Page 2 of 28
OG20.1 | Medical Termination of Pregnancy — SDL Guide (Part 2)
Eligibility Assessment and Pre-procedure Workup
Before performing MTP, the clinician must establish that the procedure is legally and medically appropriate for this particular woman at this gestational age. Rushing to a technique without a structured pre-procedure framework is one of the commonest root causes of MTP complications — inaccurate gestational-age assessment leads to wrong method selection, missed ectopic pregnancies have caused maternal deaths following medical MTP, and undetected anaemia worsens haemorrhagic outcomes. The eligibility assessment therefore encompasses three parallel and simultaneous streams: legal eligibility (confirming the woman falls within a permitted indication and gestational tier under the MTP Act), clinical suitability (identifying contraindications or conditions requiring special management), and informed consent (documented after non-directive counselling on all available options including continuing the pregnancy). Each stream must be completed before scheduling the procedure.
The pre-procedure workup for MTP includes:
- Gestational age confirmation: Ultrasound — mandatory to confirm intrauterine location, gestational age, and number of embryos. Ectopic pregnancy must be excluded before any medical or surgical MTP.
- Blood investigations: Haemoglobin/haematocrit (anaemia < 8 g/dL increases risk of medical-method failure and haemorrhagic complications), blood group and Rh type (Rh-negative women require anti-D immunoglobulin within 72 h of MTP), and baseline coagulation if second-trimester termination is planned.
- Cervical examination: Assess cervical dilatation and condition — relevant for method selection; cervical priming may be needed before surgical evacuation.
- Contraindications to mifepristone (for medical MTP): known hypersensitivity, chronic adrenal insufficiency, concurrent long-term corticosteroid therapy, inherited porphyria, coagulopathy, or anticoagulant therapy.
- Contraindications to misoprostol: Known hypersensitivity; caution in severe asthma (though prostaglandin E1 is generally safe; the risk is less than with carboprost PGF2α).
Counselling before MTP must be non-directive, covering: (a) the woman's decision is hers and will be respected; (b) the available methods, their efficacy, the need for follow-up, and what to expect; (c) contraception options after MTP to prevent recurrence; (d) psychological support if needed. All discussions and the woman's consent must be documented.
SELF-CHECK
Under the MTP (Amendment) Act 2021, a 22-year-old rape survivor at 22 weeks gestation requests termination. Which of the following correctly describes the legal requirement?
A. One RMP's opinion is sufficient because she is a rape survivor
B. Two RMPs' opinions are required and the case qualifies under specified categories
C. This is beyond the legal limit and cannot be performed
D. The State Medical Board must approve because gestation is >20 weeks
Reveal Answer
Answer: B. Two RMPs' opinions are required and the case qualifies under specified categories
Under MTP Rules 2021, the 20–24 week window requires TWO RMPs' opinions AND the woman must fall into a specified category (Rule 3B). Rape/sexual assault survivors are explicitly listed. The State Medical Board is required only beyond 24 weeks for foetal abnormality. One RMP opinion suffices only up to 20 weeks.
First-Trimester MTP: Medical and Surgical Methods
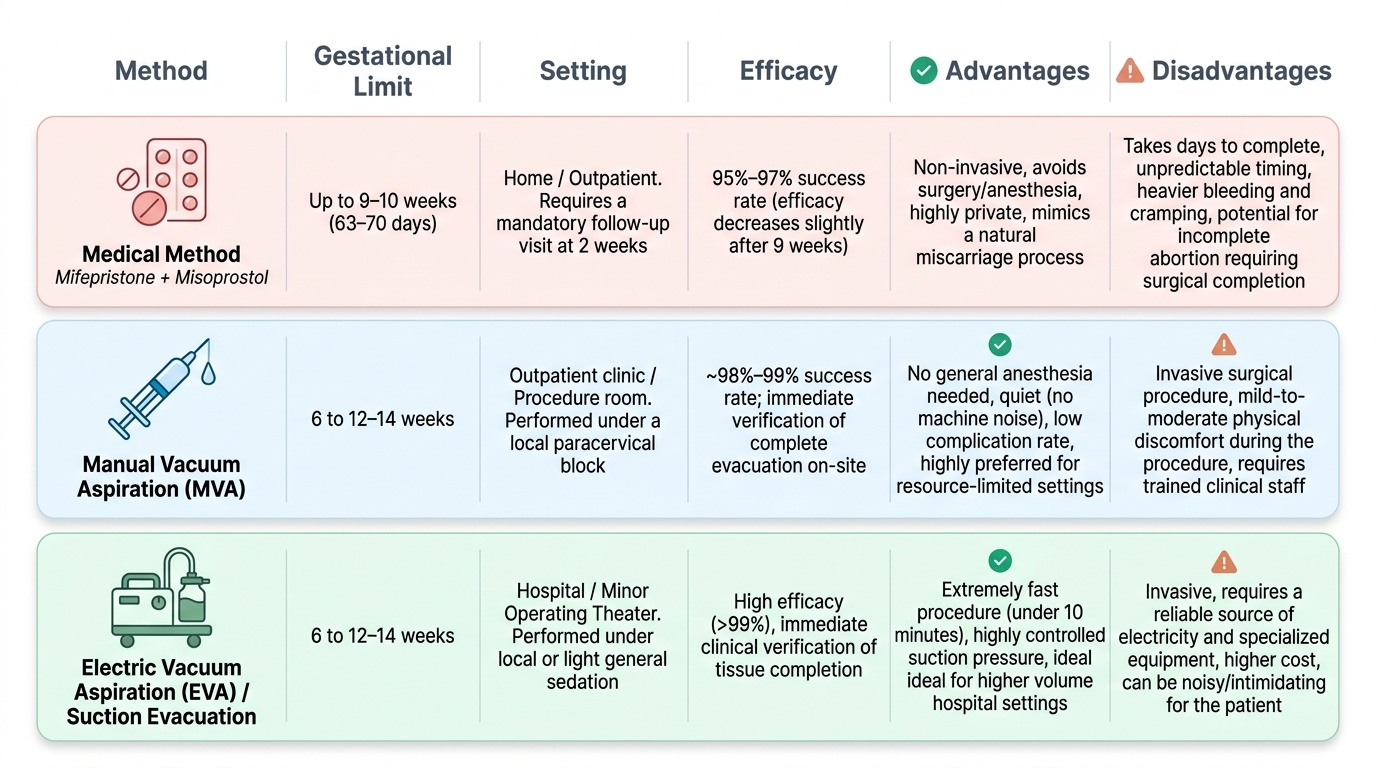
First-trimester MTP (up to 12 completed weeks, practically up to 9–10 weeks for medical method) can be safely accomplished either pharmacologically or surgically. The choice depends on gestational age, patient preference, clinical setting, and contraindications. Both methods are highly effective when performed correctly.
Medical method (mifepristone + misoprostol): The current regimen approved by the Ministry of Health and Family Welfare (MoHFW) and supported by WHO is mifepristone 200 mg orally followed 24–48 hours later by misoprostol 800 mcg administered sublingually, vaginally, or buccally. This combination is effective up to 9–10 weeks (63–70 days) of gestation. Mifepristone is a competitive antiprogesterone that primes the uterus by blocking progesterone receptors, leading to endometrial decidualization, cervical softening, and increased myometrial sensitivity to prostaglandins. Misoprostol, a synthetic prostaglandin E1 analogue, then causes uterine contractions and cervical dilatation, completing the expulsion. The overall complete abortion rate is approximately 95–97% up to 9 weeks; failure rates increase modestly beyond 9 weeks. A follow-up visit at 2 weeks is mandatory to confirm complete expulsion (clinical assessment + ultrasound if incomplete is suspected). The woman must be counselled about expected cramping, bleeding (heavier than a period for 1–2 weeks), and the signs of incomplete abortion or infection that warrant immediate return.
Manual Vacuum Aspiration (MVA): MVA uses a hand-held syringe-based vacuum aspirator (Karman cannula, 4–12 mm) to evacuate the uterine contents under local paracervical block as an outpatient procedure. It is effective from 6 to 12–14 weeks and is the WHO-preferred surgical method for early first-trimester termination in resource-limited settings. Advantages include no need for general anaesthesia, low complication rate, and immediate verification of complete evacuation. Electric Vacuum Aspiration (EVA), using an electric pump, is the hospital equivalent with similar indications and efficacy.
Sharp curettage (D&C): Dilatation and curettage, once the standard surgical method, is now considered obsolete by WHO and FOGSI for first-trimester MTP due to higher complication rates (perforation, Asherman syndrome) compared with vacuum aspiration. It should be used only when vacuum aspiration is unavailable.
Provided image
SELF-CHECK
A 26-year-old woman at 8 weeks of gestation opts for medical MTP. Which regimen is currently recommended by MoHFW?
A. Methotrexate 50 mg/m² IM followed by misoprostol 800 mcg vaginally after 3–7 days
B. Mifepristone 600 mg orally followed immediately by misoprostol 400 mcg orally
C. Mifepristone 200 mg orally followed 24–48 hours later by misoprostol 800 mcg sublingually/vaginally
D. Misoprostol 800 mcg vaginally alone, repeated every 3 hours for up to 3 doses
Reveal Answer
Answer: C. Mifepristone 200 mg orally followed 24–48 hours later by misoprostol 800 mcg sublingually/vaginally
The MoHFW/WHO-approved combination for first-trimester medical MTP is mifepristone 200 mg orally followed 24–48 hours later by misoprostol 800 mcg (sublingual, vaginal, or buccal route). Methotrexate-misoprostol is used in some countries but is not the Indian standard. Higher doses of mifepristone (600 mg) are not more effective and are more costly. Misoprostol alone is less effective than the combination.
Second-Trimester MTP: Methods and Considerations
Second-trimester MTP (13–24 weeks) is technically more complex, carries higher maternal morbidity, and requires a higher-level facility with access to surgical backup, blood transfusion services, and appropriate anaesthesia. It is indicated when first-trimester termination was not sought or not possible — for instance, because the pregnancy was concealed, because the woman lacked access to services, or because a significant foetal anomaly was identified only at the anomaly scan (performed routinely at 18–20 weeks in India). Under the MTP (Amendment) Act 2021, second-trimester termination is now explicitly lawful up to 24 weeks for the specified categories enumerated in Rule 3B. The key clinical challenge in second-trimester MTP is balancing the effectiveness of the procedure, the safety of the woman, and the availability of trained personnel and facilities. Because the uterus is larger, the cervix requires more preparation, blood loss potential is higher, and the psychological burden on the woman and the care team is greater — all of these factors inform method selection.
Medical methods for second trimester:
- Mifepristone followed by high-dose misoprostol: For 13–20 weeks, the current FOGSI/WHO protocol uses mifepristone 200 mg orally, followed 24–48 hours later by misoprostol 400 mcg vaginally or sublingually every 3–6 hours (maximum 5 doses). Induction-to-abortion interval is typically 8–16 hours. Efficacy is >90% within 24 hours.
- Misoprostol alone (without mifepristone): Used where mifepristone is unavailable. Doses are higher and intervals more frequent, with longer induction time. This approach is less efficient but acceptable.
- Extra-amniotic instillation (Ethacridine lactate / Rivanol): A catheter is placed through the cervix into the extra-amniotic space and ethacridine lactate is instilled. This method was widely used in India before the availability of misoprostol; it has a slower onset (24–48 h) and higher infection risk, and is now largely replaced by prostaglandin protocols.
Surgical methods for second trimester:
- Dilatation and Evacuation (D&E): The standard surgical method at 13–20 weeks in settings with trained providers. Requires mechanical cervical priming (osmotic dilators — Dilapan-S or Laminaria, or misoprostol 400 mcg 3–4 h before) to safely dilate the cervix to 14–20 mm. D&E under general/regional anaesthesia by a trained operator has a lower complication rate than medical induction in expert hands but is highly operator-dependent. Not universally available in India.
- Feticide before D&E: For gestational ages approaching or exceeding 20 weeks where foetal cardiac activity may be detected after evacuation, intracardiac digoxin or potassium chloride is used prior to the surgical procedure in some protocols.
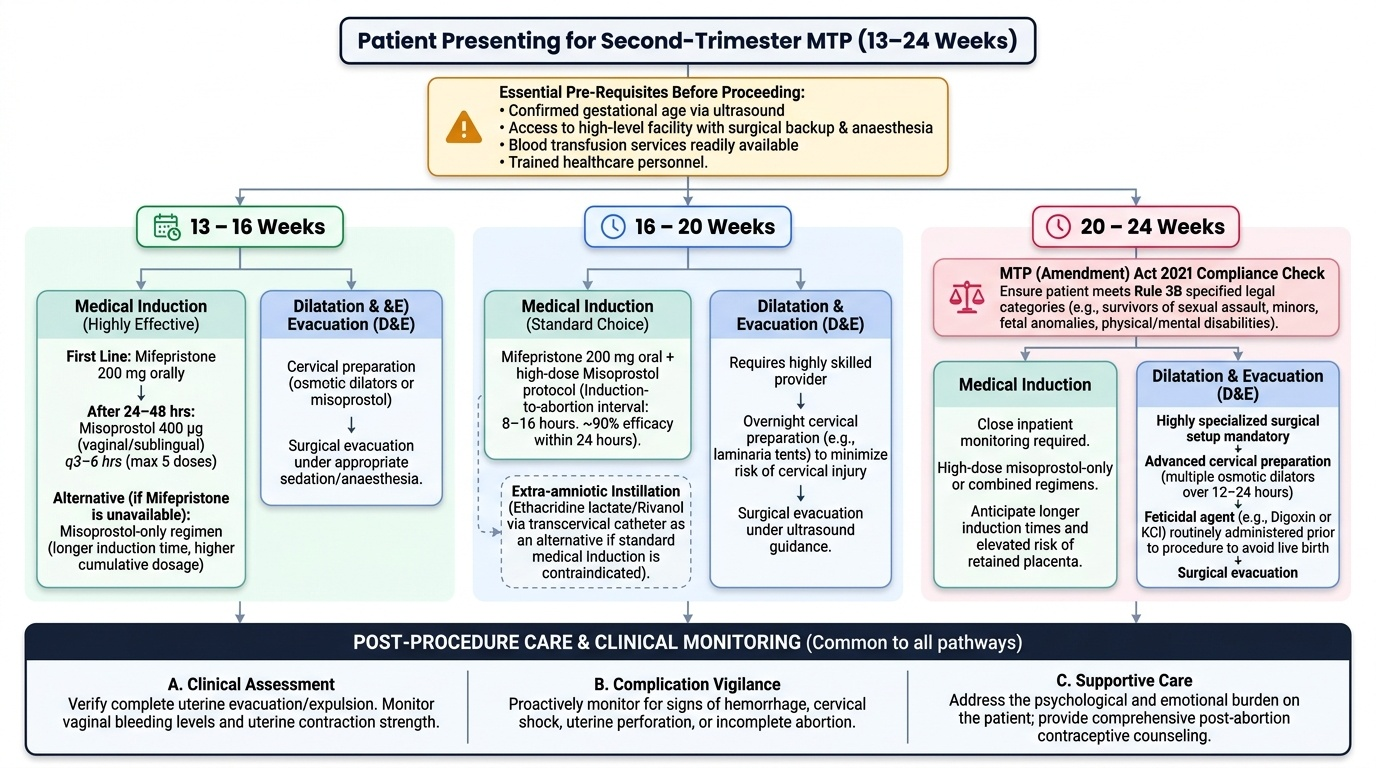
Provided image
The choice of method in the second trimester depends on: operator training and facility capacity, gestational age, urgency, patient preference, and availability of mifepristone. Medical methods are preferred in most Indian settings due to lower operator-skill demands. All second-trimester procedures should be performed in a hospital with access to blood transfusion, surgical backup, and intensive care.
SELF-CHECK
A woman at 17 weeks with a confirmed foetal anomaly incompatible with life requires MTP. Which of the following methods is currently preferred in most Indian hospital settings?
A. Extra-amniotic ethacridine lactate instillation
B. Sharp curettage (D&C) under general anaesthesia
C. Mifepristone followed by vaginal/sublingual misoprostol
D. Hysterotomy as it is most reliable at this gestation
Reveal Answer
Answer: C. Mifepristone followed by vaginal/sublingual misoprostol
For second-trimester MTP at 13–20 weeks, the mifepristone + high-dose misoprostol protocol is the preferred medical method in most Indian hospitals. Ethacridine lactate is older, slower, and has higher infection risk. Sharp curettage is obsolete for first-trimester and not appropriate here. Hysterotomy is only for cases where vaginal delivery is unsafe.