Page 21 of 28
OG22.2 | Common Vaginal Discharge Syndromes — SDL Guide
Learning Objectives
- Describe the aetiology, clinical features, and pathophysiology of bacterial vaginosis, vulvovaginal candidiasis, and trichomoniasis
- Apply Amsel's criteria and interpret the Nugent score for diagnosis of bacterial vaginosis
- Interpret wet mount microscopy findings for each of the three vaginal discharge syndromes
- Describe the specific management (drug, dose, duration, partner treatment) for each syndrome
- Apply the syndromic management algorithm for vaginal discharge in a primary care setting without microscopy
- Provide evidence-based genital hygiene advice to women with vaginal discharge
INSTRUCTIONS
Vaginal discharge syndromes are among the most common conditions managed in outpatient gynaecology, antenatal care, and primary healthcare settings. This SDL covers the three principal causative syndromes — bacterial vaginosis, vulvovaginal candidiasis, and trichomoniasis — from clinical presentation through to treatment. It builds directly on the physiological discharge module; ensure you have completed that SDL before beginning this one. Work through each section in order, attempting every micro-quiz before reading the explanation.
References
- DC Dutta's Textbook of Gynecology, 8th ed., Ch. 24 (Vaginal Discharge) (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 18 (textbook)
- WHO Guidelines for the Management of Sexually Transmitted Infections, 2016 (guideline)
- NRHM/MoHFW India — Syndromic Management of STI/RTI Guidelines (guideline)
- Amsel R et al. Nonspecific vaginitis: diagnostic criteria and microbial and epidemiologic associations. Am J Med 1983;74(1):14–22 (journal)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three women attend the gynaecology outpatient department on the same afternoon. The first, a 26-year-old teacher, reports a thin greyish discharge with an unpleasant 'fishy' smell that worsens after intercourse. The second, a 24-year-old student recently completing a course of amoxicillin, has intense vulval itching and a thick white 'cottage cheese' discharge. The third, a 32-year-old married woman, presents with a profuse yellow-green frothy discharge with vulval soreness, and her husband has recently been treated for a urethral discharge. Vaginal pH in the three women is 5.1, 4.1, and 5.4 respectively. All three have 'discharge' — but each requires a completely different diagnosis and treatment. How do you tell them apart?
WHY THIS MATTERS
Vaginal discharge syndromes are the most common reproductive tract infection presentations encountered by primary care physicians, gynaecologists, and antenatal care providers in India. Bacterial vaginosis, candidiasis, and trichomoniasis together account for the vast majority of symptomatic vaginal discharge in women of reproductive age. Getting the diagnosis right matters beyond symptom relief: bacterial vaginosis in pregnancy is associated with preterm labour and premature rupture of membranes; trichomoniasis facilitates HIV transmission and requires simultaneous partner treatment to prevent reinfection; inappropriate empiric antifungal prescribing for non-fungal discharge drives resistance and delays appropriate treatment. This SDL prepares you to diagnose these three syndromes confidently in both resource-rich settings (with microscopy and culture) and resource-limited settings (syndromic management), in line with WHO and NRHM guidelines.
RECALL
Before beginning, recall from the physiological discharge SDL: (1) Normal vaginal pH is 3.8–4.5, maintained by lactic acid from Lactobacillus species. (2) Lactobacilli dominate the healthy vaginal microbiome; their depletion opens the ecological niche for pathogens. (3) Candidal vaginitis does NOT raise vaginal pH — pH remains ≤4.5. (4) BV and trichomoniasis raise vaginal pH >4.5 through amine production and protozoal metabolism respectively. (5) Post-antibiotic candidiasis occurs because antibiotics deplete Lactobacillus. Also recall: metronidazole is a nitroimidazole that kills anaerobes and protozoa by forming toxic radicals via bacterial nitroreductase; fluconazole is a triazole antifungal that inhibits fungal ergosterol synthesis.
Clinical Presentation: Recognising Abnormal Discharge
The clinical presentation of the three principal vaginal discharge syndromes is sufficiently distinctive that an experienced clinician can make a working diagnosis from history and examination findings alone — which is the basis of the syndromic management approach. Each syndrome has a characteristic combination of discharge appearance, odour, associated symptoms, and vaginal pH that together form a recognisable clinical pattern. Understanding these patterns is the entry point into rational diagnosis and management.
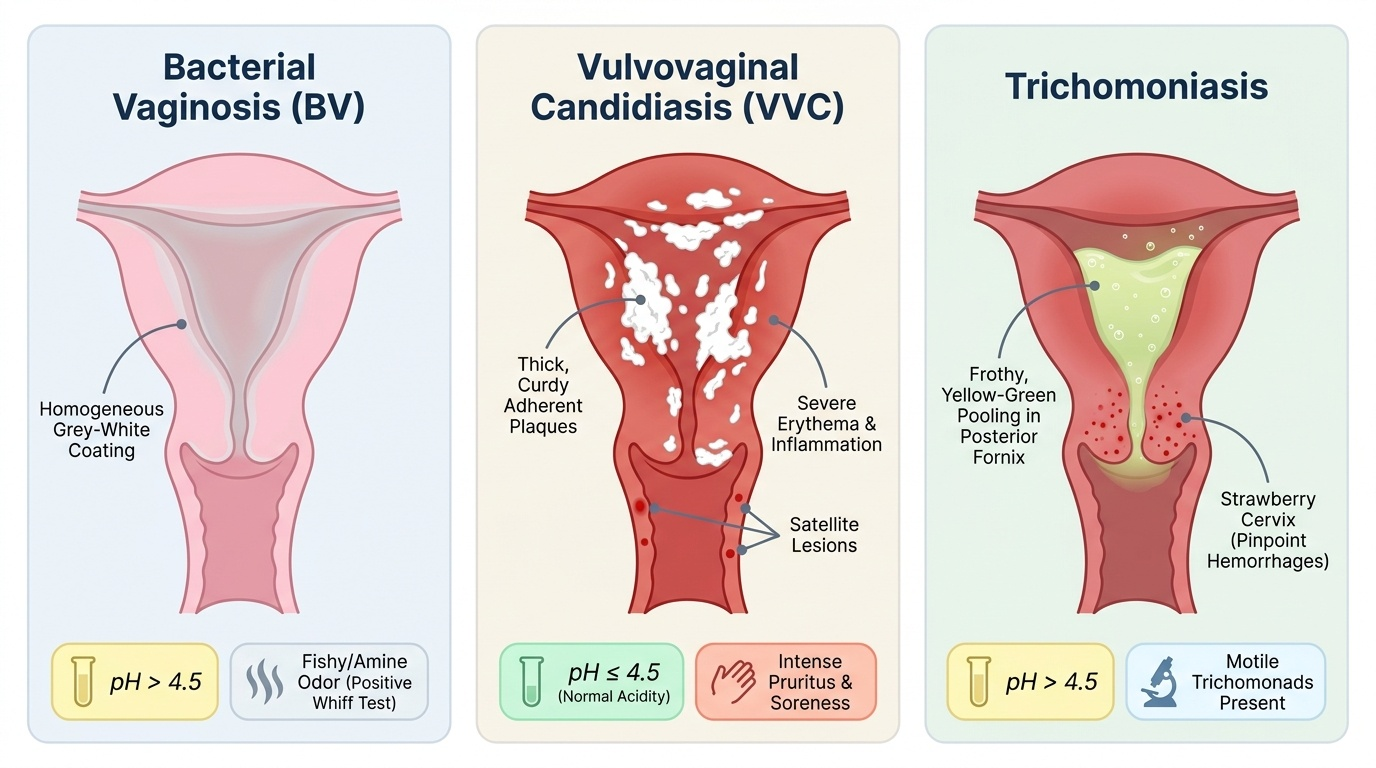
Bacterial vaginosis (BV) presents with a thin, homogeneous, greyish-white discharge that coats the vaginal walls in a uniform layer. The hallmark symptom is a fishy or amine odour that is often noticed by the woman herself and may worsen after intercourse or during menstruation (alkaline semen and menstrual blood liberate volatile amines). There is typically no vulval pruritus or soreness — the absence of itch is an important distinguishing feature from candidiasis. On examination, the vaginal walls appear coated but not inflamed or erythematous. BV accounts for approximately 40–50% of symptomatic vaginal discharge presentations in most settings. It is important to note that up to 50% of women with BV are asymptomatic — in these women the condition may still be detected incidentally on a routine swab or noted as an incidental finding in pregnancy screening.
Vulvovaginal candidiasis (VVC) presents with intense vulval pruritus as the dominant symptom — often described as unbearable, particularly at night. The discharge is characteristically thick, white, and curdy ('cottage cheese' or 'curd-like'), and adherent to the vaginal walls and ectocervix. On examination there is prominent vulval and vaginal erythema (bright red, inflamed mucosa). There is typically no offensive odour and vaginal pH remains ≤4.5 — both features that distinguish VVC from BV and trichomoniasis. Satellite lesions (erythematous macules beyond the main inflamed area) on the vulva suggest candidiasis. The condition is caused by Candida albicans in 80–90% of cases; non-albicans species (C. glabrata, C. tropicalis) account for the rest and are more likely to be azole-resistant.
Trichomoniasis presents with a profuse, frothy, yellow-green discharge — the 'frothy' quality is caused by CO₂ produced by the organisms and is one of the most specific clinical signs. There is an offensive odour and vulvosaginal soreness and dyspareunia. On speculum examination, the characteristic finding is a 'strawberry cervix' — punctate haemorrhages on the ectocervix (cervical petechiae) seen in approximately 10–20% of cases, though not pathognomonic. Vaginal pH is typically >4.5 (often 5–6). Trichomoniasis is a sexually transmitted infection caused by Trichomonas vaginalis, a flagellated protozoan; it virtually always requires simultaneous partner treatment.
Provided image
SELF-CHECK
A woman presents with vaginal discharge. On examination you find a thin, homogeneous, grey-white coating on the vaginal walls with a fishy odour but no vulval erythema or pruritus. Vaginal pH is 5.2. Which diagnosis fits best?
A. Vulvovaginal candidiasis
B. Trichomoniasis
C. Bacterial vaginosis
D. Physiological leucorrhoea
Reveal Answer
Answer: C. Bacterial vaginosis
Bacterial vaginosis presents with thin homogeneous grey-white discharge, fishy amine odour, pH >4.5, and — crucially — absence of pruritus or erythema. The lack of itch and inflammation distinguishes it from VVC (which has intense pruritus and erythema but no fishy odour and normal pH) and from trichomoniasis (which causes frothy yellow-green discharge with soreness, also pH >4.5). Physiological leucorrhoea has no odour and normal pH.
Pathophysiology and Aetiology of the Three Syndromes
Understanding why each syndrome produces its characteristic clinical features requires understanding the underlying microbiology and the mechanism by which each pathogen disrupts the vaginal ecosystem. Each syndrome involves a fundamentally different type of organism — polymicrobial bacteria, yeast, protozoan — and each disrupts the lactobacillus-pH axis through a distinct mechanism.
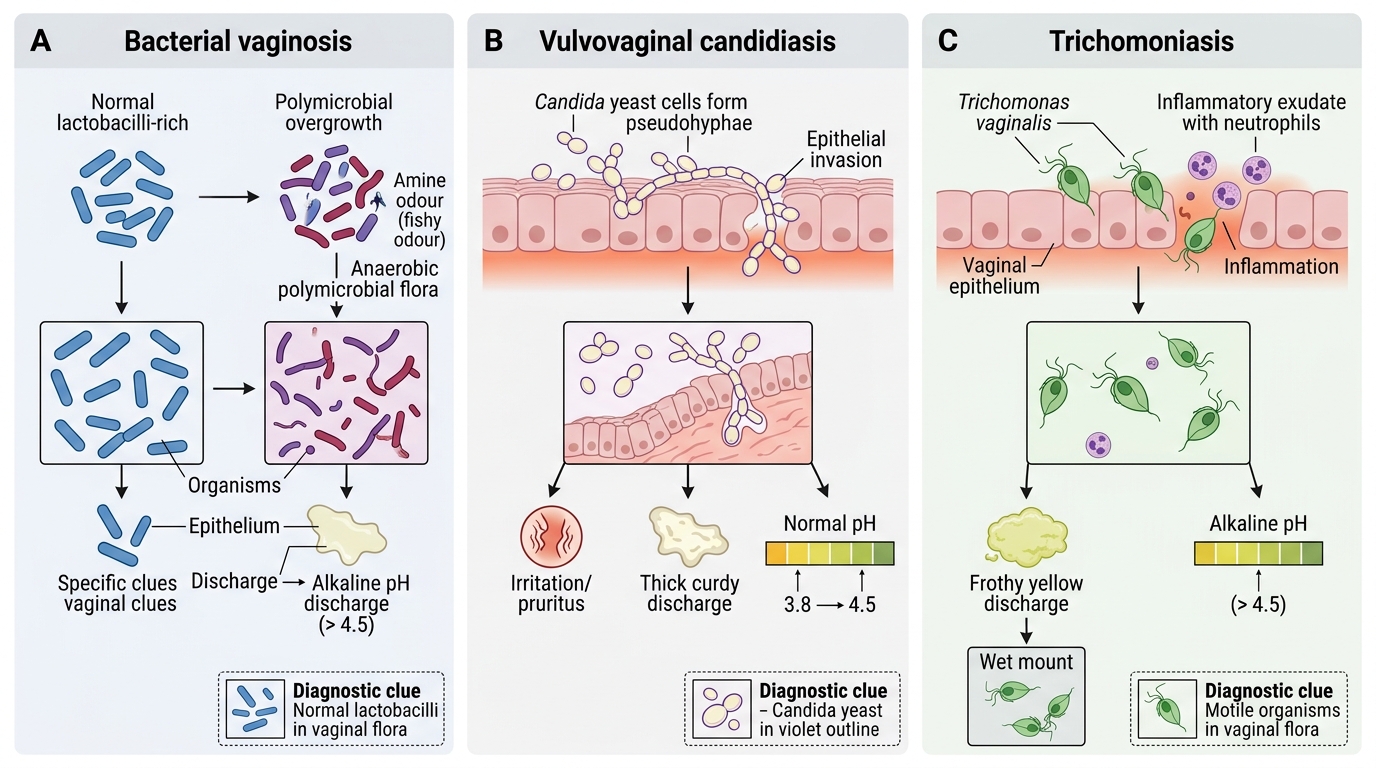
Bacterial vaginosis (BV) is not caused by a single organism but by a shift in the vaginal microbial community: the dominant Lactobacillus flora is replaced by a polymicrobial overgrowth of Gardnerella vaginalis (the index organism most reliably detected), anaerobic gram-negative rods (Mobiluncus spp., Bacteroides spp., Prevotella spp.), Mycoplasma hominis, and Ureaplasma species. This is fundamentally an ecological dysbiosis, not a classic infection with a single invading pathogen. The exact trigger for the shift is not fully understood; risk factors include sexual activity (multiple or new partners, though BV can occur without sexual exposure), vaginal douching, cigarette smoking, intrauterine device use, and antibiotic exposure. The overgrown organisms, especially Gardnerella and anaerobes, metabolise amino acids into volatile amines — particularly putrescine, cadaverine, trimethylamine — that produce the characteristic fishy odour. They also raise vaginal pH above 4.5 by consuming lactic acid. BV is associated with serious obstetric complications: it is an independent risk factor for preterm labour, preterm premature rupture of membranes (PPROM), and post-partum/post-abortal endometritis. Screening for and treating BV in pregnancy is therefore clinically significant, not merely cosmetic.
Vulvovaginal candidiasis (VVC) is caused by Candida albicans (80–90% of cases) and, less commonly, non-albicans species such as C. glabrata and C. tropicalis. Candida is a commensal organism present in the lower genital tract in about 20% of asymptomatic women; disease occurs when the ecological balance shifts in Candida's favour — most commonly through antibiotic-mediated depletion of protective Lactobacillus species. Other predisposing factors include: uncontrolled diabetes mellitus (elevated glycogen provides additional substrate for yeast), pregnancy (elevated oestrogen and glycogen), immunosuppression (HIV, corticosteroids, chemotherapy), and tight synthetic clothing (local heat and moisture). Candida produces pseudohyphae — elongated, branching filamentous forms that penetrate vaginal epithelial cells, triggering an inflammatory response with intense pruritus, erythema, and the characteristic thick curd-like exudate. Notably, Candida does not produce amines and does not alkalinise the vaginal environment, so pH remains ≤4.5.
Trichomoniasis is caused by Trichomonas vaginalis, a flagellated protozoan (not a bacterium or fungus) that is transmitted exclusively by sexual contact — it has no non-sexual reservoir and cannot survive for significant periods outside the human host. T. vaginalis is the most common non-viral sexually transmitted infection globally, and in India its prevalence in symptomatic discharge is approximately 5–20%. The organism attaches to vaginal epithelial cells via surface adhesins, triggering a pronounced acute inflammatory response with polymorphonuclear infiltration, producing the frothy yellow-green discharge and vulval soreness. It raises vaginal pH above 4.5 through its own metabolic activity. Importantly, T. vaginalis infection facilitates HIV transmission (increases viral shedding and increases susceptibility) and is associated with adverse pregnancy outcomes (preterm birth). It is also associated with male urethritis, though men are often asymptomatic — explaining why simultaneous partner treatment is mandatory to prevent reinfection ('ping-pong' reinfection).
Mechanisms of the Three Vaginal Discharge Syndromes
Diagnosis: Amsel Criteria, Nugent Score, and Point-of-Care Tests
Accurate diagnosis of vaginal discharge syndromes requires interpreting clinical findings alongside simple point-of-care tests — specifically vaginal pH, the whiff test, and wet mount microscopy — and, in referral settings, gram-stained smear scoring (Nugent). Each of these tests is inexpensive, rapid, and interpretable at the bedside without sophisticated equipment. Together they provide more diagnostic accuracy than clinical appearance alone. The diagnostic framework described here is structured around the three tests you should apply to every patient presenting with discharge: first measure vaginal pH with narrow-range pH paper, then perform the whiff test, then prepare a saline wet mount — a sequence that takes under five minutes and dramatically narrows the differential before any laboratory culture result is available. This sequence is what distinguishes systematic clinical reasoning from pattern-matching on appearance alone, and it is the approach that Amsel's original 1983 study validated against clinical outcome.
Amsel's criteria for BV diagnosis: BV is diagnosed when three of the following four criteria are present — not all four, and not fewer than three:
1. Homogeneous, thin, grey or white discharge that smoothly coats the vaginal walls
2. Vaginal pH >4.5 (measured with narrow-range pH paper applied to the lateral vaginal wall)
3. Positive whiff (amine) test — a drop of 10% potassium hydroxide (KOH) added to a sample of the discharge produces an immediate, pungent fishy amine odour (positive = BV or TV; negative = candida)
4. Clue cells >20% of epithelial cells on wet mount (saline preparation) — clue cells are vaginal squamous epithelial cells whose surfaces and edges are densely studded with coccobacilli (Gardnerella), giving them a granular, stippled appearance with indistinct cell borders
The Amsel criteria are the primary clinical tool for BV diagnosis; they are used at the bedside and require no laboratory equipment beyond pH paper and a microscope.
Nugent score is a gram-stain-based scoring system applied to a smear of vaginal discharge: it scores the density of large gram-positive rods (Lactobacillus morphotypes, scored 0–4), small gram-variable rods (Gardnerella/Bacteroides morphotypes, scored 0–4), and curved gram-variable rods (Mobiluncus morphotypes, scored 0–2), for a total of 0–10. Score 0–3 = normal; 4–6 = intermediate flora (indeterminate, may progress to BV); 7–10 = BV. The Nugent score is the reference standard in research settings and is more objective than the Amsel criteria, but requires a trained microscopist.
Wet mount microscopy findings by syndrome:
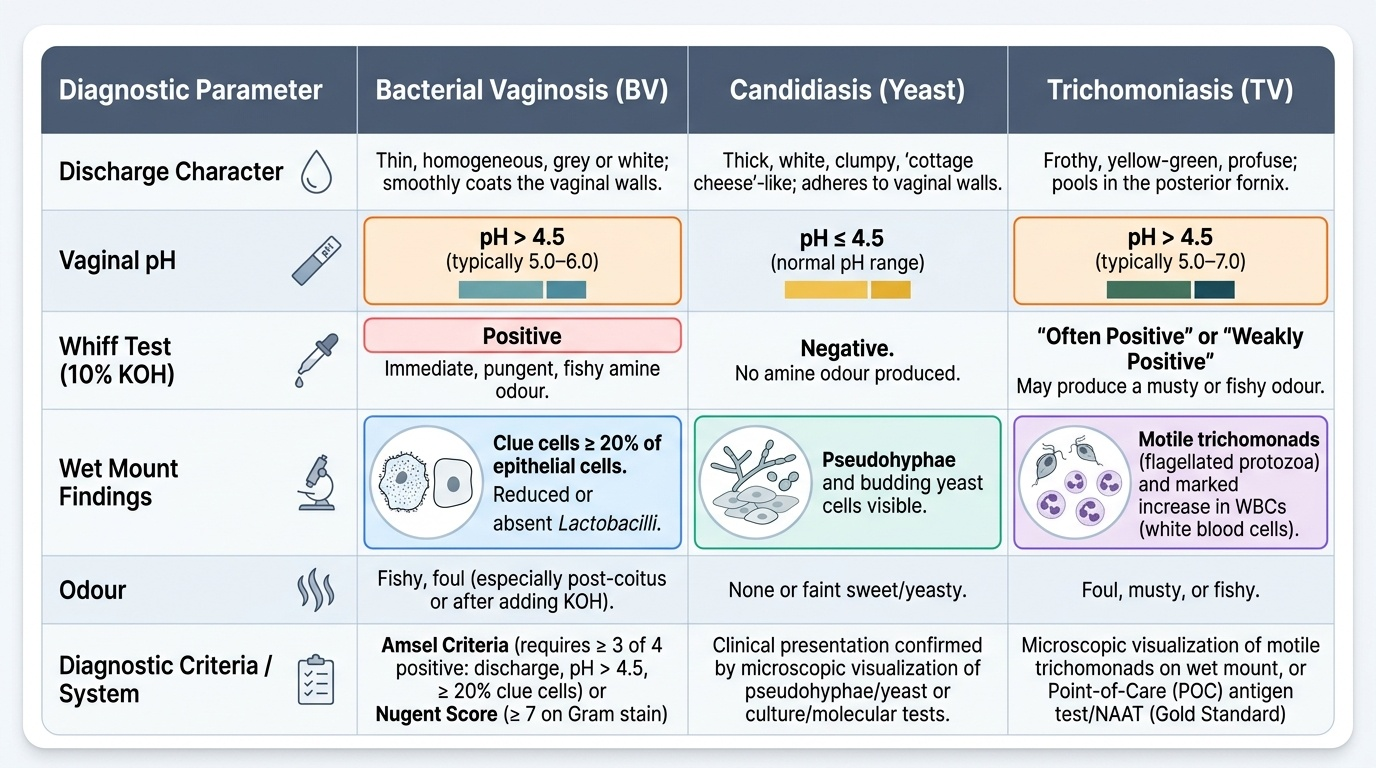
- BV: clue cells (>20% of epithelial cells); absence of lactobacilli; many gram-variable rods; few white cells (important — BV causes minimal inflammation, unlike trichomoniasis)
- VVC: pseudohyphae or hyphae (branching filamentous forms) ± budding yeast cells on KOH preparation (KOH dissolves epithelial cells, making fungal elements easier to see); many WBCs; normal lactobacilli may still be present. Culture on Sabouraud agar if KOH negative in suspected candidiasis.
- Trichomoniasis: motile, pear-shaped, flagellated trichomonads — identification requires a fresh wet mount (motility is rapidly lost within 10–20 minutes of preparation); many WBCs (prominent inflammation); clue cells absent; pH >4.5; whiff test may be positive
Additional investigations for trichomoniasis: culture in Diamond's medium is the gold standard but rarely available in India; NAAT (nucleic acid amplification test) is the most sensitive test available in tertiary settings; newer rapid antigen tests are available in some referral centres.
Provided image
SELF-CHECK
A wet mount smear from a woman with grey-white discharge shows vaginal epithelial cells whose surfaces are densely coated with small coccobacilli, giving them an indistinct, granular border. Vaginal pH is 5.1 and the whiff test is positive. How many of Amsel's criteria are satisfied, and what is the diagnosis?
A. Two criteria (pH >4.5 + positive whiff); diagnosis is indeterminate — more tests needed
B. Three criteria (discharge character + pH >4.5 + positive whiff); bacterial vaginosis confirmed
C. Three criteria (discharge character + clue cells + positive whiff); bacterial vaginosis confirmed
D. Three criteria (pH >4.5 + clue cells + positive whiff); bacterial vaginosis confirmed
Reveal Answer
Answer: D. Three criteria (pH >4.5 + clue cells + positive whiff); bacterial vaginosis confirmed
The question states: pH >4.5 (criterion 2), positive whiff test (criterion 3), and clue cells on wet mount (criterion 4). The discharge character (criterion 1) is also described as grey-white and homogeneous, so actually all four criteria are met — but BV requires ≥3 of 4. The 'clue cells' finding is the classic microscopic hallmark: epithelial cells studded with coccobacilli with indistinct granular borders, representing Gardnerella adhering to the cell surface. Option D correctly identifies the three explicitly tested criteria; in the clinical scenario all four Amsel criteria are actually present.