Page 1 of 22
OG23.1 | Normal and Abnormal Puberty — SDL Guide
Learning Objectives
- Describe the hormonal physiology of puberty including the HPO axis, GnRH pulse activation, and gonadotrophin secretion
- Apply the Tanner staging system to classify breast development and pubic hair growth in girls
- Outline the normal sequence of pubertal events from thelarche through menarche with expected timing
- Define precocious puberty (< 8 yr) and delayed puberty (no breast development by 13 yr; no menarche by 15 yr)
- Enumerate the common causes of precocious and delayed puberty and outline their initial management
INSTRUCTIONS
Puberty is the biological transition from childhood to reproductive maturity, orchestrated by a precisely timed neuroendocrine cascade. As a gynaecologist you will encounter girls and young women whose puberty deviates from the norm — arriving too early, too late, or in the wrong sequence. Recognising these deviations requires a firm grounding in what is normal: the order of events, the hormonal drivers, and the clinical staging tools clinicians rely upon. This module builds that foundation, then surveys the spectrum of abnormal puberty you must be prepared to identify and manage.
References
- DC Dutta's Textbook of Gynecology, 8th ed., Ch. 26 — Puberty and its Disorders (textbook)
- Shaw's Textbook of Gynaecology, 17th ed., Ch. 7 — Puberty (textbook)
- Williams Gynecology, 4th ed., Ch. 14 — Pediatric and Adolescent Gynecology (textbook)
- Tanner JM, Marshall WA. Variations in the pattern of pubertal changes in girls. Arch Dis Child. 1969;44(235):291-303 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A mother brings her 7-year-old daughter to the outpatient clinic, anxious about breast buds she noticed a month ago. The child appears otherwise well, is growing taller than her classmates, and has a bone age of 10 years on X-ray. There is no vaginal bleeding. Should you reassure or investigate? Your answer depends entirely on your command of normal pubertal physiology and the thresholds that separate the expected from the pathological.
WHY THIS MATTERS
Puberty disorders are among the most common reasons for paediatric and adolescent gynaecology referrals. Precocious puberty, if untreated, leads to premature epiphyseal fusion and short adult stature. Delayed puberty causes psychosocial distress and may signal serious underlying pathology such as Turner syndrome or a pituitary tumour. Understanding normal puberty underpins the management of amenorrhoea, polycystic ovarian syndrome, and fertility — topics that will recur throughout your gynaecological career. The Tanner staging system, the HPO axis feedback loops, and the ordered sequence of pubertal milestones are foundational knowledge for every practitioner.
RECALL
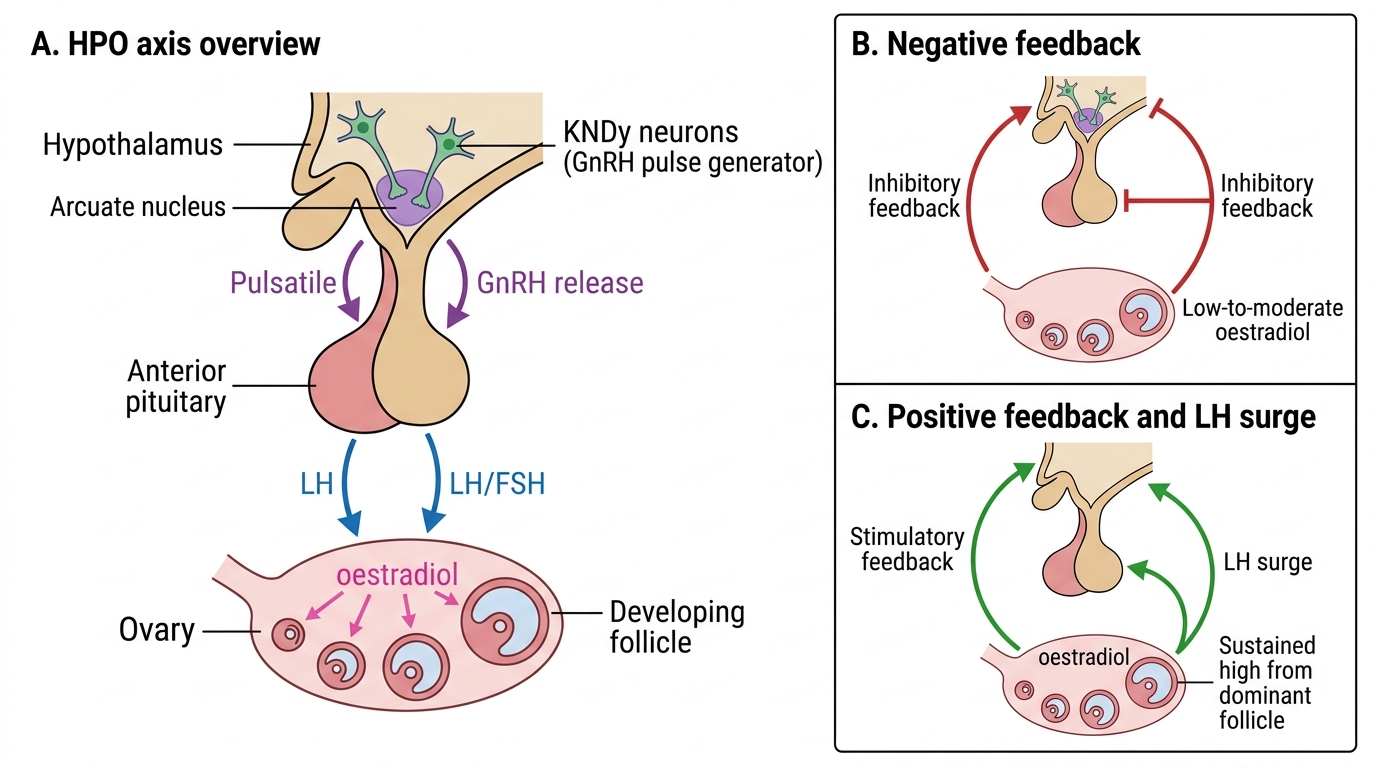
Before proceeding, refresh the following from your physiology studies: (1) The hypothalamic-pituitary axis — GnRH is released in pulses from the arcuate nucleus and stimulates LH and FSH release from the anterior pituitary. (2) Ovarian folliculogenesis — FSH drives follicular development and oestradiol synthesis; the LH surge triggers ovulation. (3) Negative and positive feedback — low oestradiol suppresses GnRH/LH; rising oestradiol at mid-cycle triggers the LH surge (positive feedback). (4) Adrenal cortex — the zona reticularis secretes androgens (DHEAS, androstenedione) independent of the pituitary-ovarian axis.
Why Puberty Matters: Clinical Relevance for the Gynaecologist
Puberty is the physiological process through which a child acquires adult secondary sexual characteristics and reproductive capacity. In girls, it spans approximately 2–5 years, typically between ages 8 and 16, and culminates in the establishment of regular ovulatory menstrual cycles. For the gynaecologist, puberty is not merely a developmental milestone — it is a clinically actionable period. Disorders of puberty alter final adult height, impair bone health, affect fertility, and carry psychosocial consequences that may persist into adult life. Early recognition requires knowing the normal trajectory precisely, because the same physical finding (breast budding) is reassuring at age 9 but demands urgent investigation at age 6.
Clinically, the importance of puberty extends in several directions. Girls presenting with primary amenorrhoea have almost always had an abnormal puberty. The investigation of PCOS, hypothalamic amenorrhoea, and gonadal dysgenesis all trace back to pubertal physiology. Bone mineral density peaks in late adolescence and depends on adequate oestrogen exposure during puberty — a deficit (from delayed puberty or hypothalamic suppression in athletes) translates into lifetime fracture risk. For the examining physician, the Tanner staging examination is the single most standardised and reproducible clinical tool for assessing pubertal progress.
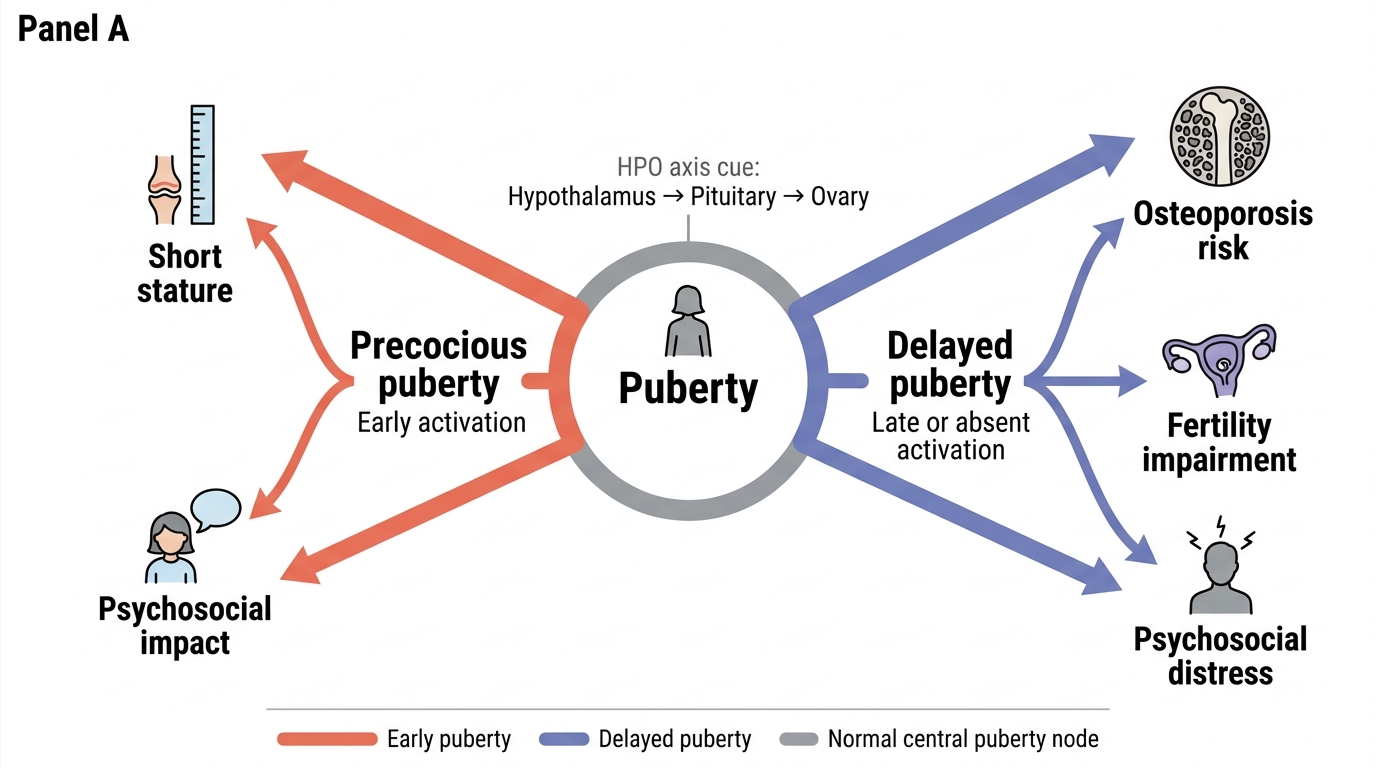
Clinical Consequences of Abnormal Puberty
The HPO Axis and the Hormonal Cascade of Puberty
The initiation of puberty is governed by the hypothalamic-pituitary-ovarian (HPO) axis, which undergoes a profound transformation from a quiescent childhood state to the pulsatile activity that characterises reproductive adulthood. During childhood, the HPO axis is actively suppressed by a combination of central inhibitory mechanisms — primarily the KNDy neurons (kisspeptin, neurokinin B, dynorphin) in the arcuate nucleus of the hypothalamus. These neurons act as a pulse generator for GnRH (gonadotrophin-releasing hormone) release; in childhood their activity is suppressed, keeping GnRH, LH, and FSH levels very low.
At puberty, this suppression lifts. The precise trigger is not fully understood but involves a critical body composition threshold, genetic factors, and metabolic signals (notably leptin). Once KNDy neuron inhibition is released, GnRH is secreted in pulses of increasing amplitude and frequency — particularly at night initially. The anterior pituitary responds with increased secretion of LH (luteinising hormone) and FSH (follicle-stimulating hormone). FSH stimulates ovarian follicular development and oestradiol production; oestradiol drives the development of female secondary sex characteristics — breast tissue, uterine growth, and redistribution of body fat. LH eventually triggers ovulation once positive feedback capacity is established.
The sequence at HPO axis level is: GnRH pulsatility rises → FSH rises first → early follicular development and low oestradiol → then LH rises → granulosa and theca cells produce oestradiol and progesterone → secondary sex characteristics develop → positive feedback matures over 1–3 years → ovulatory cycles establish.
IMPORTANT: Adrenarche (adrenal androgen secretion — DHEAS and androstenedione from the zona reticularis) is a separate event from gonadarche (HPO axis activation). Adrenarche typically precedes gonadarche by approximately 2 years. It drives pubic hair and axillary hair development but is independent of the pituitary-gonadal axis — it is not suppressed by GnRH analogues.
Hypothalamic-Pituitary-Ovarian Axis
SELF-CHECK
Which of the following neurons in the arcuate nucleus act as the primary GnRH pulse generator and whose activity is suppressed during childhood?
A. Dopaminergic neurons
B. KNDy neurons (kisspeptin, neurokinin B, dynorphin)
C. Serotonergic neurons
D. GABA-ergic neurons
Reveal Answer
Answer: B. KNDy neurons (kisspeptin, neurokinin B, dynorphin)
KNDy neurons (expressing kisspeptin, neurokinin B, and dynorphin) in the arcuate nucleus are the hypothalamic GnRH pulse generator. Their inhibition during childhood keeps GnRH, LH, and FSH at prepubertal levels. At puberty this inhibition is released, initiating the hormonal cascade.
Tanner Staging: Breast, Pubic Hair, and Growth
The Tanner staging system (Marshall and Tanner, 1969) provides a standardised, clinically reproducible method for assessing pubertal development by physical examination. It divides breast (B) and pubic hair (PH) development each into five stages, allowing the physician to quantify pubertal progress independently of chronological age. This distinction is important: two girls aged 11 years may be at entirely different pubertal stages, and management decisions depend on staging, not age alone. Without a structured staging system, clinicians would be forced to rely solely on chronological age — a deeply unreliable index of pubertal maturity, given the wide normal range of 8–13 years for thelarche onset. Tanner staging also serves as the universal language in which pubertal disorders are described in referral letters, textbooks, and research studies, making fluency in this system essential.
The system was derived from longitudinal studies of British girls conducted in the 1960s and has since been validated across multiple populations. Two parameters are assessed independently: breast development (B) and pubic hair (PH). Axillary hair, genital development in boys, and testicular volume are also part of the original Tanner description, but for clinical gynaecological practice, breast and pubic hair staging in girls is the core assessment. Importantly, the B and PH stages do not always advance in lockstep — a girl may be at B3 and PH2, or PH3 and B2, and both can be entirely normal. The clinician must assess each independently and then interpret the overall picture in light of the child's age, growth velocity, and bone age.
Breast Development (B1–B5):
- B1 (Tanner I): Prepubertal; elevation of papilla only; no palpable glandular tissue.
- B2 (Tanner II): Thelarche — breast bud stage; small mound of breast tissue and areolar enlargement. This is the first clinically detectable sign of puberty in most girls (mean age 10.5–11 yr; range 8–13 yr).
- B3 (Tanner III): Further enlargement of breast and areola; no separation of contours between them.
- B4 (Tanner IV): Areola and papilla project above the breast to form a secondary mound (double-contour sign); menarche typically occurs at this stage.
- B5 (Tanner V): Adult breast — only the papilla projects; single contour re-established.
Pubic Hair (PH1–PH5):
- PH1: Prepubertal; no pubic hair.
- PH2: Sparse, straight or slightly curled lightly pigmented hair along the labia majora.
- PH3: Darker, coarser, more curled hair extending sparsely over the pubic junction.
- PH4: Adult-type hair, but not yet reaching the thighs; fills the pubic triangle.
- PH5: Adult distribution, spreading to the medial thighs (some authorities add PH6 for further spread).
Axillary hair appears approximately at B3 (Tanner III), after pubic hair. Peak height velocity (the growth spurt in girls) typically occurs between B2 and B3, preceding menarche by 6–12 months. This timing is clinically significant: a girl who has not yet had her growth spurt can still gain significant stature, whereas a girl who is already post-menarche has limited growth remaining.
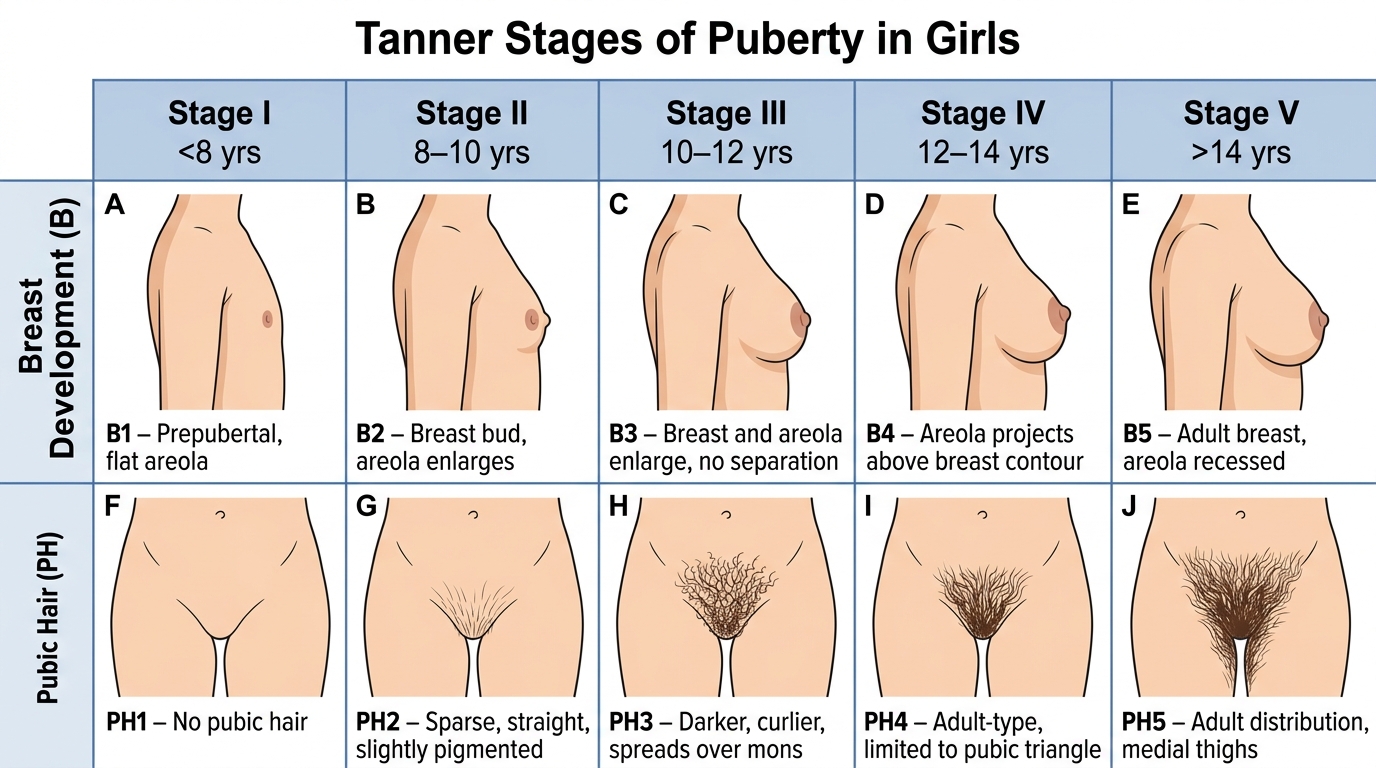
Tanner Stages of Puberty in Girls (Breast and Pubic Hair Development)