Page 16 of 22
OG25.1 | Amenorrhea — SDL Guide (Part 3)
Principles of Management by Cause
Management of amenorrhea is almost entirely cause-specific. There is no single treatment for 'amenorrhea' — rather, the compartment diagnosis directs the intervention. Three overarching goals apply regardless of aetiology: first, treat the underlying cause where this is possible (shrink a prolactinoma, restore body weight, perform hysteroscopic adhesiolysis, induce ovulation); second, restore the hormonal milieu to protect long-term health — because prolonged hypoestrogenism from any cause is not merely a menstrual inconvenience but carries serious downstream consequences including osteoporosis, increased cardiovascular risk, genitourinary atrophy, and impaired cognitive health; and third, provide accurate and sensitive counselling on fertility and reproductive options, since many of these diagnoses have profound implications for a young woman's reproductive future. The clinician who only restores periods without addressing bone density or fertility expectations has delivered incomplete care. What follows is a cause-structured summary; each management recommendation is tied back to the compartment logic established in the earlier sections.
Outflow/Uterine causes:
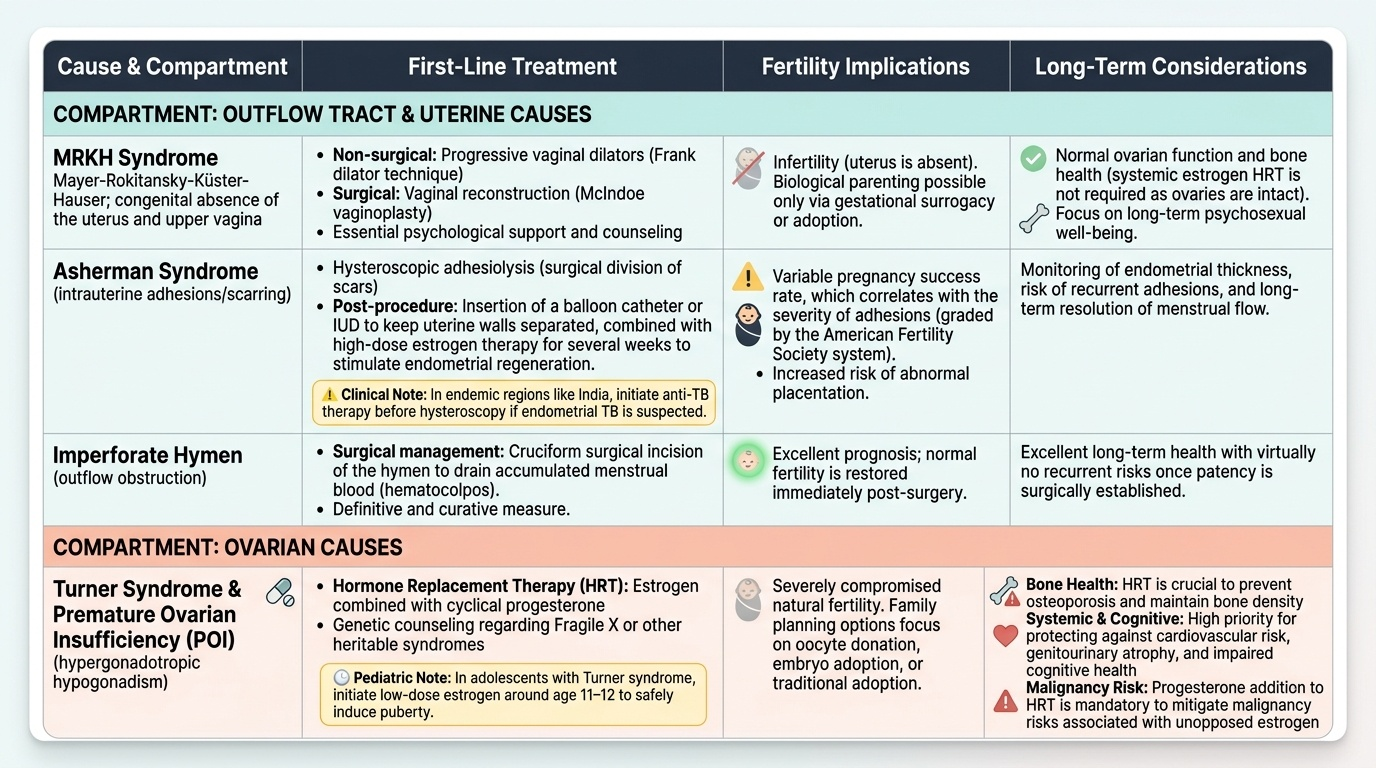
- MRKH syndrome: the uterus cannot be created; fertility with own uterus is not possible. Vaginal construction (progressive vaginal dilators — the Frank dilator technique — or surgical vaginoplasty such as McIndoe procedure) allows sexual function. Genetic counselling regarding Fragile X or other heritable syndromes if applicable. Psychological support and counselling are essential.
- Asherman syndrome: hysteroscopic adhesiolysis is the definitive treatment. Post-procedure, the uterine cavity is maintained with a balloon or IUD and high-dose oestrogen is prescribed for several weeks to stimulate endometrial regeneration. Subsequent pregnancy rates are variable and correlate with severity of adhesions (the American Fertility Society grading system). In India, anti-TB therapy should be started before hysteroscopy if endometrial TB is suspected.
- Imperforate hymen: cruciform surgical incision to create an opening; definitive and curative.
Ovarian causes:
- Turner syndrome and POI: HRT (oestrogen and cyclical progesterone) is the cornerstone of management. In adolescents with Turner syndrome, oestrogen is started at low doses around age 11–12 to induce puberty gradually. HRT is continued until the age of natural menopause (approximately 50 years) to protect bone mineral density and cardiovascular health. Annual DEXA scan and cardiac surveillance (for aortic dilatation) are part of ongoing care. Fertility with own oocytes is rarely possible; donor oocyte IVF is the main fertility option.
- PCOS: management is individualised by the primary complaint — if the concern is irregular cycles and no fertility desire, the combined oral contraceptive pill (OCP) regulates cycles and reduces androgen levels. If fertility is desired, ovulation induction with clomiphene citrate (first-line) or letrozole (increasingly preferred) is used. Metformin improves insulin sensitivity and may restore ovulation in insulin-resistant PCOS. Weight loss (even 5–10% in overweight patients) significantly improves ovulatory function. Long-term management must address metabolic risks (annual glucose, lipids).
Pituitary causes:
- Prolactinoma: dopamine agonists (cabergoline 0.25–0.5 mg twice weekly; or bromocriptine 1.25–2.5 mg twice daily) suppress prolactin, cause tumour shrinkage, and restore menstrual cycles. Surgery (transsphenoidal resection) is reserved for dopamine agonist intolerance or non-response, large tumours with visual field defects, and pregnancy complications. If the patient desires pregnancy, dopamine agonist normalises prolactin and restores ovulation in >90% of microadenoma cases.
- Sheehan syndrome: lifelong hormone replacement for each deficient axis — thyroxine, hydrocortisone (most critical first — adrenal crisis is life-threatening), and sex steroids (oestrogen/progesterone). Desmopressin if posterior pituitary affected. Growth hormone if symptomatic.
Hypothalamic causes:
- Functional hypothalamic amenorrhea (FHA): primary treatment is nutritional rehabilitation and resolution of the energy deficit; CBT for eating disorders and psychological stress. Sports medicine input for the female athlete triad. Oestrogen replacement (transdermal preferred to oral — avoids first-pass hepatic IGF-1 suppression that impairs bone density) if amenorrhea persists despite lifestyle change. Fertility: pulsatile GnRH (where available) or gonadotrophin injections for ovulation induction, only after energy status is restored.
Provided image
A universal principle: prolonged hypo-oestrogenism from any cause carries a risk of osteoporosis — advise calcium (1000–1200 mg/day) and vitamin D supplementation and arrange DEXA scanning in all patients with established hypoestrogenic amenorrhea of more than 6–12 months. An additional principle specific to the uterus: endometrial protection — in any woman with a uterus who receives oestrogen therapy, cyclical progestogen or levonorgestrel-IUS is mandatory to prevent endometrial hyperplasia and cancer.
CLINICAL PEARL
The progesterone challenge test is a powerful, low-cost clinical tool — but its interpretation requires the two-stage logic. A negative challenge (no bleed) does NOT immediately mean the uterus is absent or scarred. It means either the endometrium was not adequately primed by oestrogen (hypo-oestrogenic state — hypothalamic, pituitary, or ovarian cause) OR there is an outflow/uterine problem. Only the sequential oestrogen-progesterone challenge distinguishes these: a bleed after the combined challenge points to hypo-oestrogenism (endometrium can respond when given oestrogen, and outflow is patent); no bleed even after combined challenge = endometrium or outflow is irreversibly non-functional (Asherman, MRKH, AIS, stenosis). Many students forget the second-stage challenge and jump straight to a diagnosis of outflow obstruction after the first negative test — always complete both stages before concluding.
A second pearl: never start a workup for amenorrhea without first checking a serum β-hCG. Pregnancy is the most common cause of secondary amenorrhea, even in women who believe they cannot be pregnant. Missing an ectopic pregnancy while investigating hypothalamic amenorrhea is a dangerous error.
Self-Assessment: Integrating Amenorrhea Workup
At this stage in the module you have covered all four compartments, the hormonal signatures that distinguish them, the stepwise investigation algorithm, and the cause-specific management principles. The self-assessment scenarios below are designed to consolidate that learning by asking you to work through a clinical vignette and localise the compartment before arriving at a diagnosis and management plan. This is the skill that underpins the NMC OG25.1 competency at the KH level — knowing the facts is necessary but not sufficient; you must be able to apply compartment logic to a real or simulated patient encounter. For each scenario, read the clinical details, interpret the hormonal investigations using the patterns you have learned, apply the progesterone-challenge two-stage logic where relevant, and arrive at the diagnosis before reading the analysis. The reference table below summarises the four compartment hormonal patterns as a self-check anchor.

Provided image
Scenario A: A 28-year-old woman has no periods for 7 months after resuming training as a competitive long-distance runner following a 2-year break. She has lost 7 kg over the past year. Serum β-hCG: negative. TSH: normal. Prolactin: normal. FSH: 4 IU/L (low). LH: 3 IU/L (low). Oestradiol: 40 pmol/L (low). Progesterone challenge: no withdrawal bleed. Oestrogen-progesterone challenge: withdrawal bleed present. What is the diagnosis and first-line treatment?
Analysis: Low FSH and LH with low oestradiol = hypogonadotrophic hypogonadism. History of weight loss and intense exercise. Normal prolactin and TSH exclude pituitary and thyroid causes. Bleed on the combined challenge confirms intact outflow tract and a functional but oestrogen-deprived endometrium. Diagnosis: functional hypothalamic amenorrhea (FHA) due to energy deficit from training load and weight loss. First-line treatment: nutritional rehabilitation (increase energy intake), reduction of training volume, psychological support/CBT. Oestrogen replacement if amenorrhea persists.
Scenario B: A 32-year-old woman has had no periods for 10 months. She had two D&C procedures for incomplete miscarriage 12 months ago. Serum β-hCG: negative. All hormone levels (TSH, prolactin, FSH, LH, oestradiol) are within normal limits. Progesterone challenge: no bleed. Oestrogen-progesterone challenge: no bleed. What is the diagnosis and recommended investigation?
Analysis: Normal hormonal profile = outflow/uterine compartment problem. History of uterine instrumentation. Negative both challenges = non-responsive endometrium or obstructed outflow. Diagnosis: Asherman syndrome. Recommended investigation: hysteroscopy (diagnostic + therapeutic — adhesiolysis).
Scenario C: A 38-year-old woman presents with hot flushes, irregular periods for 6 months, and one period in the past 3 months. Her mother had early menopause. β-hCG negative. TSH normal. Prolactin normal. FSH: 42 IU/L. LH: 35 IU/L. Oestradiol: 55 pmol/L (low). What is the diagnosis and what additional test is indicated?
Analysis: Hypergonadotrophic hypogonadism (high FSH and LH, low oestradiol) with hot flushes in a 38-year-old = premature ovarian insufficiency (POI). Confirm: repeat FSH in 4 weeks (must be >25 IU/L on two occasions ≥4 weeks apart). Additional tests: karyotype (especially if <30 years — to detect Turner mosaic or Fragile X permutation), autoimmune screen (TPO antibodies, adrenal antibodies), DEXA scan. Management: HRT until age 50–51, fertility counselling (donor oocyte IVF).
SELF-CHECK
A 38-year-old woman with secondary amenorrhea has serum FSH 46 IU/L and FSH 43 IU/L on repeat testing 5 weeks later. Her LH is 38 IU/L, oestradiol is low, and prolactin and TSH are normal. She has hot flushes and vaginal dryness. What is the most appropriate long-term management?
A. Dopamine agonist therapy with cabergoline
B. Combined oral contraceptive pill to regulate cycles
C. Hormone replacement therapy with oestrogen and cyclical progestogen until age 50–51
D. Clomiphene citrate for ovulation induction
Reveal Answer
Answer: C. Hormone replacement therapy with oestrogen and cyclical progestogen until age 50–51
This is premature ovarian insufficiency (POI) — elevated FSH on two occasions, low oestradiol, age 38. The appropriate management is hormone replacement therapy (HRT) with oestrogen plus cyclical progestogen (to protect the endometrium) continued until the average age of natural menopause (~50–51 years). This is important for bone density, cardiovascular health, and quality of life. Dopamine agonists are for prolactinoma. COC can be used but HRT is preferred in POI for its physiological replacement approach and more favourable safety profile. Clomiphene is for ovulation induction in PCOS — there is no functional ovarian tissue to stimulate in POI.