Page 26 of 32
OG19.{2,4} | Postpartum Contraception Counselling and PPIUCD — SDL Guide (Part 3)
Self-Assessment: Contraception Eligibility and Counselling
You have now completed the full OG-skills arc for postpartum contraception — from the clinical urgency and the inter-pregnancy interval evidence, through the WHO MEC framework, the anatomy governing PPIUCD insertion, the method comparison, the eligibility decision algorithm, and the GATHER counselling structure. This self-assessment block uses active recall to verify your readiness for simulation and written assessment. Retrieval practice strengthens memory consolidation more than passive re-reading — work through each question from memory, note any gaps honestly, and return to the relevant section before your skill station or examination. These questions are drawn from the most commonly tested aspects of postpartum contraception in MBBS final examinations, clinical OSCEs, and postgraduate entrance assessments — they are not exhaustive but they cover the highest-yield distinctions. A confident, unprompted answer to each confirms you have integrated the material at the level of application rather than mere recognition.
Questions for active self-testing:
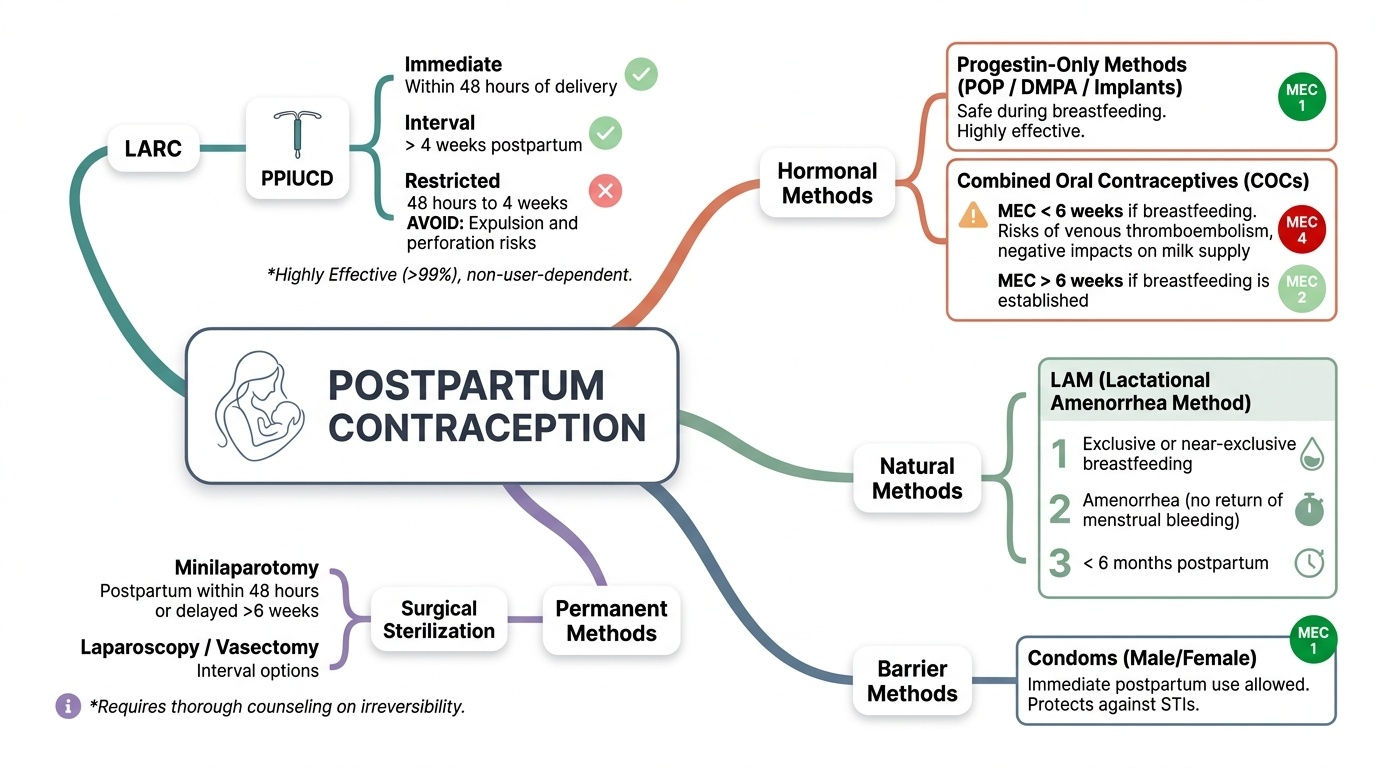
- Urgency: How early can ovulation return in a non-breastfeeding woman? What is the WHO-recommended inter-pregnancy interval and why is short IPI harmful?
- WHO MEC: State the MEC category for COC in a breastfeeding woman at 4 weeks postpartum. At 8 weeks breastfeeding? At 7 months breastfeeding? Give the physiological reason for each change.
- LAM: State the three LAM criteria precisely. A woman is exclusively breastfeeding her 5-month-old but her period just returned — is LAM still effective?
- PPIUCD: Name the two recommended insertion windows and the one window to avoid. What are three absolute contraindications to PPIUCD?
- Non-breastfeeding COC: From what postpartum time can a non-breastfeeding woman safely start COC?
- Sterilisation: What is the surgical approach for puerperal sterilisation within 7 days of delivery? When should counselling for sterilisation ideally begin?
Provided image
SELF-CHECK
According to WHO MEC, which statement about postpartum contraception is CORRECT?
A. DMPA is absolutely contraindicated in breastfeeding women at all times postpartum
B. Copper IUCD is WHO MEC category 1 for breastfeeding women at all postpartum time points
C. COC becomes safely usable (MEC 2) from 6 weeks postpartum in all breastfeeding women
D. LAM provides 98% protection for up to 12 months as long as the woman continues breastfeeding
Reveal Answer
Answer: B. Copper IUCD is WHO MEC category 1 for breastfeeding women at all postpartum time points
Copper IUCD (including PPIUCD) has no hormonal component and is WHO MEC category 1 for breastfeeding women at all postpartum times. DMPA is MEC 2 (not absolutely contraindicated) in early breastfeeding <6 weeks. COC at 6 weeks is still MEC 3 (not freely safe) in breastfeeding women until 6 months. LAM is only valid for a maximum of 6 months — the baby <6 months criterion is one of three required conditions.