Page 24 of 32
OG19.{2,4} | Postpartum Contraception Counselling and PPIUCD — SDL Guide
Learning Objectives
- Explain the clinical urgency of postpartum contraception counselling using the WHO inter-pregnancy interval evidence
- Apply the WHO Medical Eligibility Criteria (MEC) categories 1-4 to select appropriate contraceptive methods for breastfeeding and non-breastfeeding postpartum women
- Describe the PPIUCD programme: eligibility, timing windows (immediate vs delayed), contraindications, and expulsion rates
- Enumerate the three criteria for the Lactational Amenorrhoea Method (LAM) and explain when LAM is no longer reliable
- Counsel a simulated patient on postpartum contraceptive options, addressing breastfeeding concerns, myths, and method preference
- Describe the indications, timing, and consent requirements for puerperal sterilisation
INSTRUCTIONS
Postpartum contraception is a critical component of postnatal care — yet in India, approximately 48% of women leave the maternity facility without a contraceptive method. The puerperium is a unique opportunity to provide highly effective contraception at a moment when women are motivated, in contact with the health system, and beginning breastfeeding. This module follows the OG-skills arc to move you from the clinical rationale through the governing principles (WHO MEC), to the techniques of PPIUCD insertion and structured counselling. Competency OG19.2 focuses on counselling skill in a simulated environment; OG19.4 focuses on knowledge of the PPIUCD programme.
References
- WHO Medical Eligibility Criteria for Contraceptive Use, 5th Edition, 2015 (guideline)
- Ministry of Health & Family Welfare, India — PPIUCD Training and Service Delivery Guidelines, 2010 (updated 2013) (guideline)
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch. 31 — Family Planning (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., Ch. 20 — Contraception (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old multipara delivers her third child by normal vaginal delivery. She is breastfeeding, looking healthy, and planning to go home tomorrow. As you conduct the discharge examination, she says: 'Doctor, my husband wants more children soon, but I am not sure I am ready. What can I do — I am feeding the baby so I thought I was safe?' You have this one conversation before she leaves. What will you tell her, and what will you offer her before she walks out the door?
WHY THIS MATTERS
Unintended pregnancy is among the most preventable contributors to maternal and neonatal morbidity in low- and middle-income countries. The WHO recommends an inter-pregnancy interval of at least 24 months from delivery to next conception to reduce the risks of preterm birth, low birth weight, maternal anaemia, and uterine rupture (in women with a previous caesarean section). In India, a significant proportion of pregnancies are closely spaced — the National Family Health Survey (NFHS-5, 2019-21) found that 27% of births occurred within 24 months of a preceding birth. The postpartum contact — whether within 48 hours at the maternity facility or at the 6-week postnatal check — is the highest-yield opportunity to provide contraception because the woman is already in the health system, motivated, and her fertility intentions are immediately relevant. Missing this window often means the next pregnancy has already begun before the next routine health contact. As the doctor who conducts postnatal discharge counselling, you are the key person in this equation.
RECALL
Test your baseline before we begin. From your pharmacology and physiology modules: (1) Why is oestrogen contraindicated in the early postpartum period in breastfeeding women — what physiological mechanism explains this? (2) What are the three mechanisms of action of the copper IUCD? (3) What is the prolactin-ovulation relationship — why does breastfeeding suppress (but not reliably prevent) ovulation? Write brief answers — the physiology directly explains the WHO MEC categories we will apply.
Why Postpartum Contraception Cannot Wait: Clinical Indication and the Inter-Pregnancy Interval
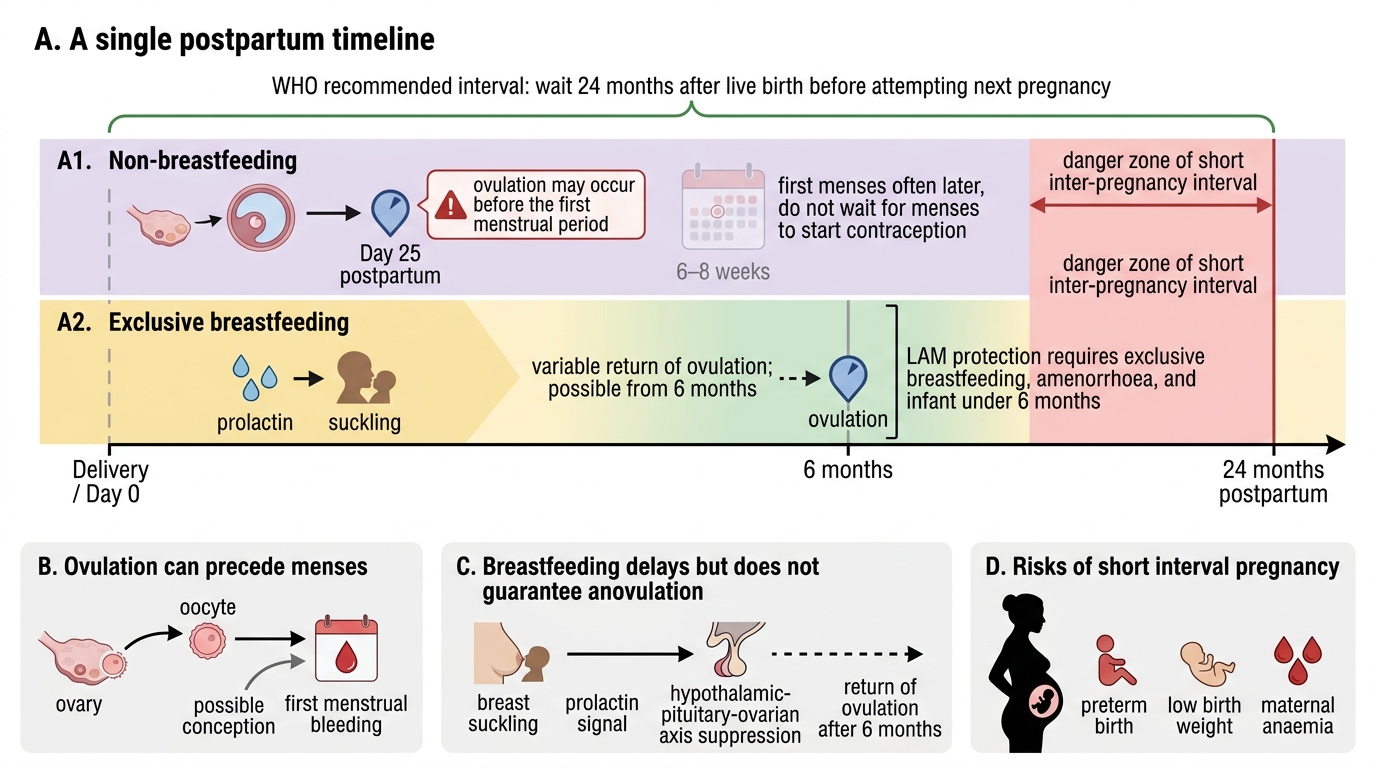
The fundamental clinical problem in postpartum contraception is the mismatch between women's assumptions about their fertility and the biological reality. The commonest assumption — illustrated in the hook — is that breastfeeding provides reliable contraception. It does not, unless three specific criteria are met (covered in the LAM section below). The biological reality is stark: in non-breastfeeding women, ovulation can return as early as 25 days postpartum, with the majority ovulating by 6-8 weeks. Even in exclusively breastfeeding women, ovulation can resume from 6 months onwards, and breakthrough ovulation without any preceding menstruation is biologically possible. A woman can therefore conceive before her first postpartum period — before she or her family realises her fertility has returned. This is not a rare event — it is the mechanism behind the high proportion of short-interval pregnancies in populations without postpartum contraception access.
The evidence base for the 24-month inter-pregnancy interval (IPI) comes from large population-based studies demonstrating a J-shaped relationship between IPI and perinatal outcomes. An IPI of less than 18 months doubles the risk of preterm birth and is associated with a 1.6-fold increase in low birth weight. The mechanisms include: incomplete uterine scar healing (relevant for C-section deliveries), maternal nutritional depletion (particularly folate and iron), and incomplete cervical remodelling. For the mother, short IPI is associated with increased anaemia, pregnancy complications, and — in C-section deliveries — uterine rupture. India's family planning programmes have therefore made postpartum family planning (PPFP) a national priority, with the PPIUCD programme as its flagship intervention.
Return of Ovulation and Inter-Pregnancy Interval After Delivery
SELF-CHECK
A non-breastfeeding woman asks when she could become pregnant again after delivery. The correct answer, based on biological evidence, is:
A. Not until her first menstrual period returns, at approximately 6-8 weeks
B. As early as 25 days postpartum, since ovulation can precede the first menstrual period
C. Only after 6 months, as the uterus takes that long to return to its pre-pregnant state
D. She is protected for 3 months due to elevated prolactin from delivery
Reveal Answer
Answer: B. As early as 25 days postpartum, since ovulation can precede the first menstrual period
Ovulation can return as early as 25 days postpartum in non-breastfeeding women — before the first menstrual period. A woman can therefore conceive without ever having a postpartum period. Waiting for the first period before initiating contraception is clinically incorrect advice. Prolactin elevation from delivery alone (without suckling) does not reliably suppress ovulation.
Anatomy, Physiology and Governing Principles of Postpartum Contraception Eligibility
The framework governing all postpartum contraceptive decisions is the WHO Medical Eligibility Criteria for Contraceptive Use (WHO MEC), currently in its 5th edition (2015). Published by the World Health Organization and updated periodically based on systematic reviews of the evidence, the MEC provides a globally standardised reference for matching contraceptive methods to women's clinical circumstances. It eliminates the guesswork that previously led to over-restriction (denying safe methods) and under-restriction (prescribing unsafe ones) and is the definitive reference used by India's national family planning programme, the FOGSI guidelines, and the NMC curriculum. Every clinician providing family planning services must be fluent in applying MEC categories to common postpartum scenarios — it is not sufficient to know 'what methods exist'; you must know which are eligible, contraindicated, and preferred for the woman in front of you. The MEC assigns each contraceptive method a category rating (1-4) for each medical condition or circumstance:
- Category 1: No restriction — method can be used freely.
- Category 2: Advantages generally outweigh theoretical or proven risks — method can generally be used.
- Category 3: Theoretical or proven risks generally outweigh the advantages — method use requires careful clinical judgement; alternatives preferred.
- Category 4: Absolute contraindication — method must not be used.
For postpartum contraception, the two most clinically significant eligibility conditions are breastfeeding status and time since delivery. The physiological basis for these distinctions is important to understand, not merely memorise. Oestrogen in combined hormonal contraceptives (COC) suppresses prolactin secretion and reduces the volume and fat content of breast milk, posing a direct nutritional risk to the breastfed infant. This is why COCs carry WHO MEC category 4 (absolute contraindication) in breastfeeding women <6 weeks postpartum, when the infant's nutritional dependence on breast milk is highest and the breastfeeding relationship is most vulnerable. As the infant matures and begins complementary feeds (and maternal prolactin levels stabilise), this risk diminishes — hence the category 3 rating from 6 weeks to 6 months, and category 2 after 6 months of breastfeeding. This graduated eligibility directly reflects the biology of lactation physiology.
Progestogens (in POPs and DMPA) do not suppress lactation and are classified WHO MEC category 1 or 2 for breastfeeding women from 6 weeks. Before 6 weeks, there is a theoretical concern about neonatal exposure to progestogens via breast milk (the neonatal liver's enzyme systems are immature), which places these methods at category 2 (advantages generally outweigh risks) in the 0-6-week window — meaning they CAN be used if other options are unavailable or unacceptable.
Anatomical principle for PPIUCD: In the postpartum uterus, the fundus is high, the uterine walls are soft and thick, and the os is open — making IUCD insertion technically feasible. The critical anatomical challenge is correct fundal placement: the device must sit in the uterine fundus, above the internal os, not in the lower uterine segment (which leads to expulsion). The postpartum uterine cavity is large, and standard inserters are inadequate — PPIUCD requires a specifically designed longer inserter or ring forceps placement for post-placental insertion.
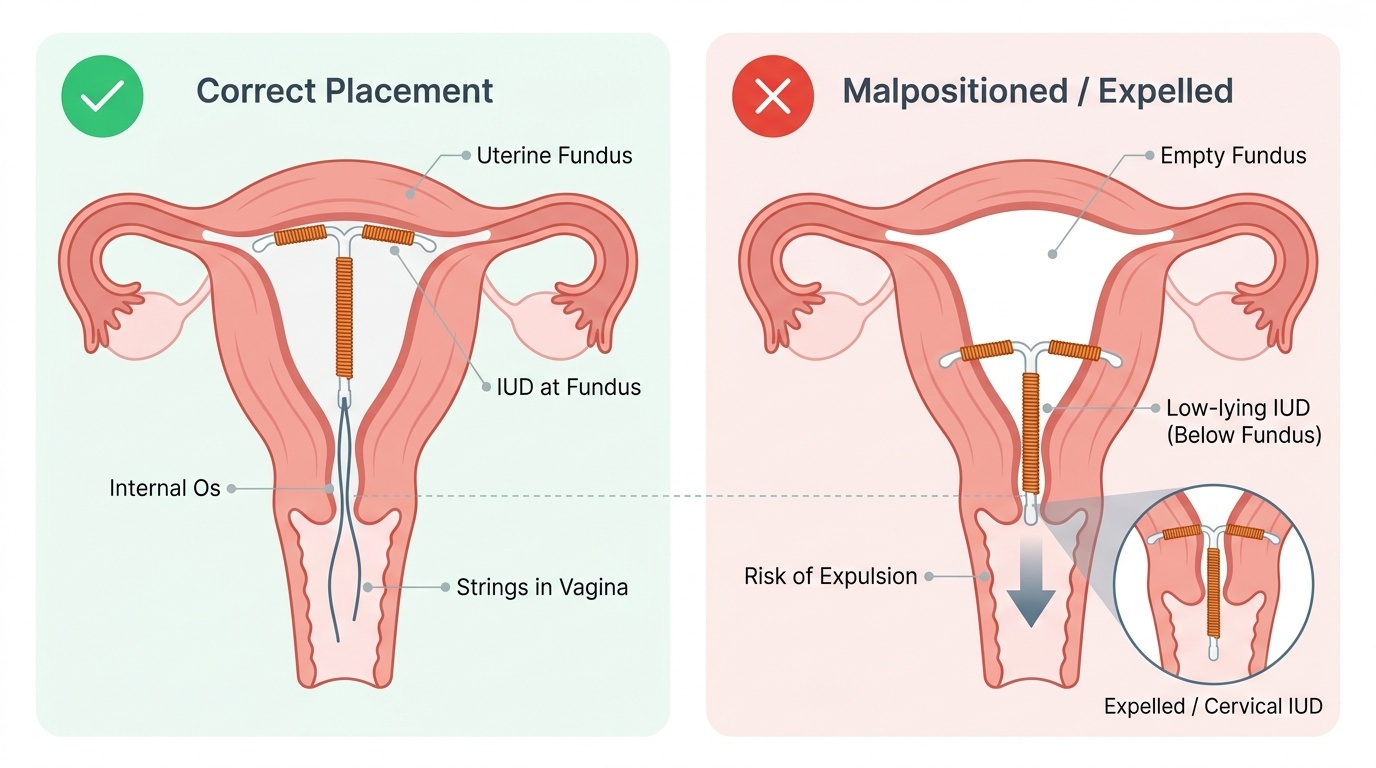
Provided image
PPIUCD Programme: Technique, Timing and Eligibility
The PPIUCD (Postpartum Intrauterine Contraceptive Device) programme was launched by the Government of India's Ministry of Health & Family Welfare as a national initiative to increase postpartum family planning uptake at the facility level. It offers a highly effective (>99%), long-acting reversible contraceptive that can be inserted at the time of delivery, integrating family planning into the obstetric episode without requiring a separate visit. The copper CuT 380A is the standard PPIUCD used in India; it provides protection for 10 years and is fully reversible. Two insertion timing windows exist, with a critical gap between them that must be avoided:
Immediate (post-placental) insertion: within 10 minutes of placental delivery. This is the technically easiest window — the uterus is large, the os is open, and the operator can directly visualise the uterine cavity. Insertion is performed using a specially designed long-handle ring forceps ('Kelly's forceps') placed to deliver the IUCD to the fundus under direct vision or following the inserter tube. The device strings are left long (to be trimmed at the 6-week check). Expulsion rates for immediate post-placental insertion are approximately 10-15% — higher than interval insertion, but the method is still cost-effective because the woman leaves the facility already protected.
Early postpartum: within 48 hours of delivery. The uterus remains large enough for placement before rapid involution begins. Expulsion rates are similar to immediate insertion.
AVOID the 48-hour to 6-week gap: During this period, uterine involution makes placement technically difficult and increases risk of perforation and expulsion significantly. This window is not recommended.
Delayed (interval) insertion: from 6 weeks onwards (after uterine involution is complete). At this point, insertion technique is similar to an interval IUCD insertion. Expulsion rates are lower (~5%).
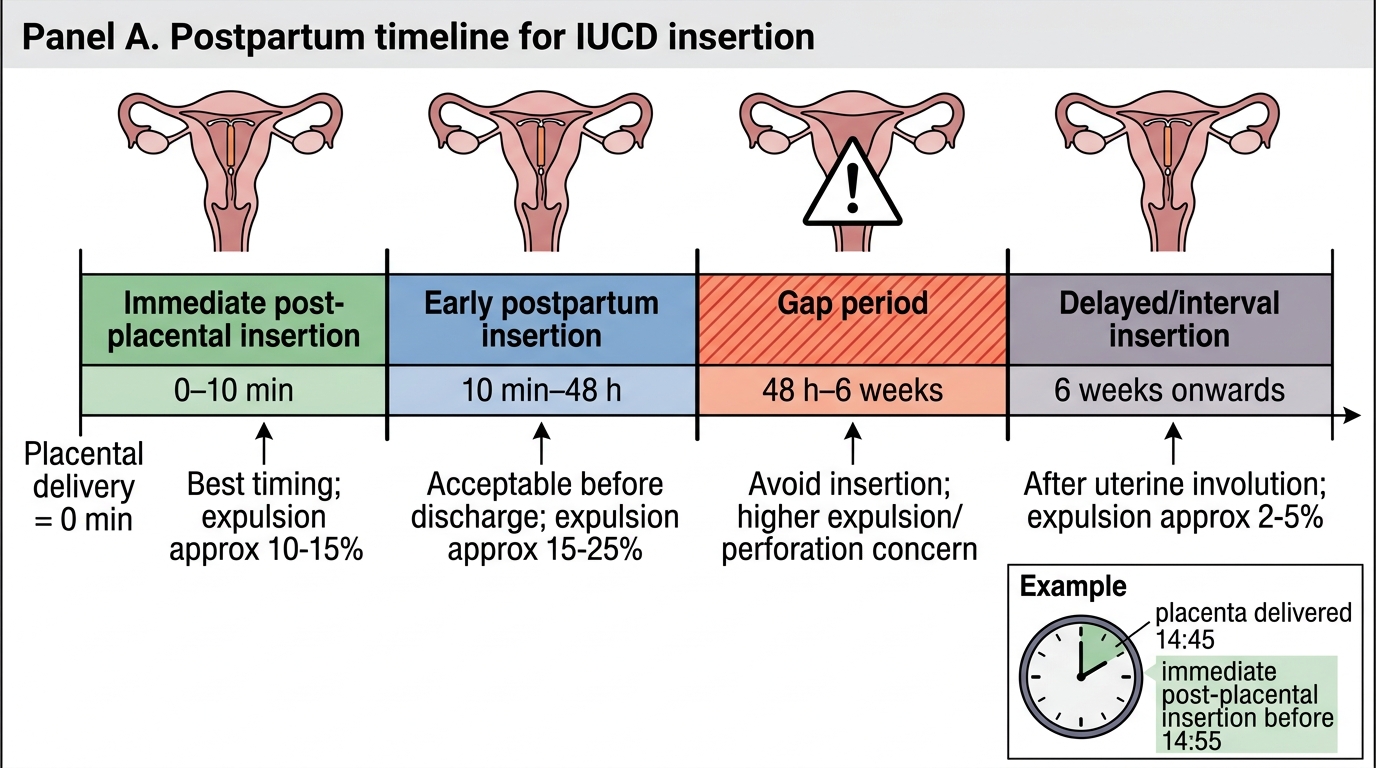
PPIUCD Insertion Timing Windows
Eligibility and contraindications for PPIUCD:
- Eligible: all consenting women delivering vaginally or by C-section without the following contraindications.
- Contraindications: Prolonged PROM (>18 hours, due to chorioamnionitis risk), fever in labour, chorioamnionitis, PPH with uncontrolled bleeding, known uterine anomaly (septate uterus, fibroids distorting cavity), known STI at time of insertion, immunocompromised states (relative).
Counselling for PPIUCD: Women must be counselled on: (1) the increased expulsion rate vs interval insertion, (2) the need to check strings at 6-week visit, (3) full reversibility, and (4) no effect on breastfeeding (copper IUCD is WHO MEC category 1 for breastfeeding at all postpartum times).
SELF-CHECK
A woman delivers at 14:30 h. The placenta is delivered at 14:45 h. She consents to PPIUCD. According to the 'immediate post-placental' definition, insertion should occur:
A. Any time in the first 24 hours after delivery
B. Within 10 minutes of placental delivery — i.e., before 14:55 h
C. Within 48 hours, after the woman has rested and been counselled
D. Only at the 6-week postnatal check to ensure full involution
Reveal Answer
Answer: B. Within 10 minutes of placental delivery — i.e., before 14:55 h
Immediate post-placental PPIUCD insertion is defined as within 10 minutes of placental delivery — in this case before 14:55 h. After this window, the early postpartum window (up to 48 hours) is still acceptable. The 48h-6 week gap must be avoided due to involution-related perforation and expulsion risk. The 6-week visit is the delayed/interval insertion window with the lowest expulsion rate.