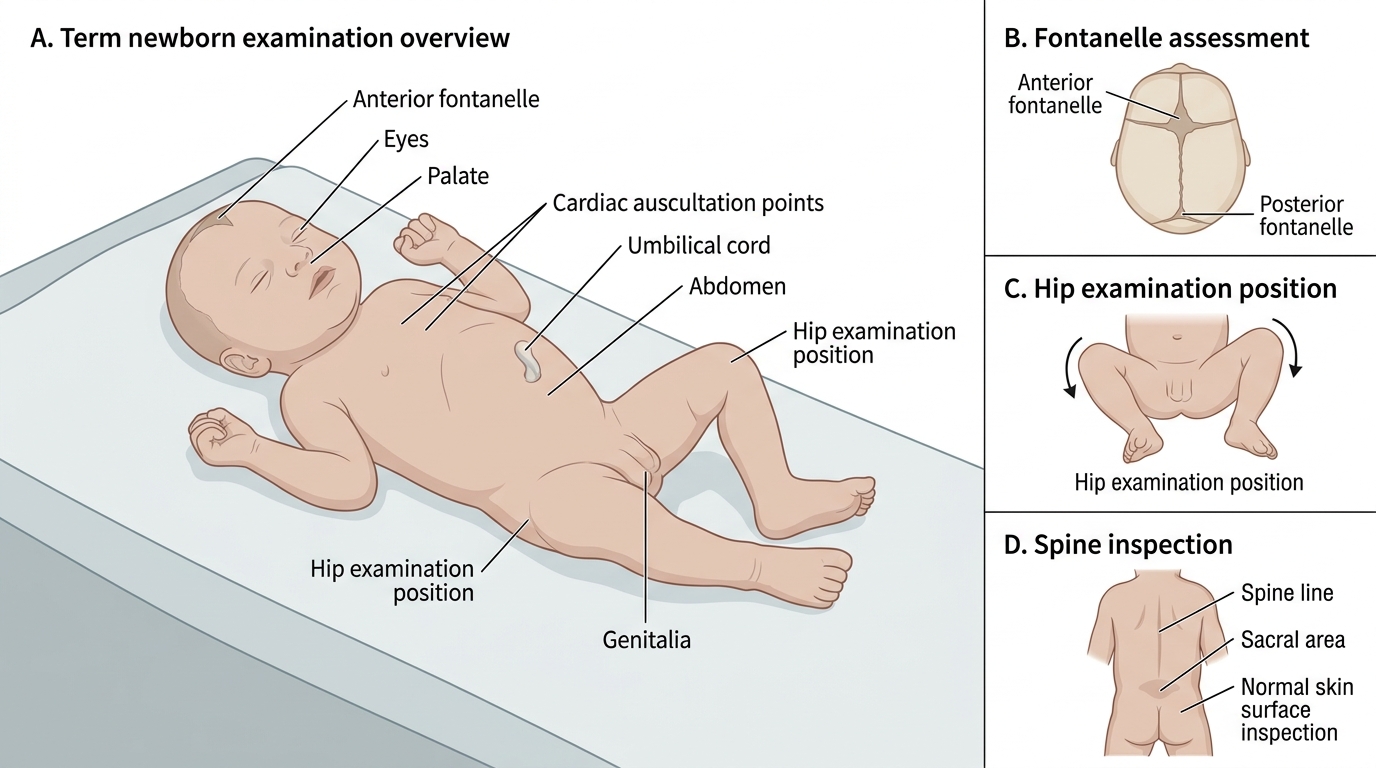
Term Newborn Examination Points
Birth Asphyxia: Definition, Pathophysiology, and Organ Consequences
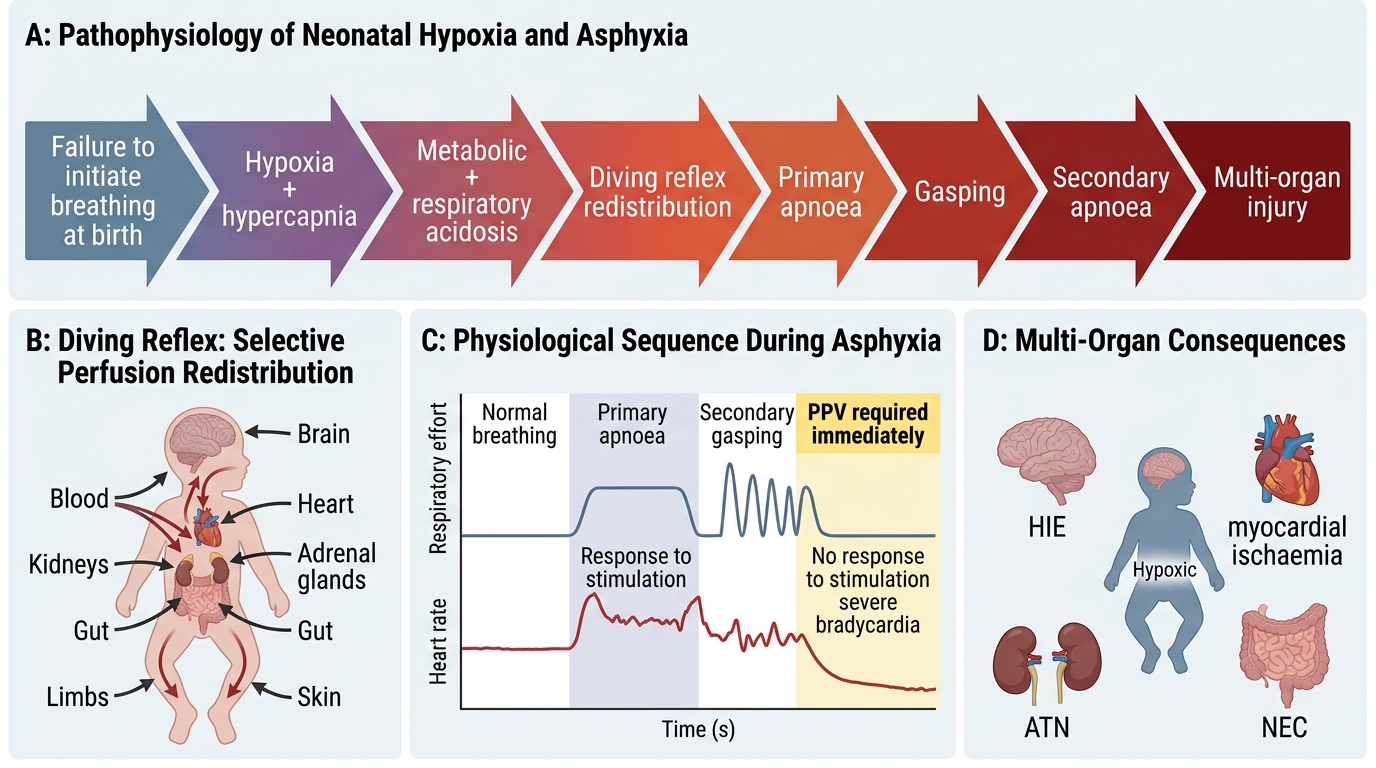
Birth asphyxia is defined as the failure to establish adequate spontaneous respiration at birth, resulting in progressive hypoxia (low oxygen), hypercapnia (elevated CO₂), and metabolic acidosis. It is not synonymous with a low APGAR score — a low APGAR may result from prematurity, maternal sedation, or neuromuscular disease — but it is confirmed biochemically by umbilical cord arterial blood gas values showing pH <7.0 and/or base excess more negative than -12 mmol/L in the context of clinical compromise.
Pathophysiological sequence:
The fetus responds to acute hypoxia with the diving reflex — a redistribution of cardiac output away from peripheral vascular beds (skin, gut, kidneys, skeletal muscle) toward the vital organs (brain, heart, adrenal glands). This protective response buys time but is limited in duration. As hypoxia continues:
Primary apnoea: The neonate initially makes gasping respiratory efforts, then stops breathing. Heart rate falls but remains above 60 bpm. This is primary apnoea — the infant can still be stimulated to breathe (gentle drying, flicking the feet, or tactile stimulation may be sufficient).
Terminal gasping → secondary apnoea: If hypoxia continues beyond primary apnoea, a brief period of irregular gasping occurs, followed by secondary (terminal) apnoea — complete cessation of breathing, progressive bradycardia, and cardiovascular collapse. At this stage, stimulation alone will NOT restart breathing — positive pressure ventilation is required. This is the critical resuscitation threshold.
Multi-organ consequences of birth asphyxia:
- Brain: Hypoxic-Ischaemic Encephalopathy (HIE) — the most feared and clinically prominent consequence; spectrum from mild (hypotonia, poor feeding) to severe (seizures, coma, brain death); classified by Sarnat staging (I–III); may be partially mitigated by therapeutic hypothermia (cooling) if initiated within 6 hours
- Heart: Transient myocardial ischaemia → reduced contractility → poor cardiac output → tricuspid regurgitation in some cases; troponin elevated
- Kidneys: Acute tubular necrosis (ATN) → oliguria/anuria in the first 24–48 h; monitor urine output and creatinine
- Gut: Necrotising enterocolitis (NEC) — ischaemia of the gut mucosa; presents with abdominal distension, bloody stools, and pneumatosis intestinalis on X-ray; risk is highest in preterm asphyxiated neonates
- Metabolic: Hypoglycaemia (depleted glycogen stores), hypocalcaemia, hyponatraemia
- Haematological: Disseminated intravascular coagulation (DIC) in severe cases
Pathophysiology of Birth Asphyxia
SELF-CHECK
A neonate at term fails to breathe at birth. After 60 seconds of drying and stimulation, the baby makes one gasping breath then becomes apnoeic again. Heart rate is 40 bpm and falling. The neonatal team attempts tactile stimulation again — there is no respiratory response. What physiological stage has this infant reached and what is the correct intervention?
A. Primary apnoea — continue tactile stimulation for another 30 seconds
B. Secondary (terminal) apnoea — positive pressure ventilation (PPV) is required immediately
C. Primary apnoea — administer naloxone as maternal opioids are likely the cause
D. Secondary apnoea — intubation with chest compressions only; no ventilation needed at this stage
Reveal Answer
Answer: B. Secondary (terminal) apnoea — positive pressure ventilation (PPV) is required immediately
The sequence (initial gasp → apnoea → no response to stimulation + severe bradycardia) indicates the infant has progressed through primary apnoea to secondary (terminal) apnoea. In secondary apnoea, the brain's respiratory centres are no longer responsive to stimulation — positive pressure ventilation (PPV, via mask and bag or T-piece resuscitator) is the mandatory intervention to restore oxygenation. Tactile stimulation alone is insufficient and wastes critical time. Naloxone is inappropriate here; it reverses opioid-induced respiratory depression but has no role in secondary apnoea from asphyxia. Chest compressions are added only if heart rate remains <60 bpm after 30 seconds of effective ventilation.
Risk Factors and Prevention of Birth Asphyxia
Birth asphyxia is not always preventable, but a significant proportion of cases are attributable to identifiable risk factors that can be anticipated and managed. Preparedness — having a trained neonatal resuscitation team present at deliveries with known high risk — reduces the time from birth to effective intervention and improves outcomes.
Antenatal risk factors:
Maternal factors: pre-eclampsia and hypertensive disorders (uteroplacental insufficiency → chronic fetal hypoxia), diabetes mellitus (macrosomia → birth trauma; metabolic derangements), anaemia (reduced oxygen delivery), antepartum haemorrhage (abruption → acute placental insufficiency), maternal infection (chorioamnionitis), post-term pregnancy (ageing placenta → reduced reserve).
Fetal factors: intrauterine growth restriction (IUGR) with abnormal Doppler flow (absent/reversed end-diastolic flow = severely compromised placenta); multiple pregnancy; prematurity; congenital anomalies; hydrops fetalis.
Intrapartum risk factors (these cause ACUTE asphyxia at the time of delivery and must be anticipated by the obstetric team):
- Umbilical cord prolapse: cord compression = acute fetal hypoxia; requires emergency delivery within minutes
- Shoulder dystocia: prolonged delivery of the shoulders = cord compression + trunk compression
- Prolonged second stage: fetal head compression → progressive venous congestion → hypoxia
- Thick meconium-stained amniotic fluid (MSAF): marker of fetal distress; risk of meconium aspiration syndrome
- Uterine rupture: acute placental separation + blood loss
- Placental abruption: acute disruption of gas exchange
- Abnormal CTG patterns: type II decelerations, prolonged decelerations, reduced variability with decelerations
- Difficult instrumental delivery (forceps, vacuum)
Preparedness at delivery:
All deliveries with identified antenatal risk should be attended by a neonatal team capable of resuscitation. The resuscitation trolley (radiant warmer, bag-mask, suction, oxygen, intubation equipment, medications) must be checked and ready before the delivery. The APGAR assessment begins at 1 minute of life — the resuscitation decision must be made before the 1-minute APGAR is formally recorded.