Page 1 of 28
OG20.1 | Medical Termination of Pregnancy — SDL Guide
Learning Objectives
- Enumerate the legal indications for Medical Termination of Pregnancy under the MTP Act 1971 (amended 2021)
- Describe the gestational-age tiers and the number of RMP opinions required at each tier
- Discuss first-trimester and second-trimester methods of MTP including medical and surgical approaches
- Enumerate and manage the complications of MTP
INSTRUCTIONS
Unsafe abortion remains a leading contributor to maternal mortality in India. Every practitioner of obstetrics must know the current legal framework, gestational thresholds, eligible method options, and how to recognise and manage complications. This module walks you through all four dimensions — law, patient assessment, method selection, and complication care — using the MTP Act 1971 as amended by the Medical Termination of Pregnancy (Amendment) Act 2021 and the MTP Rules 2021.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Chap 14 (Medical Termination of Pregnancy) (textbook)
- Williams Obstetrics, 26th ed., Chap 18 (Abortion) (textbook)
- MTP Amendment Act 2021 and MTP Rules 2021, Ministry of Health and Family Welfare, Government of India (guideline)
- WHO Safe Abortion: Technical and Policy Guidance, 2nd ed., 2012 (updated 2022) (guideline)
- FOGSI Good Clinical Practice Recommendations — Medical Methods of Termination of Pregnancy, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman presents to your outpatient clinic at 8 weeks of gestation. She reveals that the pregnancy resulted from contraceptive failure and that she and her partner are not in a position to raise a child at this time. She asks whether she can legally end the pregnancy and how it would be done. A colleague asks you whether one doctor's opinion is sufficient or whether two are needed. How do you counsel her, and which method would you choose?
WHY THIS MATTERS
India accounts for approximately 13% of global maternal deaths attributable to unsafe abortion. The MTP Act 1971, significantly updated in 2021, provides a legal and safe framework for terminating unwanted or high-risk pregnancies. As a graduating doctor, you will encounter requests for MTP in primary-care settings, casualty, and outpatient gynaecology. Understanding the law, the gestational thresholds, the available methods, and the complications is non-negotiable for safe, legal, and compassionate care.
RECALL
Before proceeding, recall the following from earlier modules: (1) Gestational age is dated from the first day of the last menstrual period (LMP) and confirmed by first-trimester ultrasonography; the crown-rump length is the most accurate dating tool before 14 weeks. (2) The embryo transitions to a fetus at 8 weeks; viability (capacity for independent extra-uterine survival) is generally accepted at 22–24 weeks with neonatal intensive care. (3) Abortion is defined as expulsion or extraction of a fetus weighing less than 500 g or before 20 weeks of gestation. Review the definition — it underpins the legal structure.
The Unwanted Pregnancy: Scope and Clinical Context
Unwanted pregnancy is a pregnancy that is mistimed, unplanned, or unwanted at the time of conception, regardless of the woman's subsequent decision to continue or terminate. Globally, approximately 45% of all pregnancies are unintended, and nearly half of these end in induced abortion. In India, the Sample Registration System and District Level Household Survey data consistently document high rates of unsafe, clandestine abortion in settings without access to trained providers, leading to haemorrhage, sepsis, and maternal death. The burden is highest in young women, women of low socioeconomic status, and those in conflict zones or with limited literacy.
Clinically, women who request MTP may present across a spectrum of contexts. Some have experienced contraceptive failure — a missed pill cycle, condom rupture, or IUCD expulsion. Others present after sexual assault, including cases where the woman is a minor. Pregnancies in women carrying known or suspected foetal anomalies detected on prenatal diagnosis form a distinct and increasingly important category. Additionally, pregnancies that pose a grave risk to the physical or mental health of the woman — severe cardiac disease, severe pre-eclampsia diagnosed early, or worsening renal disease — constitute medical indications that cross both obstetric and ethical dimensions.
Understanding the clinical context in which MTP is requested helps the practitioner apply the correct legal provision and choose the most appropriate method. The law in India does not require a woman to justify her reasons beyond the categories enumerated in the MTP Act — the decision is ultimately hers, within the legal framework.
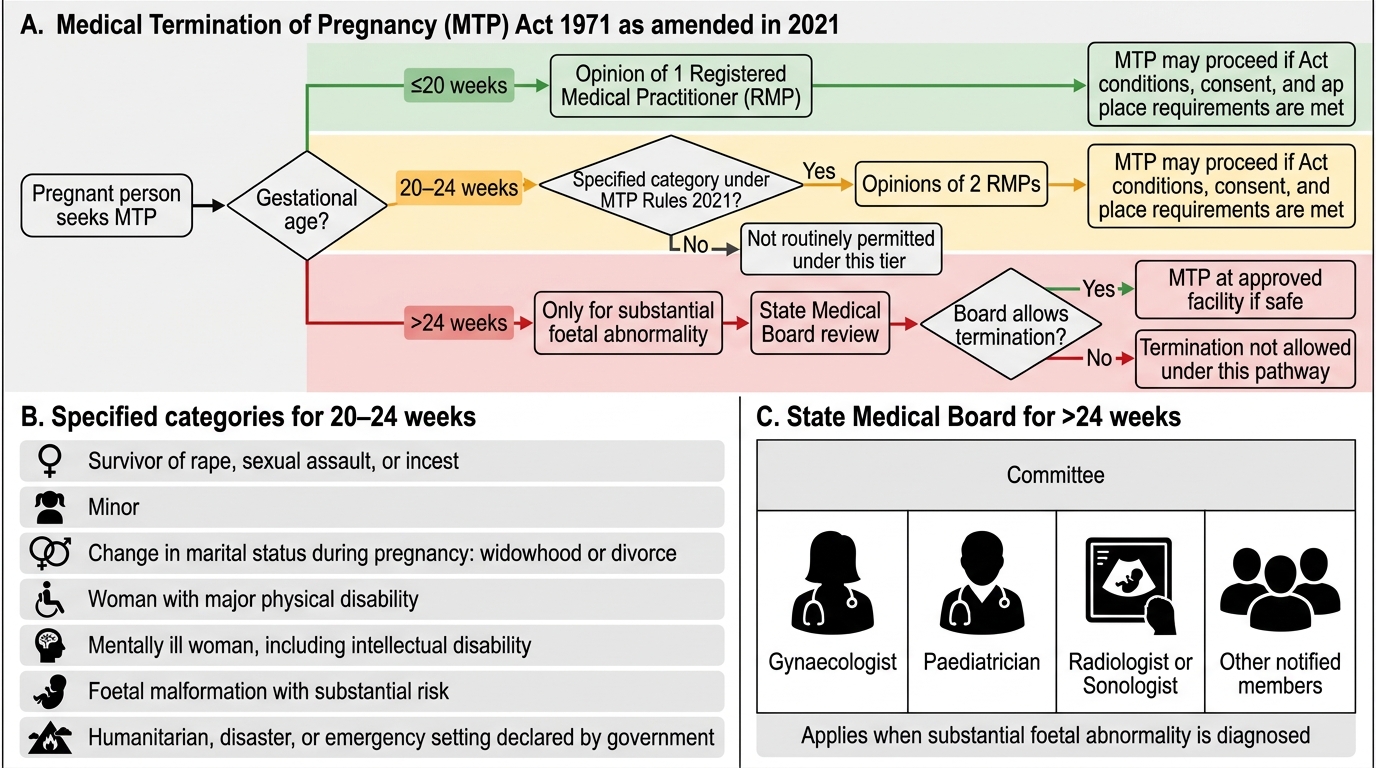
MTP Act 2021 Gestational-Age Decision Flow
Embryological and Gestational Basis of MTP
The physiological rationale for gestational-age thresholds in abortion law rests on the progressive biological development of the conceptus, increasing procedural complexity with advancing gestation, and rising maternal risk. In the first trimester (up to 12 completed weeks), the embryo and early fetus are entirely dependent on the placenta and uterine environment; no organ system is capable of independent function. Fetal viability — the capacity for sustained extra-uterine survival — is generally set at 22–24 weeks, beyond which intensive neonatal care can sustain some premature newborns. This biological boundary explains the legislative distinction between first-trimester termination (low risk, several safe methods) and second-trimester termination (higher risk, more restricted methods).
Gestational age must be accurately established before MTP because both the legal threshold and the method choice are directly governed by the number of completed weeks. The preferred tool is transvaginal ultrasonography in the first trimester, using the crown-rump length (CRL) between 6 and 14 weeks; dating by CRL carries a margin of error of ±5 days. Transabdominal USG with biparietal diameter is used in the second trimester. Menstrual dating alone is unreliable in women with irregular cycles or uncertain LMP. A discordance of more than 7 days between menstrual and ultrasound dating should prompt clinical review before proceeding.
The uterus itself undergoes progressive changes with gestation — the myometrium thickens, blood supply increases, and the cervix softens — that affect both the ease of surgical access and the response to pharmacological agents. These anatomical facts explain why misoprostol doses and intervals differ between first and second trimester, and why surgical evacuation in the second trimester carries higher risk of haemorrhage and perforation than in the first.
Legal Framework: MTP Act 1971 and the 2021 Amendment
The Medical Termination of Pregnancy Act, 1971 is the primary statute governing induced abortion in India. For decades it permitted MTP up to 20 weeks of gestation, subject to specific indications and the opinion of one or two registered medical practitioners (RMPs). The Medical Termination of Pregnancy (Amendment) Act, 2021, with its accompanying MTP Rules, 2021, substantially revised the upper gestational limit, expanded the categories of women eligible for later termination, and for the first time explicitly acknowledged that the need for safe abortion is not confined to any particular marital status — a long-overdue recognition of clinical and social realities. These amendments reflect advocacy by women's health organisations, FOGSI, and international human-rights bodies urging India to align its law with contemporary practice. Under the current framework, the critical determinant of the legal pathway is gestational age in completed weeks, established by ultrasound dating. The law creates three distinct tiers, each with different RMP-opinion requirements and eligibility criteria; a practitioner who proceeds outside the correct tier is both clinically unsafe and legally liable.
Gestational tiers under current law (MTP Rules 2021):
1. Up to 20 weeks of gestation: A single registered medical practitioner's (RMP's) opinion is sufficient. The pregnancy may be terminated if:
- Continuation would involve risk to the life of the woman, or injury to her physical or mental health (including the distress caused by actual or reasonably foreseeable environment); or
- There is a substantial risk that if the child were born, it would suffer from such physical or mental abnormalities as to be seriously handicapped.
2. 20 to 24 weeks of gestation: The opinion of TWO RMPs is required, AND the woman must fall into one of the specified categories (MTP Rules 2021, Rule 3B):
- Survivors of rape or sexual assault, including incest
- Minors (women below 18 years of age)
- Change of marital status during an ongoing pregnancy (widowhood, divorce)
- Differently abled women (physical/intellectual/psychiatric disability)
- Foetal malformation incompatible with life or substantial foetal anomaly
- Humanitarian settings, including disasters or emergencies declared by government
- Beyond 24 weeks of gestation: Termination is permitted ONLY for substantial foetal abnormality diagnosed by a Medical Board constituted by the State Government. The Board includes a gynaecologist, a paediatrician, a radiologist or sonologist, and other expert members as the State deems necessary.
Additional legal points to remember: the woman's written or oral consent (for herself, or her guardian if under 18 or mentally incapacitated) is mandatory. The identity of the woman is confidential. MTP must be performed in a government hospital or a place approved under the Act. A registered medical practitioner under the Act includes a doctor registered under the Indian Medical Council Act with a recognised post-graduate qualification in obstetrics/gynaecology, or who has experience of MTP as specified — the exact qualifications are defined in Rules 2003 amended 2021.
The most important trap to avoid: Do not quote the pre-2021 ceiling of 20 weeks as the current upper limit. Under the 2021 amendment, 20–24 weeks is now legal for specified categories with two RMPs. The absolute limit remains 24 weeks for normal pregnancies; beyond 24 weeks only the State Medical Board can authorise, and only for foetal abnormality.