Page 22 of 28
OG22.2 | Common Vaginal Discharge Syndromes — SDL Guide (Part 2)
Management: Specific and Syndromic Treatment
Management of vaginal discharge syndromes requires selecting the appropriate antimicrobial for each specific syndrome, counselling on compliance and partner treatment where relevant, and providing genital hygiene advice that prevents recurrence. In settings with access to microscopy and laboratory diagnosis, treatment is pathogen-directed. In primary care settings without laboratory support, the syndromic management approach — treating on the basis of clinical syndrome pattern — is the recommended and evidence-based alternative endorsed by both WHO and India's NRHM guidelines.
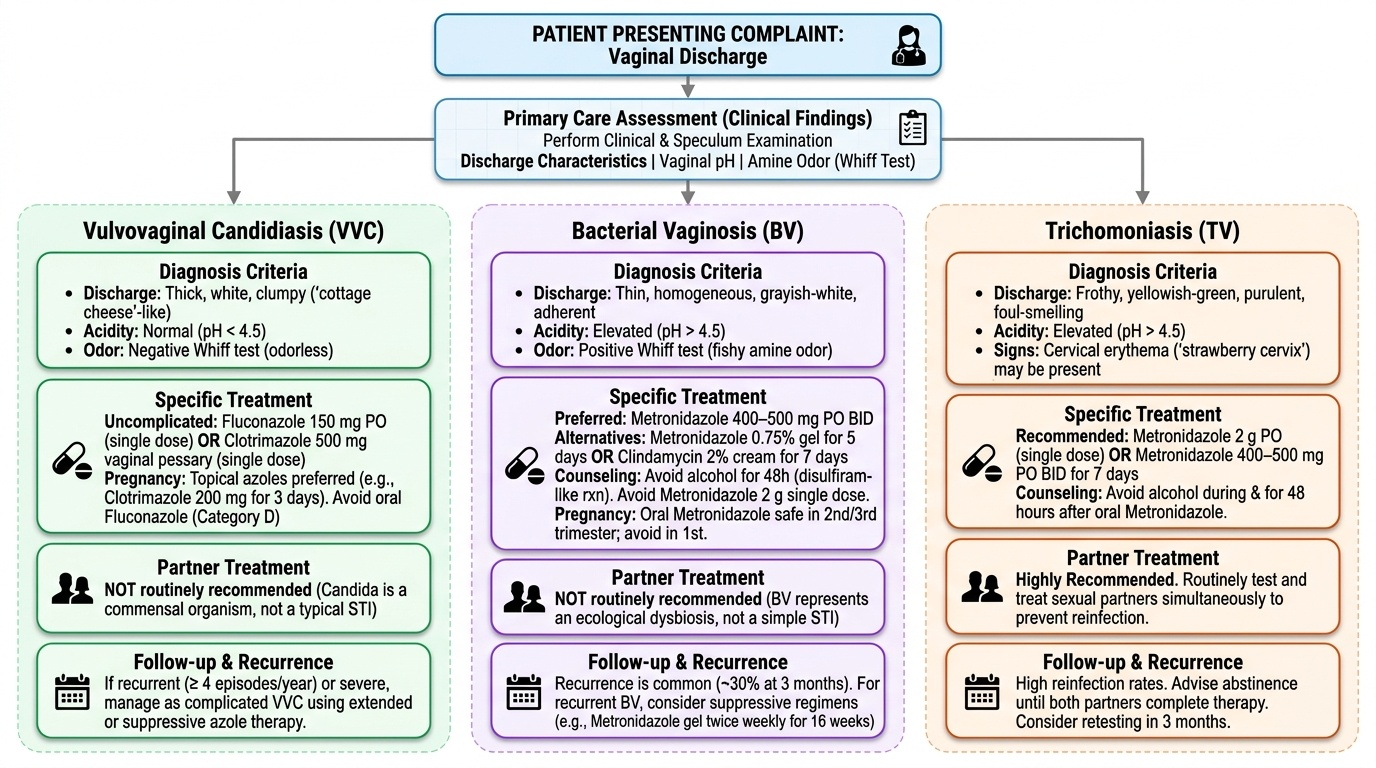
Bacterial vaginosis — specific treatment:
First-line regimens (any of the following): metronidazole 400–500 mg orally twice daily for 7 days (preferred; high cure rates, well tolerated); OR metronidazole 0.75% intravaginal gel once daily for 5 days; OR clindamycin 2% intravaginal cream at bedtime for 7 days. Metronidazole 2 g single oral dose is NOT recommended for BV (lower cure rates than 7-day regimen). Advise the patient to avoid alcohol during and for 48 hours after oral metronidazole (disulfiram-like reaction). Partner treatment is NOT routinely recommended for BV (unlike trichomoniasis), as BV is an ecological dysbiosis, not a simple STI. In pregnancy, BV should be treated because of its association with preterm labour; oral metronidazole is safe in the second and third trimesters; avoid in the first trimester if possible. Recurrence is common (approximately 30% at 3 months with a single course); for recurrent BV, consider extended or suppressive regimens (e.g., metronidazole gel twice weekly for 16 weeks after initial cure).
Vulvovaginal candidiasis — specific treatment:
For uncomplicated VVC (first episode, mild-moderate, immunocompetent, non-pregnant, likely C. albicans): fluconazole 150 mg orally as a single dose — the most convenient and widely used option. Alternatively, any of the intravaginal azole preparations (clotrimazole 500 mg pessary single dose; clotrimazole 200 mg pessary for 3 days; miconazole cream/pessary; butoconazole). Topical preparations cause fewer systemic effects and are preferred in pregnancy (fluconazole is avoided in the first trimester; category D). Partner treatment is NOT routinely required for VVC (Candida is a commensal, not a typical STI). For complicated VVC (recurrent ≥4 episodes/year, severe, non-albicans species, immunocompromised, or diabetic): longer courses (fluconazole 150 mg every 72 hours for 3 doses as induction, then weekly suppression for 6 months) and culture with sensitivity testing. Boric acid intravaginal capsules are used for azole-resistant C. glabrata.
Trichomoniasis — specific treatment:
First-line: metronidazole 2 g orally as a single dose — preferred for compliance (equivalent efficacy to 7-day regimen in trials). Alternative: metronidazole 400–500 mg twice daily for 7 days. Simultaneous partner treatment is mandatory — without it, reinfection from the untreated partner (ping-pong reinfection) is virtually certain within weeks. The couple should abstain from intercourse until both partners have completed treatment and are asymptomatic. Screen for co-existing STIs (HIV, syphilis, gonorrhoea, chlamydia) in all patients diagnosed with trichomoniasis. In pregnancy, metronidazole can be used in the second trimester onward; trichomoniasis in pregnancy is associated with preterm birth and should be treated.
Syndromic management algorithm (primary care without microscopy):
In settings where microscopy is not available, the WHO/NRHM syndromic approach treats all women presenting with vaginal discharge who have one or more risk markers (new or multiple partners, partner with STI, symptoms suggesting PID) with a combined regimen covering BV and trichomoniasis: metronidazole 2 g single dose (covers TV) + metronidazole 400 mg BD × 7 days (covers BV, or combine as metronidazole 500 mg BD × 7 days). Candidiasis is added to the regimen when clinical features strongly suggest it (pruritus, curdy discharge): add fluconazole 150 mg single dose. Partner referral and treatment is advised for all syndromic-managed women to prevent reinfection.
Genital hygiene counselling for all discharge syndromes:
The following advice applies to all women treated for vaginal discharge syndromes: (1) Avoid vaginal douching — it disrupts protective flora and promotes recurrence. (2) Wear breathable cotton underwear; avoid tight synthetic garments. (3) Complete the full antibiotic/antifungal course even if symptoms resolve early. (4) Return for review if symptoms recur within one month of treatment completion.
Provided image
SELF-CHECK
A woman is diagnosed with trichomoniasis on wet mount. She is prescribed metronidazole 2 g as a single oral dose and advised to abstain from intercourse for 7 days. Her husband is asymptomatic. What is the most appropriate next step regarding the husband?
A. No treatment needed as he is asymptomatic; advise repeat testing in 3 months
B. Test the husband and treat only if he tests positive
C. Treat the husband simultaneously with metronidazole 2 g single dose regardless of symptoms
D. Advise the husband to use condoms for 3 months; no medication needed
Reveal Answer
Answer: C. Treat the husband simultaneously with metronidazole 2 g single dose regardless of symptoms
Trichomoniasis requires simultaneous partner treatment irrespective of symptoms. T. vaginalis causes asymptomatic carriage in the majority of infected men (male urethra is the reservoir). If the partner is not treated at the same time, the woman will be reinfected at the next intercourse — the 'ping-pong' reinfection cycle. The standard regimen for the male partner is metronidazole 2 g single dose. Testing alone and then waiting for a positive result before treating introduces delay and risks continued transmission. Condom use alone is insufficient — it reduces transmission risk but does not eliminate it or treat the existing infection.
Self-Assessment: Vaginal Discharge Syndromes
The following questions integrate all four sections of this SDL. Each question is designed to test clinical reasoning across presentation, diagnosis, and management — the exact competency that OG22.2 (KH level, assessed in written examinations and viva voce) requires. For each scenario, work through your differential diagnosis systematically before choosing an answer: identify the discharge character, odour, pH, microscopy clues, and risk factors in the question stem, then apply Amsel's criteria or the syndromic algorithm as appropriate. These are the same reasoning steps you will use at the bedside. Attempt each question independently in writing before reviewing your notes. The five scenarios below span the full scope of the competency: diagnosis in pregnancy (where BV has obstetric consequences), management of complicated or recurrent candidiasis, partner treatment principles for trichomoniasis, syndromic management in a resource-limited setting, and interpretation of the whiff test. A learner who can reason through all five fluently is ready for the viva voce assessment on this topic.
- A 28-year-old woman at 18 weeks of gestation presents for routine antenatal care. She is asymptomatic but a routine high vaginal swab reports 'clue cells ++, few lactobacilli, pH 5.0'. Should this be treated? If yes, what drug, dose, and regimen? What obstetric risk is associated with untreated BV in pregnancy?
- A 35-year-old woman with poorly controlled type 2 diabetes presents with recurrent vulval pruritus and thick white discharge for the fourth time this year. Each previous episode was treated with a single dose of fluconazole. What is the diagnosis, what category (uncomplicated vs complicated) does it fall into, and what is the appropriate management change?
- A 22-year-old woman presents with frothy yellow-green discharge, vulval soreness, and a pH of 5.5. Wet mount shows pear-shaped motile organisms. Her male partner has had a urethral discharge for 2 weeks but has not sought treatment. Outline the management plan for both the woman and her partner.
- A primary health centre physician sees a 30-year-old woman with vaginal discharge in a setting without microscopy. She has two sexual partners in the past 3 months. Her discharge is thin, grey-white, with a fishy odour. pH paper from the clinic reads >4.5. Using the WHO syndromic management approach, what treatment should be prescribed?
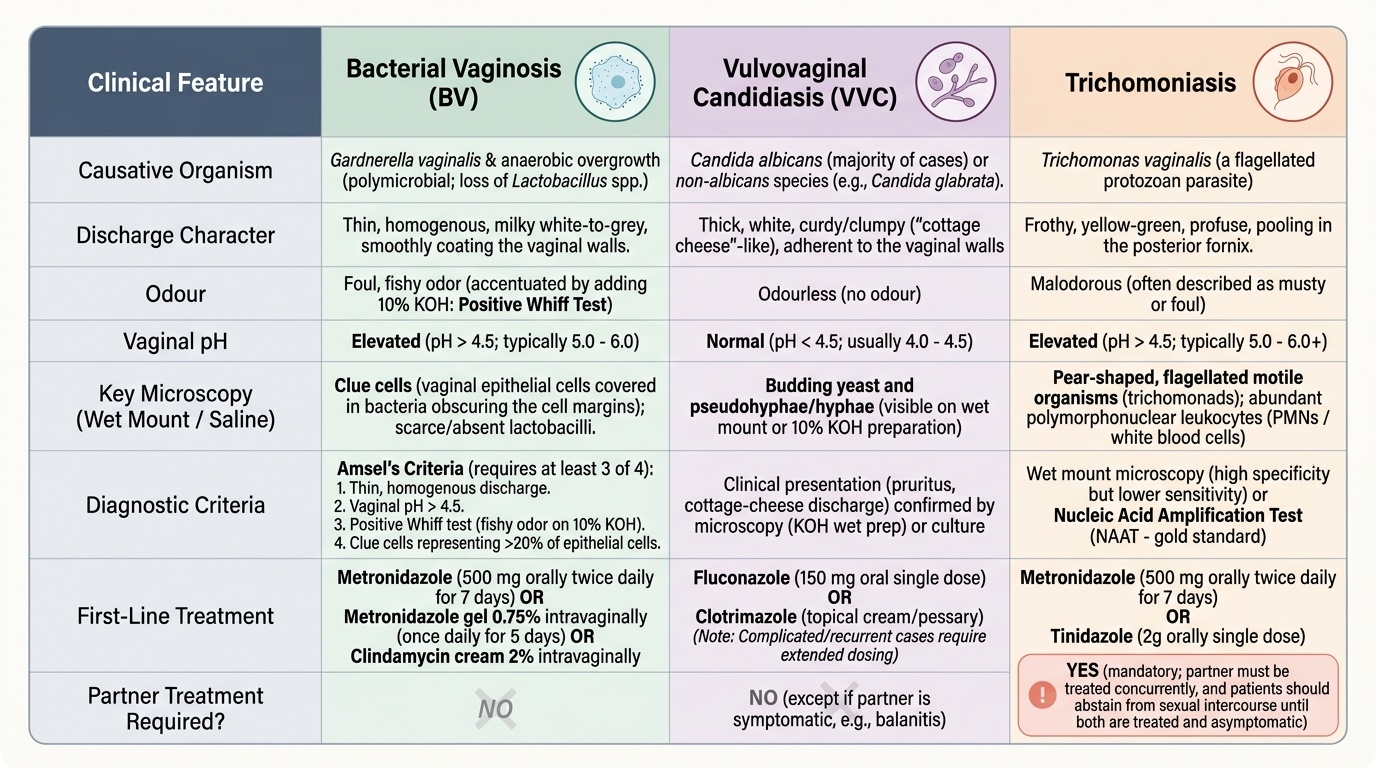
- You perform a whiff test by adding KOH to a vaginal swab. The result is strongly positive (immediate fishy odour). What does a positive whiff test indicate, and for which discharge syndromes is it seen?
Provided image
CLINICAL PEARL
The single most common mistake in vaginal discharge management is prescribing antifungals for bacterial vaginosis. This error arises from conflating 'discharge' with 'yeast infection' — a misconception reinforced by widespread over-the-counter antifungal marketing. The key discriminators at the bedside are pH and odour: fishy odour + pH >4.5 = BV or trichomoniasis; thick white curdy discharge + pruritus + pH ≤4.5 = candidiasis. A single narrow-range pH strip and the whiff test take under 60 seconds and immediately redirect the diagnosis. In pregnancy, missing BV means missing a treatable cause of preterm birth — never dismiss discharge in an antenatal patient without at least measuring pH.