Page 15 of 22
OG25.1 | Amenorrhea — SDL Guide (Part 2)
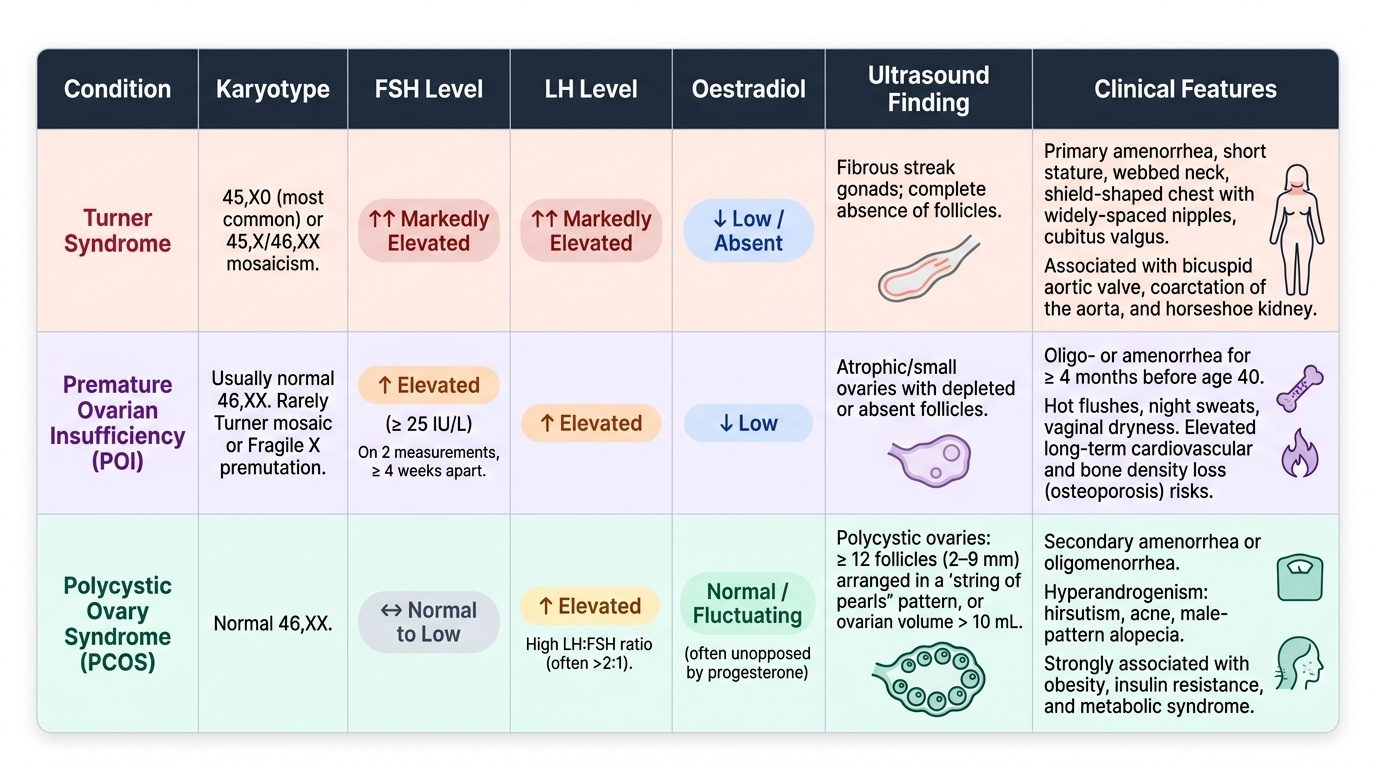
Ovarian Causes
Ovarian failure and ovarian dysfunction produce amenorrhea through distinct hormonal mechanisms, and the pattern of gonadotrophin levels is key to distinguishing them.
Turner syndrome (gonadal dysgenesis, 45X0) is the most important chromosomal cause of primary amenorrhea. The majority have a 45X0 karyotype, though mosaicism (45X/46XX) is common and may allow partial ovarian function. The ovaries are replaced by fibrous streak gonads that produce no oestradiol, so the pituitary is uninhibited and FSH and LH are markedly elevated (hypergonadotrophic hypogonadism). The absence of oestrogen means secondary sexual characteristics fail to develop. Classic somatic features include short stature, webbed neck (pterygium colli), low posterior hairline, shield-shaped chest, widely-spaced nipples, and cubitus valgus. Cardiac anomalies (bicuspid aortic valve, coarctation) and horseshoe kidney are associated. Management involves oestrogen replacement to induce puberty and protect bone density, with subsequent cyclical progestogen; fertility with own oocytes is not possible, but donor egg IVF is an option.
Premature ovarian insufficiency (POI) — previously termed premature menopause — is defined as ovarian failure before the age of 40 years. The diagnostic criterion is FSH >25 IU/L on two measurements at least 4 weeks apart, accompanied by oligo- or amenorrhea for ≥4 months. The causes include chromosomal (Turner mosaic, Fragile X premutation carriers), autoimmune (associated with autoimmune thyroiditis, Addison disease), iatrogenic (chemotherapy, pelvic radiotherapy, oophorectomy), and idiopathic (the majority). Unlike natural menopause, POI is associated with elevated cardiovascular risk, bone density loss, sexual dysfunction, and potential psychological distress — all of which require active management with hormone replacement therapy (HRT) until the average age of natural menopause (approximately 51 years). Spontaneous pregnancy is possible (5–10% chance over time), so contraception is not always needed but fertility counselling is mandatory.
Provided image
Polycystic ovary syndrome (PCOS) causes secondary amenorrhea (or oligomenorrhea) through chronic anovulation rather than ovarian failure. The HPO axis is active but dysregulated: elevated tonic LH (LH:FSH ratio often >2:1), excess ovarian androgen production (causing hirsutism, acne), and failure of dominant follicle selection. The Rotterdam 2003 criteria (revised 2012) require 2 of 3: (1) oligo- or anovulation, (2) clinical or biochemical hyperandrogenism, (3) polycystic ovarian morphology on ultrasound (≥20 follicles per ovary or ovarian volume >10 mL in the absence of a dominant follicle or corpus luteum). Unlike POI, the FSH is normal or mildly low, oestradiol is normal, and the patient is not hypoestrogenic — therefore there is no increased fracture risk from the amenorrhea itself, though metabolic risks (insulin resistance, type 2 diabetes, dyslipidaemia, endometrial hyperplasia) are prominent.
Pituitary and Hypothalamic Causes
The pituitary and hypothalamic causes of amenorrhea share a common hormonal signature — hypogonadotrophic hypogonadism — characterised by low or inappropriately normal FSH and LH with low oestradiol. The clinician must determine whether the defect is at the level of the pituitary or hypothalamus, as the treatments differ substantially.
Prolactinoma is the commonest pituitary tumour in women of reproductive age and the commonest pituitary cause of amenorrhea. Excess prolactin suppresses GnRH pulsatility at the hypothalamus, thereby inhibiting FSH and LH release and creating a functional hypogonadotrophic state. The clinical presentation is the amenorrhea-galactorrhoea syndrome — the triad of amenorrhea, galactorrhoea (spontaneous or expressible milky nipple discharge in the absence of pregnancy), and low oestrogen symptoms. Prolactin levels >20–25 ng/mL are abnormal; values >100 ng/mL are highly suggestive of a macroadenoma (>10 mm). A microadenoma (<10 mm) typically causes levels in the 25–200 ng/mL range. Investigation requires serum prolactin, followed by pituitary MRI if elevated. It is critical to first exclude hypothyroidism as a secondary cause of hyperprolactinaemia: elevated TRH (due to low thyroid hormone) stimulates both TSH and prolactin release — therefore TSH must be checked alongside prolactin in every amenorrhea workup. If TSH is elevated, treating the hypothyroidism may normalise prolactin and restore menstruation. Management of prolactinoma is primarily with dopamine agonists (cabergoline preferred over bromocriptine for better tolerability) — these suppress prolactin, shrink the adenoma, and restore ovulatory cycles in most women within weeks.
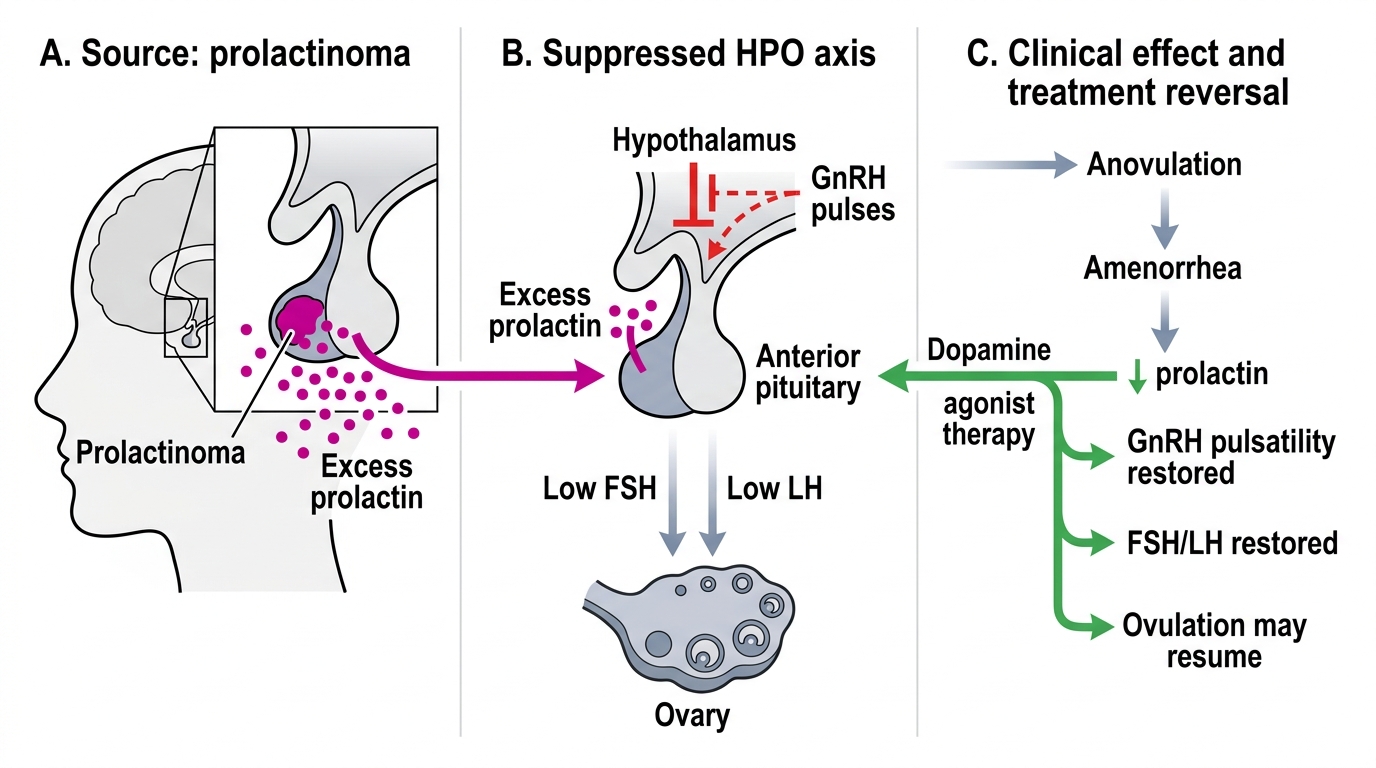
Hyperprolactinaemia Suppression of the HPO Axis
Sheehan syndrome (postpartum pituitary necrosis) results from ischaemic infarction of the anterior pituitary following massive postpartum haemorrhage, typically when hypotensive shock causes vascular spasm in the already-enlarged gland. The anterior pituitary has no collateral circulation and is therefore uniquely vulnerable. Clinically, the classic presentation is failure of lactation (prolactin deficiency) in the immediate postpartum period, followed over months to years by variable anterior pituitary hormone deficiency — amenorrhea (from gonadotrophin deficiency), hypothyroidism (TSH deficiency), adrenal insufficiency (ACTH deficiency), and diabetes insipidus (posterior pituitary may also be affected). The degree of deficiency correlates with the extent of infarction — partial Sheehan gives partial hypopituitarism. Diagnosis is by low random serum cortisol, pituitary hormone panel, and pituitary MRI (empty sella or partially empty sella). Management is lifelong hormone replacement for each deficient axis.
Functional hypothalamic amenorrhea (FHA) is caused by suppression of GnRH pulsatility by psychological or metabolic stressors — specifically energy deficit (weight loss, eating disorders such as anorexia nervosa), excessive exercise (female athlete triad: low energy availability, menstrual dysfunction, reduced bone mineral density), and psychological stress. The net result is low LH pulse frequency, low FSH, low oestradiol, and no ovulation. The hormonal picture is indistinguishable from hypogonadotrophic hypogonadism from an organic cause, but a detailed history usually reveals the precipitating factor. FHA is a diagnosis of exclusion after organic pituitary pathology has been ruled out. The Endocrine Society guideline (2017) emphasises that the primary treatment is cognitive behavioural therapy (CBT) and nutritional rehabilitation (weight restoration and normalisation of energy availability), not hormone treatment — because exogenous hormones do not restore the underlying GnRH axis and do not restore bone density as effectively as weight restoration does. Oestrogen supplementation (transdermal route preferred for bone health) is appropriate if FHA persists despite lifestyle optimisation.
SELF-CHECK
A 26-year-old woman presents with secondary amenorrhea and galactorrhoea for 6 months. Her serum prolactin is 45 ng/mL. The NEXT most important investigation before attributing this to a prolactinoma is:
A. Pituitary MRI
B. Serum FSH and LH
C. Serum TSH
D. Serum oestradiol
Reveal Answer
Answer: C. Serum TSH
Elevated prolactin can be secondary to primary hypothyroidism — elevated TRH stimulates both TSH and prolactin. TSH must be checked BEFORE pituitary MRI. If TSH is elevated, treating hypothyroidism may normalise prolactin and restore cycles without any pituitary intervention. Proceeding to MRI before excluding this reversible cause wastes resources and may lead to unnecessary investigation or treatment. FSH/LH and oestradiol are also part of the workup but are not the most critical next step to distinguish primary pituitary prolactinoma from hypothyroidism-induced hyperprolactinaemia.
Systematic Investigation Approach
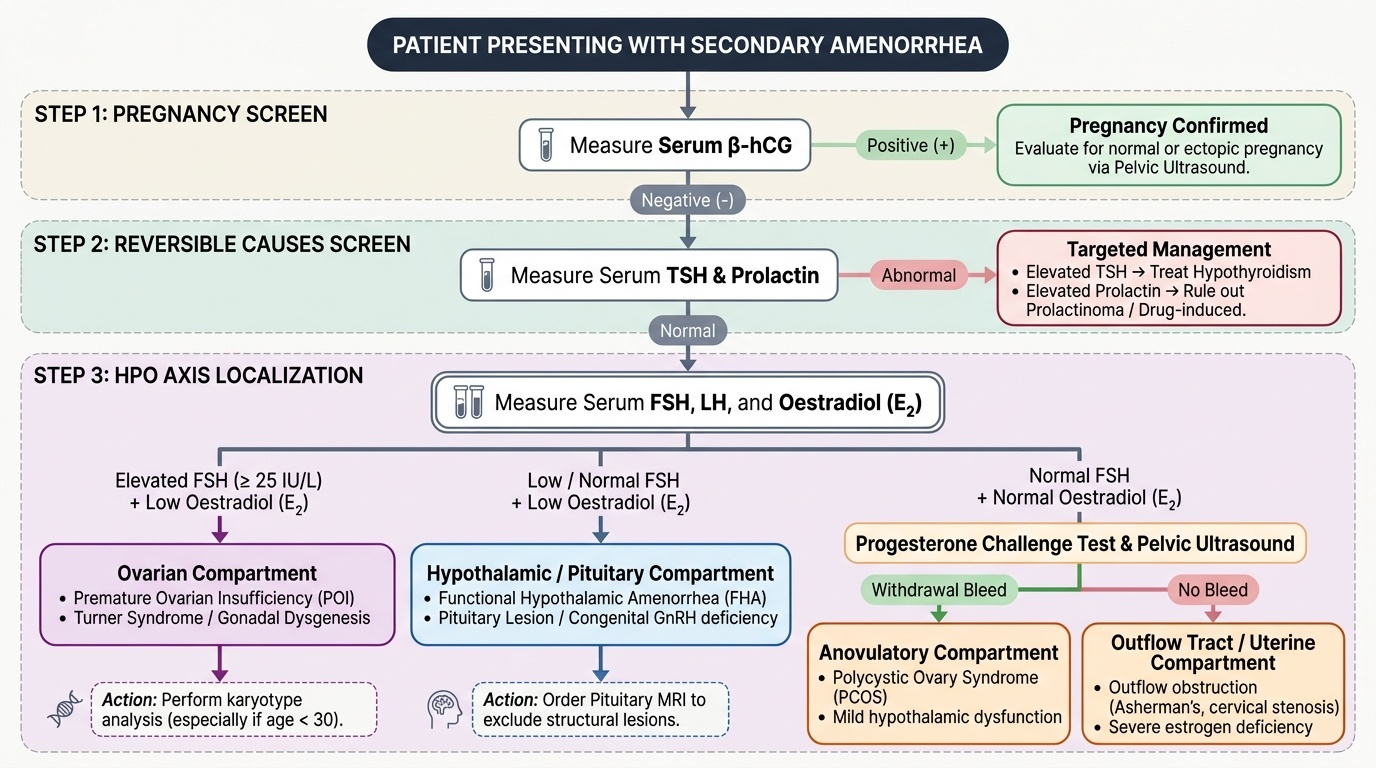
The investigation of amenorrhea is most efficient when it follows a systematic, stepwise algorithm that confirms or excludes pregnancy first, then localises the compartment with targeted hormonal tests before proceeding to imaging.
Step 1 — Exclude pregnancy: serum β-hCG. This is non-negotiable. Pregnancy is the commonest cause of secondary amenorrhea in women of reproductive age. A positive β-hCG ends the amenorrhea workup; an ectopic pregnancy must be excluded by ultrasound. All subsequent investigations are ordered only after pregnancy is excluded.
Step 2 — Exclude common reversible causes: serum TSH and prolactin. As detailed above, hypothyroidism elevates both TSH and prolactin and is readily treated. Hyperprolactinaemia (without hypothyroidism) suggests a prolactinoma or other pituitary cause. These tests are cheap, widely available, and identify two common, treatable causes before expensive imaging.
Step 3 — Assess the HPO axis: serum FSH, LH, and oestradiol. The result pattern localises the compartment:
- FSH elevated (>25 IU/L) + low oestradiol = hypergonadotrophic hypogonadism → ovarian cause (POI, Turner, gonadal dysgenesis). Obtain karyotype in all cases, especially in women under 30.
- FSH low/normal + low oestradiol = hypogonadotrophic hypogonadism → hypothalamic (FHA) or pituitary cause. Obtain pituitary MRI to exclude a structural lesion.
- FSH normal + normal oestradiol (normogonadotrophic) → outflow/uterine cause or PCOS. Proceed to progesterone challenge and ultrasound.
- FSH normal + LH elevated + normal/elevated androgens → PCOS pattern (check free testosterone, DHEAS).
Step 4 — The progesterone challenge test. This tests for: (a) the presence of oestrogen-primed endometrium, and (b) a patent outflow tract. Administer progesterone (medroxyprogesterone acetate 10 mg daily × 5–10 days, or equivalent). A withdrawal bleed within 2–7 days = positive challenge — confirms that the endometrium is oestrogen-primed and the outflow is patent; the amenorrhea is anovulatory (PCOS is the most likely diagnosis). No bleed = either the endometrium is not adequately primed (hypo-oestrogenic state) or the outflow/uterus is obstructed. To distinguish these, follow a negative challenge with an oestrogen-progesterone sequential challenge: administer oestrogen for 21 days then add progesterone for the last 5–10 days. A bleed after this = intact outflow, hypo-oestrogenic state (hypothalamic, pituitary, or ovarian cause). Still no bleed = outflow/uterine obstruction (Asherman, stenosis, MRKH).
Provided image
Step 5 — Pelvic ultrasound. Visualises uterine anatomy (presence/absence, cavity, adhesions), ovarian morphology (PCO pattern: ≥20 follicles or volume >10 mL), and any pelvic mass. MRI provides superior anatomical detail when uterine anomaly or pituitary pathology needs characterisation.
Step 6 — Karyotype. Mandatory in: all primary amenorrhea cases, all women with hypergonadotrophic hypogonadism before age 30 (Turner mosaic, Fragile X premutation), and absent uterus (MRKH vs CAIS distinction). Additional tests as directed by the clinical picture: bone density (DEXA) in hypo-oestrogenic states, thyroid antibodies, adrenal antibodies (if POI with autoimmune screen needed).
SELF-CHECK
A 22-year-old woman has secondary amenorrhea for 5 months. Beta-hCG is negative. Serum TSH, prolactin, FSH, LH, and oestradiol are all within normal limits. A progesterone challenge (medroxyprogesterone acetate 10 mg × 10 days) produces NO withdrawal bleed. Subsequent oestrogen-progesterone sequential challenge ALSO produces no bleed. What is the most likely diagnosis?
A. Functional hypothalamic amenorrhea
B. Polycystic ovary syndrome
C. Asherman syndrome (intrauterine adhesions)
D. Premature ovarian insufficiency
Reveal Answer
Answer: C. Asherman syndrome (intrauterine adhesions)
Normal FSH, LH, prolactin, TSH, and oestradiol exclude hypo-oestrogenic and pituitary/hypothalamic causes. A positive progesterone challenge would point to PCOS (anovulatory, oestrogen primed). A negative progesterone challenge with ALSO no bleed after combined oestrogen-progesterone confirms that the outflow tract or endometrium is unresponsive — this is the pattern of Asherman syndrome (intrauterine adhesions). FHA and POI would both show low oestradiol and bleed on the combined challenge. PCOS would bleed on progesterone challenge alone.