Page 25 of 32
OG19.{2,4} | Postpartum Contraception Counselling and PPIUCD — SDL Guide (Part 2)
LAM, Hormonal Methods and Barrier Contraception in the Puerperium
Beyond the PPIUCD, a spectrum of contraceptive methods is available in the puerperium, each with specific eligibility based on breastfeeding status, timing, and medical conditions. Understanding the evidence base and the WHO MEC classifications allows you to guide women to the best match for their circumstances — this is the counselling skill that OG19.2 requires. Each method discussed below has a distinct mechanism of action, eligibility profile, and practical consideration. The clinical decision is never simply 'what is available' but 'what is eligible, acceptable, and sustained for this woman given her breastfeeding status, timing postpartum, and life circumstances.' Mastering the profile of each method — including its WHO MEC category in breastfeeding women — is the foundation on which the counselling consultation is built.
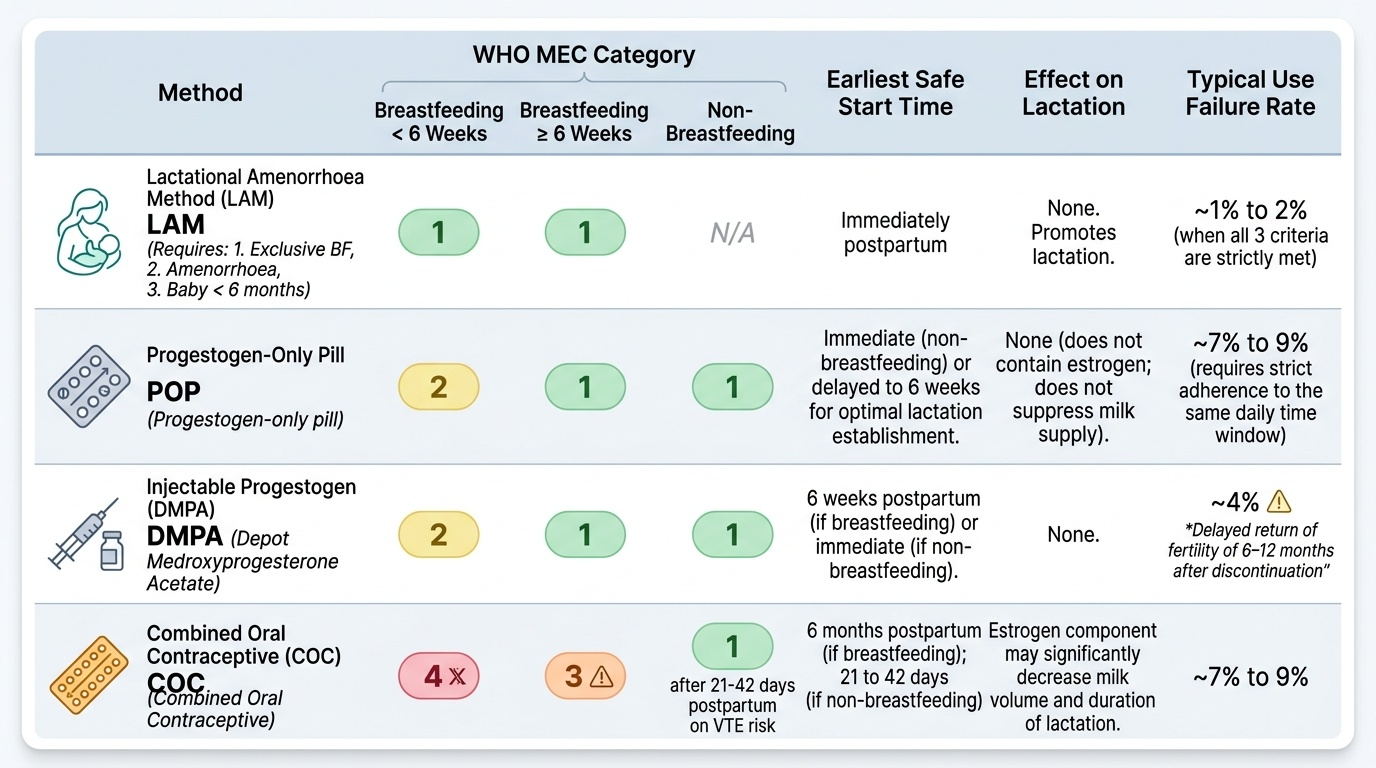
Lactational Amenorrhoea Method (LAM) is a naturally occurring temporary contraceptive method based on the principle that prolactin-driven suppression of GnRH (and consequently LH/FSH and ovulation) provides protection against pregnancy during exclusive breastfeeding. However, LAM is only effective when ALL THREE of the following criteria are simultaneously met:
1. Exclusively (or nearly exclusively) breastfeeding — the infant receives breast milk as the only food, fed on demand including at night.
2. Amenorrhoea — the woman has had no vaginal bleeding after 56 days (8 weeks) postpartum.
3. Baby is less than 6 months old.
When all three criteria are met, LAM provides approximately 98-99.5% protection against pregnancy. As soon as any ONE criterion fails — the baby starts complementary feeds, the woman's period returns, or the baby turns 6 months — LAM is no longer reliable and another method must be initiated immediately.
Progestogen-only pill (POP): Does not contain oestrogen and therefore does not suppress lactation. WHO MEC category 2 for breastfeeding women <6 weeks, category 1 from 6 weeks. Requires strict timing adherence.
Injectable progestogen — DMPA: 150 mg IM every 3 months. WHO MEC category 2 for breastfeeding women <6 weeks, category 1 from 6 weeks. Highly effective (>99%). Delayed return of fertility (6-12 months after stopping) — must be counselled.
Combined Oral Contraceptive (COC): WHO MEC category 4 (do not use) in breastfeeding <6 weeks — oestrogen suppresses prolactin and reduces milk volume/quality at the most critical period of breastfeeding establishment. Category 3 from 6 weeks to 6 months breastfeeding. Category 2 if non-breastfeeding (can start from 3 weeks postpartum) or after 6 months breastfeeding.
Barrier methods: Male condoms (MEC category 1 always), female condoms — safe, immediately usable, STI protection.
Puerperal sterilisation: Female sterilisation within 7 days of delivery by minilaparotomy (subumbilical incision, accessible because uterus is still enlarged). After 6 weeks, laparoscopic sterilisation. Key counselling: permanent — adequate pre-procedure counselling ideally beginning antenatally, written informed consent mandatory, higher regret rates in young women.
Provided image
SELF-CHECK
A breastfeeding woman at 4 weeks postpartum requests oral contraception. She is amenorrhoeic, exclusively breastfeeding, and her baby is 4 weeks old. Which is the MOST appropriate oral contraceptive recommendation?
A. Start a combined oral contraceptive (COC) — she is breastfeeding so oestrogen will not cause harm
B. No contraception needed — she is fully protected by LAM for 6 months
C. Start a progestogen-only pill (POP) — WHO MEC category 2 at <6 weeks, does not suppress lactation
D. She must wait until 6 months postpartum before any hormonal method
Reveal Answer
Answer: C. Start a progestogen-only pill (POP) — WHO MEC category 2 at <6 weeks, does not suppress lactation
COC is WHO MEC category 4 (absolute contraindication) in breastfeeding <6 weeks — it suppresses prolactin and reduces milk volume/quality. LAM alone would be valid since all 3 criteria are met, but she specifically requests oral contraception. POP is WHO MEC category 2 at <6 weeks (advantages outweigh theoretical risks) and does not suppress lactation — it is the correct choice. Waiting until 6 months is incorrect; POPs are usable from delivery.
Eligibility Assessment: Applying WHO MEC to the Individual Patient
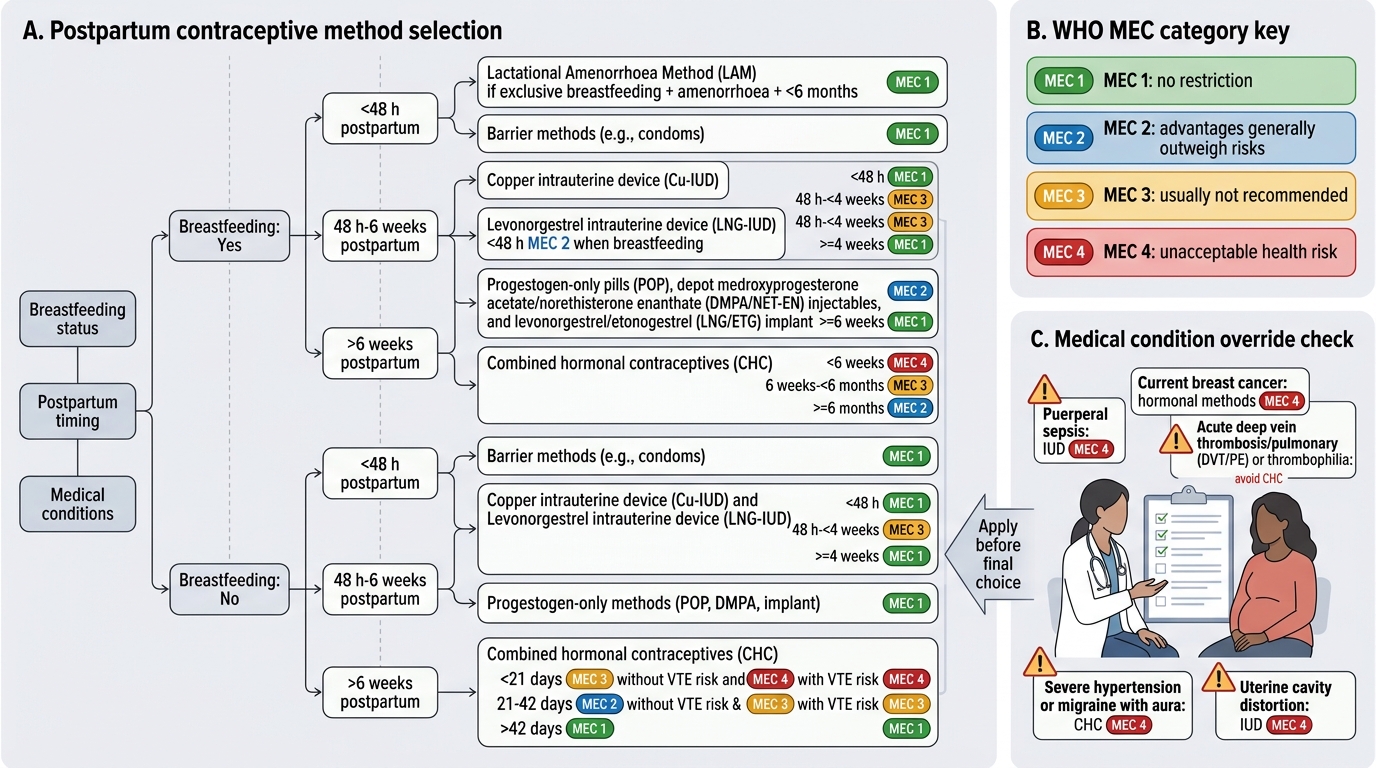
The skill of postpartum contraceptive counselling is not memorising a table — it is translating the WHO MEC framework into an individualised recommendation for the woman in front of you. This requires four clinical inputs: (1) breastfeeding status, (2) time since delivery, (3) relevant medical conditions, and (4) the woman's expressed preferences and concerns. Applying these inputs systematically prevents the most common clinical errors — particularly the prescription of COC to a breastfeeding woman in the first six weeks. The structured approach also ensures you never offer a method the woman cannot use safely, while still honouring her preferences from among the eligible options. The scenarios below represent the most common clinical situations you will encounter on the postnatal ward and at the six-week check; work through each scenario mentally before reading the eligible methods listed, then verify your reasoning against the WHO MEC categories you have studied.
For a breastfeeding woman at <48 hours postpartum, the method hierarchy by evidence and eligibility is:
- First choice LARC: PPIUCD (copper, MEC 1) — offer at delivery or within 48 hours.
- Progestogen-only: DMPA (MEC 2) or POP (MEC 2) — safe if PPIUCD declined.
- Condoms: MEC 1 — always an option, provide STI protection.
- LAM: Valid if all three criteria met — counsel on strict criteria and transition plan.
- COC: Category 4 — do not offer under any circumstances.
For a breastfeeding woman at 6 weeks postnatal check:
- LARC: IUCD or implant (MEC 1).
- Progestogen: DMPA or POP (MEC 1 from 6 weeks).
- COC: Still MEC 3 (not freely recommended) until 6 months breastfeeding — advise alternatives unless no other method is acceptable.
- LAM: Remains valid if baby <6 months, amenorrhoeic, exclusively breastfeeding — but counsel that this window is closing.
For a non-breastfeeding woman: all methods are eligible. COC can start from 3 weeks postpartum (MEC 2 — slight VTE risk in the first 3 weeks). Progestogens from day 1 postpartum.
Special medical conditions: History of VTE (avoid COC — oestrogen increases thrombosis risk); migraine with aura (COC category 4 — stroke risk); hypertension (COC category 3-4 depending on severity); HIV on antiretrovirals (check for drug interactions — some ARTs reduce COC efficacy).
Postpartum Contraceptive Method Selection by WHO MEC
Counselling Practice: Simulated Consultation for Postpartum Contraception
The competency OG19.2 requires that you counsel a patient in a simulated environment — which means the assessor is not evaluating your factual recall but your ability to conduct a structured, patient-centred consultation that produces an appropriate contraceptive plan. This is a learned clinical skill with distinct components that require deliberate practice, not merely studying the WHO MEC table. Research on communication skills in family planning consistently shows that non-directive, patient-centred counselling produces higher rates of method adoption and continuation than prescriptive approaches where the provider selects the method. The woman's informed choice — supported by accurate information and a compassionate, non-judgemental consultation — is the ethical and practical goal. In the Indian context, cultural factors (husband or family involvement in decision-making, myths about contraceptive harms, concerns about breastfeeding) make structured communication skills even more important, since factual knowledge alone is insufficient to navigate these conversations effectively. The internationally recognised GATHER framework provides a simple, reproducible scaffold for the postpartum contraception consultation:
- Greet — warmly, establish rapport, confirm name and parity, acknowledge the new baby.
- Ask — reproductive intentions (more children? how soon?), breastfeeding status, medical problems, prior contraceptive experience, partner situation, concerns or preferences.
- Tell — present the range of available methods appropriate for her eligibility profile, in plain language, without bias toward any particular method.
- Help — support her to choose by discussing preferences (duration, convenience, reversibility, side effects) within the eligible options.
- Explain — the chosen method in detail: how it works, how to use it, expected side effects, warning signs requiring review, follow-up date.
- Return — a specific follow-up appointment and information about emergency contraception if needed.
Common myths and objections, with evidence-based responses:
- 'The IUD will move and harm my baby / enter my womb.' — The IUCD is placed inside the uterus; it cannot reach the baby and is a safe, well-established method.
- 'Injections make you permanently infertile.' — DMPA delays return of fertility (6-12 months) but does NOT cause permanent infertility.
- 'I cannot use contraception while breastfeeding.' — Copper IUCD, POP, and DMPA are all safe for breastfeeding; COC is the exception in early breastfeeding.
- 'My husband decides these things.' — Acknowledge family context while affirming the woman's right to informed consent; involve the partner if the woman wishes.
- 'I will just breastfeed — that is enough protection.' — Explain LAM: works only when all three criteria are simultaneously met and only up to 6 months.
In simulation, you will be assessed on: use of clear non-medical language; non-directive approach; accurate WHO MEC application; addressing at least one concern or myth; and providing a follow-up plan.
CLINICAL PEARL
The single most common and consequential error in postpartum contraception practice is prescribing or recommending a COC to a breastfeeding woman in the first 6 weeks. This is WHO MEC category 4 — an absolute contraindication — because oestrogen suppresses prolactin and reduces breast milk volume at the most vulnerable phase of breastfeeding establishment. When a woman requests 'the pill,' always clarify: combined pill (COC) or progestogen-only pill (POP)? The POP is safe in breastfeeding (MEC 2 at <6 weeks, MEC 1 from 6 weeks) and is a valid choice. This COC/POP distinction is among the most consistently tested questions in MBBS final examinations and postgraduate entrance assessments.