Page 2 of 22
OG23.1 | Normal and Abnormal Puberty — SDL Guide (Part 2)
The Sequence of Pubertal Events: Thelarche to Menarche
Normal puberty in girls follows a highly ordered sequence, and deviation from this sequence is itself a diagnostic clue. The clinician must know the expected order, the approximate ages for each event, and the interval between them, because management of abnormal puberty depends on answering: 'Has the sequence been disrupted, or merely delayed?' Understanding the normal choreography of puberty is what allows the clinician to interpret a presenting complaint — isolated pubic hair at age 7 is entirely different from pubic hair accompanied by breast development and accelerated growth, even though the presenting sign is superficially similar. The sequence matters as much as the timing, and recognising out-of-sequence puberty is a distinct clinical skill.
The interval from thelarche to menarche is a particularly useful clinical yardstick. In normal girls this interval is approximately 2–2.5 years. When it is prolonged beyond 5 years, an underlying cause must be sought. When menarche has not followed thelarche within 3 years, investigation is warranted regardless of the girl's chronological age. This framework converts what might otherwise feel like a purely statistical reference range into an actionable clinical decision rule that guides when to reassure and when to investigate.
The typical sequence in girls is:
- Thelarche (B2): Breast budding — the first clinically visible sign of puberty in approximately 85% of girls. Mean age: 10.5–11 yr (range 8–13 yr in normal girls).
- Pubarche (PH2): Appearance of pubic and axillary hair, driven largely by adrenal androgens (adrenarche). Follows thelarche by 3–6 months on average, though in 15–20% of girls pubarche precedes thelarche — a variant of normal.
- Peak Height Velocity (Growth Spurt): Girls reach peak height velocity (mean ~8 cm/yr) at approximately Tanner B3, typically age 11–12 yr. This precedes menarche by 6–12 months. Critically, the growth spurt in girls occurs EARLY in puberty (near B2–B3), unlike boys where it occurs later.
- Menarche: First menstruation, occurring at a mean Tanner stage B4. In India, the mean age of menarche is approximately 12.5–13 yr. Normal range is 10–16 yr. Menarche occurs approximately 2–2.5 years after thelarche.
- Establishment of Regular Cycles: Early post-menarchal cycles are frequently anovulatory. Regular ovulatory cycles generally establish within 2–3 years of menarche as the positive feedback mechanism matures.
A useful clinical rule: the interval from B2 (thelarche) to menarche is approximately 2–2.5 years. If this interval is significantly prolonged (>5 years), an underlying cause should be sought. Similarly, if menarche has not occurred within 3 years of thelarche, investigation is warranted.
IMPORTANT: Premature adrenarche (isolated pubic hair before age 8) and premature thelarche (isolated breast budding before age 8) are variants distinct from true precocious puberty — they do not involve full HPO axis activation. Both are largely benign but require monitoring.
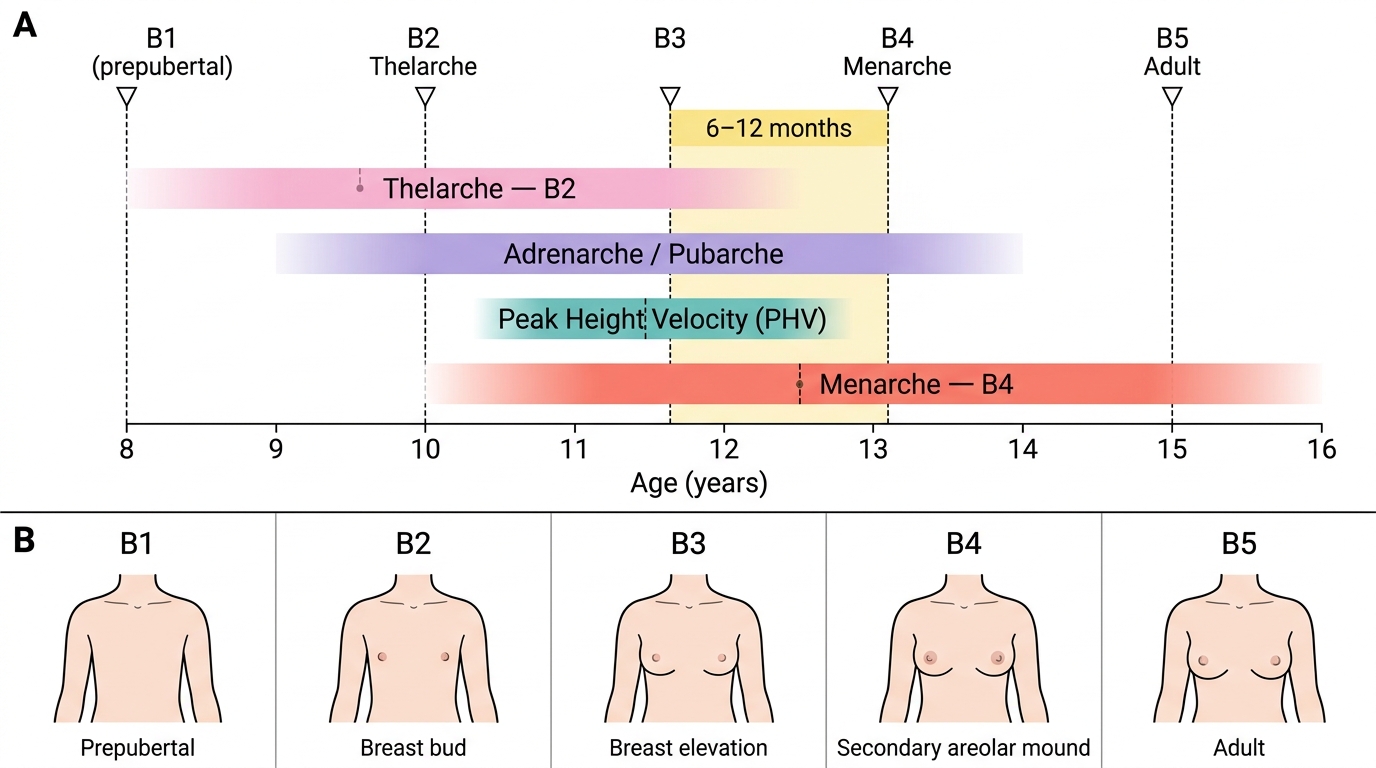
Timeline of Normal Pubertal Events in Girls with Tanner Breast Staging
SELF-CHECK
A 12-year-old girl is at Tanner stage B3. Her mother asks when menarche can be expected. Based on normal pubertal physiology, the most accurate answer is:
A. Menarche has almost certainly already occurred at B3
B. Menarche is expected approximately 6–12 months from now, usually at B4
C. Menarche will not occur until B5 is reached
D. Menarche timing bears no relation to Tanner staging
Reveal Answer
Answer: B. Menarche is expected approximately 6–12 months from now, usually at B4
Menarche in girls typically occurs at Tanner stage B4, approximately 6–12 months after reaching B3. The full interval from thelarche (B2) to menarche (B4) is approximately 2–2.5 years. Understanding this sequence allows the clinician to anticipate and counsel appropriately.
Abnormal Puberty: Precocious and Delayed — A Framework
Abnormal puberty is categorised by timing: precocious (too early) and delayed (too late). Each category is further sub-classified by mechanism, which determines investigation and management. The key conceptual insight is that puberty is not simply an on/off switch — it is a cascade with multiple component steps, each governed by a different part of the endocrine system. This means that abnormal puberty can arise from dysfunction at the hypothalamus, the pituitary, the gonads, the adrenal glands, or from anatomical obstruction, and the clinical and biochemical picture differs entirely depending on which level is affected. Correctly classifying the abnormality directs the investigation pathway efficiently and avoids both unnecessary anxiety from over-investigation and missed pathology from under-investigation.
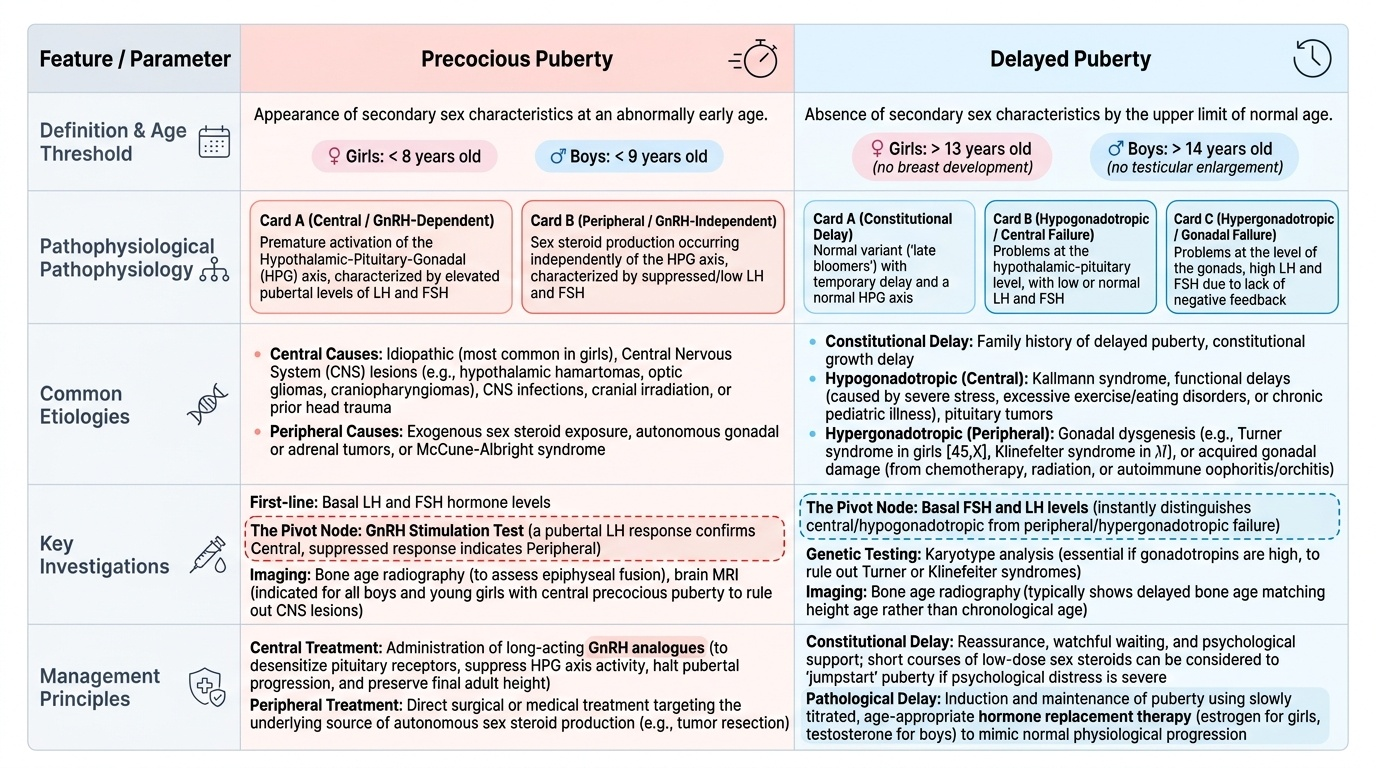
For precocious puberty specifically, the central-versus-peripheral distinction is therapeutically critical: central precocious puberty is treated with GnRH analogues (to suppress HPO axis activity and protect final height), whereas peripheral causes require treatment of the underlying source of autonomous sex steroid production. Measuring LH and FSH — and performing a GnRH stimulation test — is therefore the pivotal investigation that bifurcates the management pathway. Similarly, for delayed puberty, measuring FSH and LH first determines whether the problem lies at the gonadal level (high FSH/LH = hypergonadotropic = gonadal failure) or at the hypothalamic-pituitary level (low FSH/LH = hypogonadotropic = central failure), and this drives the subsequent investigation strategy.
Precocious Puberty is defined as the appearance of secondary sex characteristics before age 8 years in girls (or age 9 in boys). It is further classified as:
- Central (GnRH-dependent) precocious puberty: The HPO axis is prematurely activated. LH and FSH are elevated (pubertal-range); GnRH stimulation test shows pubertal LH response. Most cases in girls are idiopathic (no identifiable cause). Pathological central causes include CNS lesions (hypothalamic hamartoma — most common pathological central cause, optic glioma, craniopharyngioma), CNS infections, irradiation, and prior head injury.
- Peripheral (GnRH-independent) precocious puberty: Sex steroids are produced independent of the HPO axis. LH and FSH are suppressed. Causes include: McCune-Albright syndrome (café-au-lait spots + polyostotic fibrous dysplasia + autonomous ovarian cysts — classic triad), granulosa cell tumour of the ovary (oestrogen-secreting), congenital adrenal hyperplasia (androgen-secreting), and exogenous sex steroids.
Delayed Puberty in girls is defined as:
- No breast development (B2) by age 13 years, OR
- No menarche by age 15 years (primary amenorrhoea with secondary sex characteristics present), OR
- More than 5 years elapsing between thelarche and menarche.
Delayed puberty is classified by gonadotrophin levels:
- Hypogonadotropic hypogonadism (low LH/FSH): HPO axis not activated. Causes: constitutional delay of growth and puberty (CDGP — most common overall; benign, family history positive), Kallmann syndrome (anosmia + hypogonadotropic hypogonadism, GnRH deficiency), hypothalamic suppression (chronic illness, undernutrition, intensive athletics — 'functional'), pituitary adenoma, craniopharyngioma.
- Hypergonadotropic hypogonadism (high LH/FSH): Gonadal failure — the pituitary is signalling but the ovaries cannot respond. Causes: Turner syndrome (45,X — most common cause of primary amenorrhoea; webbed neck, short stature, shield chest, streak ovaries), Swyer syndrome (46,XY gonadal dysgenesis), premature ovarian insufficiency, gonadal irradiation/chemotherapy.
- Eugonadism with outflow tract obstruction: Normal hormones but anatomical block to menstrual outflow. Causes: imperforate hymen (haematocolpos), vaginal atresia, Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome (absent uterus and upper vagina; normal breasts and pubic hair; 46,XX).
Provided image
SELF-CHECK
A 7-year-old girl presents with breast budding (Tanner B2) and pubic hair. Her LH and FSH are in the pubertal range and the GnRH stimulation test shows a pubertal LH response. What is the most likely diagnosis?
A. McCune-Albright syndrome (peripheral precocious puberty)
B. Granulosa cell tumour of the ovary
C. Central (GnRH-dependent) precocious puberty — most likely idiopathic
D. Premature adrenarche only
Reveal Answer
Answer: C. Central (GnRH-dependent) precocious puberty — most likely idiopathic
Elevated LH and FSH with a pubertal GnRH stimulation test response confirms HPO axis activation — this is central (GnRH-dependent) precocious puberty. In girls, the majority (up to 90%) of central precocious puberty is idiopathic, though CNS causes (hypothalamic hamartoma, glioma) must be excluded with brain MRI.
Common Problems of Puberty and Their Management
Certain pubertal variants and disorders are encountered regularly in gynaecological outpatient practice. A structured approach — distinguishing benign variants from pathological conditions — prevents both unnecessary investigation and missed diagnoses.
Premature Thelarche: Isolated breast development before age 8, without other signs of puberty (no pubic hair, no accelerated bone age, no growth spurt). Usually occurs between ages 1–3 yr. Gonadotrophins and oestradiol are at prepubertal levels; bone age is normal. Management: reassurance and observation every 6 months. No treatment required. It is important to confirm isolated thelarche (does not qualify as true precocious puberty) versus early central puberty — if there is accelerated bone age or LH/FSH elevation, central precocious puberty must be excluded.
Premature Adrenarche: Appearance of pubic and/or axillary hair before age 8 without other signs of puberty, driven by early adrenal androgen secretion. DHEAS is elevated for age; gonadotrophins are prepubertal. Management: reassurance; monitor for PCOS and metabolic syndrome in adolescence (premature adrenarche is a risk factor). Exclude congenital adrenal hyperplasia (CAH) — 17-hydroxyprogesterone (17-OHP) to rule out 21-hydroxylase deficiency.
Constitutional Delay of Growth and Puberty (CDGP): The most common cause of delayed puberty in boys; also occurs in girls. Positive family history (father had delayed puberty); growth follows a normal bone-age trajectory (bone age delayed 2–3 yr below chronological age). Gonadotrophins are low-normal. Management: reassurance and watchful waiting. If social/psychological impact is significant, very low-dose oestrogen 'priming' over 6 months may be considered. Must be distinguished from pathological hypogonadotropic hypogonadism (Kallmann syndrome presents with anosmia).
Primary Amenorrhoea — Initial Approach:
- History: family history of delayed puberty; sense of smell (Kallmann's); cyclical abdominal pain (imperforate hymen/outflow obstruction); systemic illness, eating disorder, exercise intensity.
- Examination: secondary sex characteristics present? Tanner staging. External genitalia normal? Hymen intact? Abdominal/pelvic mass?
- Investigations: bone age X-ray (wrist); karyotype (Turner, MRKH, androgen insensitivity); FSH/LH (hypo- vs hypergonadotropic); prolactin; thyroid function; pelvic ultrasound (uterus present?); MRI if Mullerian anomaly suspected or CNS cause.
- Red flags requiring prompt referral: Turner stigmata (short stature, webbed neck, wide-carrying angle), cyclical pelvic pain suggesting haematocolpos, streak gonads with a Y chromosome (gonadectomy required — gonadoblastoma risk).
| Condition | Key Feature | Investigation | Management |
|---|---|---|---|
| Premature thelarche | Isolated breast budding <8 yr; no bone age advance | Baseline FSH/LH; bone age | Reassure; observe 6-monthly |
| Premature adrenarche | Isolated pubic hair <8 yr; adrenal androgens up | DHEAS; 17-OHP (rule out CAH) | Reassure; monitor for PCOS |
| Constitutional delay | Delayed bone age; +ve family Hx; low-normal FSH/LH | Bone age; FSH/LH; karyotype | Watchful waiting; low-dose oestrogen if distressed |
| Turner syndrome | No puberty; short stature; 45,X karyotype | Karyotype; FSH (very high) | Oestrogen replacement + GH; fertility counselling |
| Imperforate hymen | Cyclical pain; haematocolpos on US; bulging hymen | Pelvic ultrasound | Surgical hymenectomy |
CLINICAL PEARL
The growth spurt in girls occurs EARLY in puberty — at Tanner B2–B3 — and the child reaches near-adult height approximately 6–12 months before menarche. This means that if you see a girl with precocious puberty (age 7, Tanner B3), her bones are likely already advancing rapidly and she may lose 5–10 cm of final adult height if untreated. In contrast, boys' growth spurt occurs late (Tanner G3–G4), so delayed treatment in boys is less detrimental to final height. This temporal difference is the reason that precocious puberty in girls is treated more urgently from a height perspective.