Page 3 of 28
OG20.1 | Medical Termination of Pregnancy — SDL Guide (Part 3)
Complications of MTP and Their Management
Complications of MTP are uncommon when the procedure is performed by trained providers in appropriate settings, but they are life-threatening when they occur in clandestine or unskilled hands. Recognising and managing complications promptly is a core clinical skill.
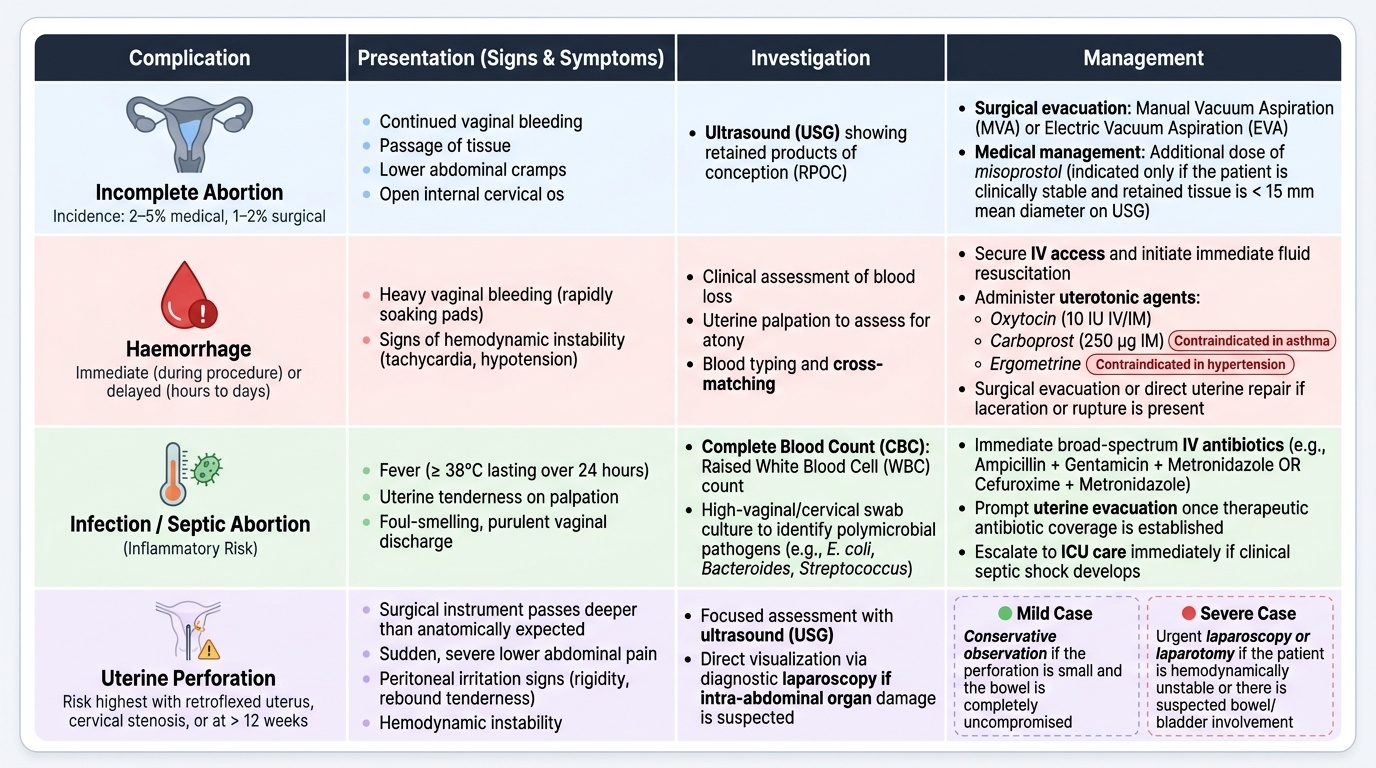
Incomplete abortion is the most common complication, occurring in approximately 2–5% of medical MTPs and 1–2% of surgical MTPs. It presents with continued bleeding, passage of tissue, lower abdominal cramps, and an open internal cervical os. Ultrasound typically shows retained products of conception. Management is surgical evacuation (MVA or EVA) or additional misoprostol if the woman is stable and the retained tissue is small (< 15 mm mean diameter on USG).
Haemorrhage may be immediate (during the procedure) or delayed (hours to days after). Causes include incomplete evacuation, uterine atony, uterine perforation, or — rarely — placenta praevia in mid-trimester cases. Management: secure IV access, cross-match blood, uterotonic agents (oxytocin 10 IU IV/IM; note: ergometrine is contraindicated in hypertension; carboprost 250 mcg IM is effective but contraindicated in asthma), surgical evacuation or repair as needed.
Uterine perforation occurs in < 1% of surgical evacuations; risk is highest in an anteverted retroflexed uterus, with cervical stenosis, or at >12 weeks. Signs: instrument passes in unexpectedly, haemodynamic instability, peritoneal signs. Management: if small and uncompromised bowel, conservative observation; if haemodynamically significant or bowel involved, laparoscopy or laparotomy.
Septic abortion (post-procedure infection) presents with fever (>38°C for >24 h), uterine tenderness, purulent discharge, and raised WBC. Organisms: polymicrobial (E. coli, Bacteroides, Streptococcus). Management: broad-spectrum IV antibiotics (ampicillin + gentamicin + metronidazole; or cefuroxime + metronidazole), uterine evacuation once antibiotics are started, ICU care in septic shock.
Failed MTP (continuing pregnancy): Medical MTP fails in approximately 3–5%; surgical MTP failure is rare (< 1%). A follow-up ultrasound at 2 weeks confirms outcome. A continuing or viable pregnancy after medical MTP requires repeat medical dose or surgical evacuation.
Cervical / vaginal laceration: Usually minor at the tenaculum site; managed with pressure or suture.
Provided image
SELF-CHECK
A woman returns 5 days after a medical MTP with fever 39°C, foul-smelling vaginal discharge, and uterine tenderness. Ultrasound confirms retained products. The most appropriate immediate management is:
A. Broad-spectrum IV antibiotics followed by uterine evacuation once afebrile for 24 h
B. Broad-spectrum IV antibiotics AND uterine evacuation without waiting to become afebrile
C. Oral antibiotics for 7 days followed by outpatient aspiration
D. Repeat dose of misoprostol to complete the evacuation before starting antibiotics
Reveal Answer
Answer: B. Broad-spectrum IV antibiotics AND uterine evacuation without waiting to become afebrile
Septic abortion with retained products requires broad-spectrum IV antibiotics (ampicillin + gentamicin + metronidazole) AND uterine evacuation. Waiting for the patient to become afebrile before evacuating the septic focus is incorrect — the focus must be removed to clear the infection. The combination of antibiotics + evacuation reduces mortality. Repeat misoprostol without antibiotics risks worsening sepsis.
CLINICAL PEARL
The MTP Rules 2021 introduced two practice-changing provisions that are regularly tested: (1) Up to 20 weeks, one RMP opinion is now sufficient (the earlier 12-week one-doctor threshold has been replaced by a uniform 20-week limit); and (2) the 20–24-week category requires two RMPs AND the woman must belong to a specified category (Rule 3B). A request at 21 weeks from a survivor of rape requires two RMP opinions — not a Medical Board. The Medical Board pathway is reserved for gestations beyond 24 weeks where substantial foetal abnormality is the indication. Getting these tiers right in a viva or OSCE is non-negotiable.
Self-Assessment
You have now covered the full scope of MTP as required by competency OG20.1 — the legal framework under the 1971 Act and 2021 amendment, the gestational-tier structure, the pre-procedure eligibility workup, and both first- and second-trimester methods and their complications. The questions below are designed to test your ability to apply this knowledge in clinical scenarios rather than simply recite facts. These are the types of scenarios you will encounter in OSCE stations, viva voce examinations, and in clinical practice as a junior doctor or intern. Work through each scenario before checking the answer. Pay particular attention to the questions on gestational tiers, uterotonic contraindications, and management of complications — these three areas account for the majority of marks in this competency.
- A 15-year-old minor presents at 22 weeks with a request for MTP after sexual assault. How many RMP opinions are needed, and under which provision of the MTP Rules 2021 does she qualify?
- Enumerate four indications for MTP under the MTP Act 1971 (amended 2021).
- A woman is given mifepristone 200 mg and returns 36 hours later for misoprostol. She is found to be 11 weeks pregnant on ultrasound (miscalculated earlier). How does this change your management?
- Describe the first-line management of haemorrhage complicating a second-trimester MTP in a woman with a history of bronchial asthma. Which uterotonic is contraindicated?
- A woman returns 10 days after medical MTP with no further bleeding and no passage of tissue. Ultrasound shows a gestational sac still in situ with a fetal heartbeat. What is the next step?
Answers:
1. Two RMP opinions are required; she qualifies under Rule 3B of MTP Rules 2021 (minor, and rape/sexual assault survivor — dual grounds).
2. Risk to life or physical/mental health of the woman; foetal anomaly/handicap; failure of contraception (in a married woman or by 2021 amendment — unmarried women too); specified categories 20–24 weeks (rape, minor, marital-status change, disability, foetal malformation, humanitarian).
3. At 11 weeks, the medical method has reduced efficacy and the mifepristone has already been given. Options: proceed with misoprostol (with higher dose/repeat dosing per second-trimester protocol — 11 weeks is borderline), or counsel for surgical evacuation (MVA). The woman should be informed of the higher failure rate at this gestation.
4. Secure IV access, oxytocin 10 IU IV/IM (first-line); ergometrine contraindicated if hypertension is present. Carboprost (PGF2α) is contraindicated in bronchial asthma. Use tranexamic acid; prepare for surgical management if bleeding persists.
5. This is a failed medical MTP with a continuing pregnancy. The patient should be counselled about the failure, foetal risk from prior misoprostol exposure, and given the choice of repeat medical MTP (additional misoprostol) or surgical evacuation (MVA/EVA). Continuing the pregnancy is also her right, but she must be informed of the potential teratogenic risk of misoprostol (limb defects, Möbius syndrome).