Page 1 of 18
OG26.1-2 | Genital Injuries and Fistulae — SDL Guide
Learning Objectives
- Describe the causes and clinical features of acute genital injuries including vulvovaginal lacerations, perineal tears, and cervical injuries
- Explain the pathophysiology of obstetric fistula formation through prolonged obstructed labour
- Classify urogenital and rectovaginal fistulae by anatomy and aetiology
- Outline the diagnostic approach to vesicovaginal and ureterovaginal fistulae using dye tests, cystoscopy, and imaging
- Describe the principles of surgical management and timing of fistula repair
- Recognise prevention strategies including skilled birth attendance and access to emergency obstetric care
INSTRUCTIONS
Genital injuries and fistulae represent a spectrum from acute obstetric trauma to devastating long-term morbidity. Obstetric fistulae — predominantly vesicovaginal — are a marker of healthcare system failure and affect millions of women in low-resource settings, including India. Understanding their formation, investigation, and repair principles is essential for every clinician involved in women's health. This SDL uses the OG disease arc: clinical presentation → pathophysiology → diagnosis → management → self-assessment.
References
- DC Dutta's Textbook of Obstetrics, 9th ed., Ch 32 (Injuries to the Birth Canal), Ch 33 (Vesicovaginal Fistula) (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., Ch 34 (Fistulae) (textbook)
- WHO, UNFPA: Obstetric Fistula — Guiding Principles for Clinical Management and Programme Development, 2006 (guideline)
- TeLinde's Operative Gynaecology, 11th ed., Ch 31 (Urinary Tract Fistulas) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 20-year-old primigravida from a rural village in Bihar presents to a district hospital complaining of constant leakage of urine from the vagina for the past three weeks. She delivered at home three weeks ago after a labour lasting nearly two days. The delivery was difficult and protracted, and she eventually delivered a macerated stillborn baby. She is malnourished and visibly distressed — she describes how she can no longer sit with her family at meals because of the smell, and her husband has moved out. On examination, the vaginal walls are pale and indurated, with a visible opening in the anterior vaginal wall communicating with the bladder. This woman has an obstetric vesicovaginal fistula — a preventable complication of obstructed labour that has destroyed her continence, her dignity, and her social standing. Understanding how this happened, how to diagnose it correctly, and how to repair it begins with this module.
WHY THIS MATTERS
Genital injuries are encountered in every obstetric unit — from first-degree perineal tears in uncomplicated deliveries to complex lacerations and haematomas following instrumental or obstructed labour. Recognition and timely repair prevent long-term sequelae. Fistulae, particularly vesicovaginal fistulae (VVF), represent one of the most disabling complications in obstetrics and gynaecology. The World Health Organization estimates that approximately 2 million women live with obstetric fistula globally, with 50,000–100,000 new cases occurring annually. India bears a significant share of this burden, concentrated in low-resource states. For the MBBS graduate, the ability to identify risk factors, diagnose a fistula correctly (and distinguish VVF from ureterovaginal fistula), counsel patients on treatment options, and refer appropriately is a core clinical competency. These conditions also appear regularly in written examinations and clinical postings.
RECALL
Before proceeding, activate your prior knowledge. Recall the anatomical relationships in the female pelvis: the urinary bladder lies anterior to the uterus and vagina, and the ureters course through the base of the broad ligament passing close to the uterine cervix before entering the bladder trigone — this proximity makes ureteric injury a recognised complication of hysterectomy. Recall the layers of the perineum from anatomy: perineal skin, superficial and deep perineal pouches, the perineal body (the fibromuscular node at the centre of the perineum to which multiple muscles attach). Recall the grades of perineal tear you may have encountered in your obstetric posting. From Physiology, recall the mechanism of urinary continence — the urethrovesical junction and the role of the internal and external urethral sphincters. These anatomical and physiological foundations will make the mechanism of injury and the principles of fistula repair immediately comprehensible.
Clinical Presentation of Genital Injuries and Fistulae
The clinical presentation of genital tract injuries and fistulae varies considerably depending on whether the condition is acute or chronic. Acute genital injuries present at the time of delivery or surgery: pain, bleeding, swelling, and haematoma formation are the cardinal features. Vulvovaginal lacerations following delivery present with active bleeding from identifiable tears, which may be superficial (mucosa only) or extend into deeper tissue planes. Perineal tears present with bleeding and pain; the degree of tear determines the extent of disruption — from superficial skin tears to complete division of the external anal sphincter and rectal mucosa. Broad ligament haematomas may present with pelvic pain, signs of concealed haemorrhage, and a lateral pelvic mass. Cervical lacerations at the time of forceps delivery or rapid second stage can cause brisk haemorrhage even when the uterus is well contracted.
Fistulae, in contrast, typically present in the days to weeks following the precipitating event. The classic presentation of a vesicovaginal fistula (VVF) is the triad of: (1) continuous involuntary leakage of urine per vaginum (patient cannot store any urine — even when she feels the urge, leakage is constant), (2) absence of the normal desire to void (because the bladder never fills), and (3) dry vaginal pad (some patients describe soiling of clothing continuously). The leakage is constant and unrelated to position or exertion, which distinguishes it from stress incontinence. Rectovaginal fistula (RVF) presents with passage of flatus and faeces through the vagina, faecal soiling, and recurrent vaginal or urinary tract infections from faecal contamination. A ureterovaginal fistula (UVF) presents with continuous vaginal discharge that may be mistaken for VVF but with a key difference: the patient retains some bladder filling and the urge to void remains intact (because one kidney and ureter continue to drain normally into the bladder). Secondary features common to all fistulae include perineal excoriation from constant moisture, social isolation, depression, and in obstetric fistula patients — often a history of stillbirth.
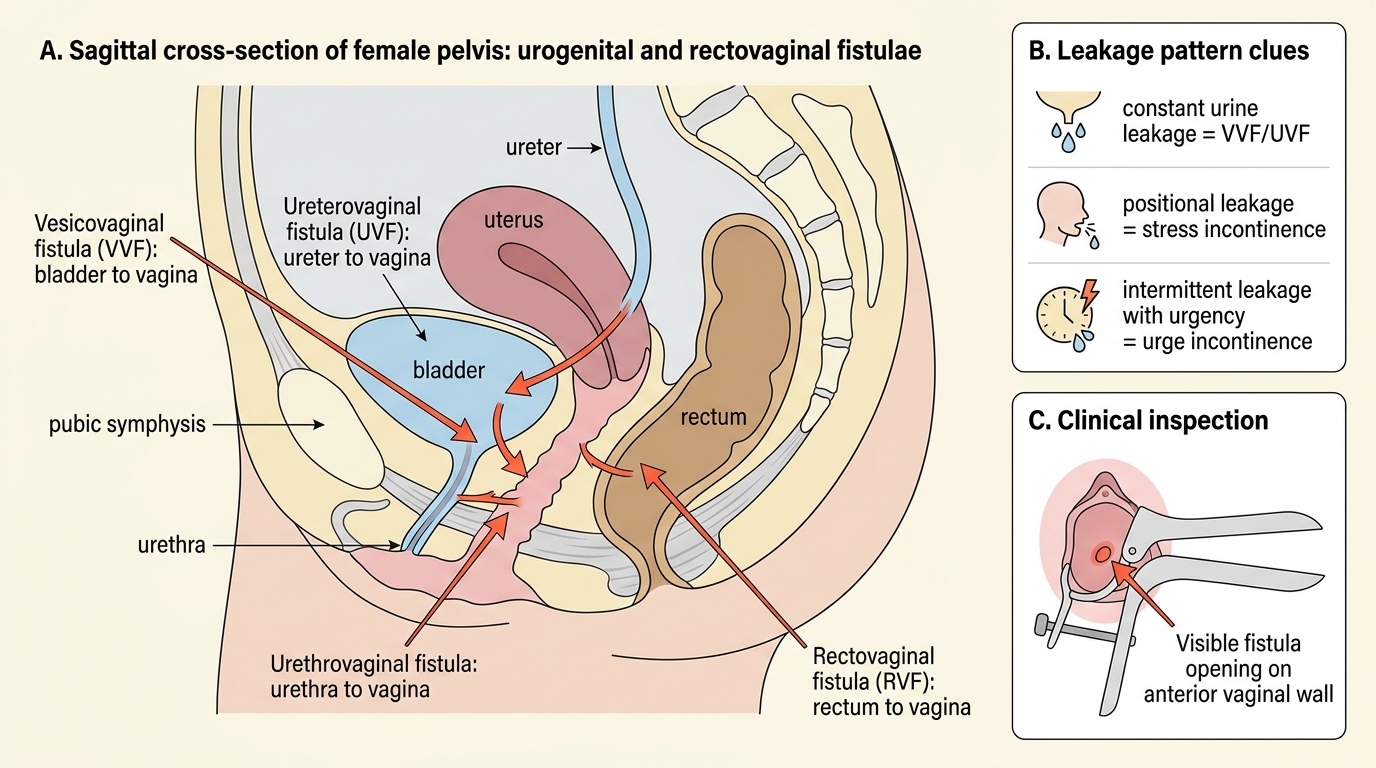
Female Genital Fistulae: Sagittal Pelvic Anatomy
Key points for the clinical encounter: always ask about the obstetric history (duration of labour, mode of delivery, outcome of baby), the temporal relationship between delivery/surgery and onset of symptoms, and the pattern of leakage (constant = VVF/UVF; positional = stress incontinence; intermittent = urge incontinence). Examination should include inspection of the vagina with a speculum — the fistula opening may be directly visible, particularly on the anterior vaginal wall in VVF.
Pathophysiology and Aetiology
Understanding the mechanism of genital injury and fistula formation requires an appreciation of how prolonged mechanical pressure or surgical trauma destroys the tissue planes separating adjacent organ systems. In obstetric fistula — the commonest type in developing countries — the mechanism is ischaemic pressure necrosis. During prolonged obstructed labour, the presenting fetal part (typically the head) becomes impacted in the pelvis. The soft tissues of the bladder base, vesicovaginal septum, and anterior vaginal wall are compressed between the bony pelvis and the fetal skull. This sustained ischaemia — lasting many hours — leads to necrosis of the compressed tissue. When the baby is finally delivered (often by operative means or after fetal death), the necrotic tissue sloughs over the following days, leaving a communication between the bladder and the vagina. The same mechanism can produce ureterovaginal, urethrovaginal, or rectovaginal communications depending on which tissue planes are compressed. The critical determinant is the duration of impaction: obstructed labour lasting more than 24 hours carries the highest risk. Associated factors include a contracted or android pelvis (common in adolescent girls who conceive before pelvic maturation is complete), primiparity, small maternal stature, large fetal head, and malposition.
Surgical (iatrogenic) fistulae arise from inadvertent injury to the bladder, ureter, or rectum during gynaecological surgery — most commonly total abdominal or vaginal hysterectomy, anterior colporrhaphy, or radical pelvic surgery. The ureter is most vulnerable as it passes beneath the uterine artery ('water under the bridge') and then through the ureteric tunnel in the cardinal ligament — both points of risk during ligation of the uterine pedicles. Bladder injury at hysterectomy can arise from adhesions (previous caesarean section), dense endometriosis, or technically difficult dissection. Radiotherapy fistulae result from radiation injury to the small vessels supplying the pelvic viscera — the tissue becomes ischaemic, fibrotic, and eventually breaks down, typically 6 months to 2 years after treatment for cervical or endometrial cancer. Malignancy can erode through tissue planes directly. Rare causes include Crohn's disease (RVF), lymphogranuloma venereum, and foreign bodies.
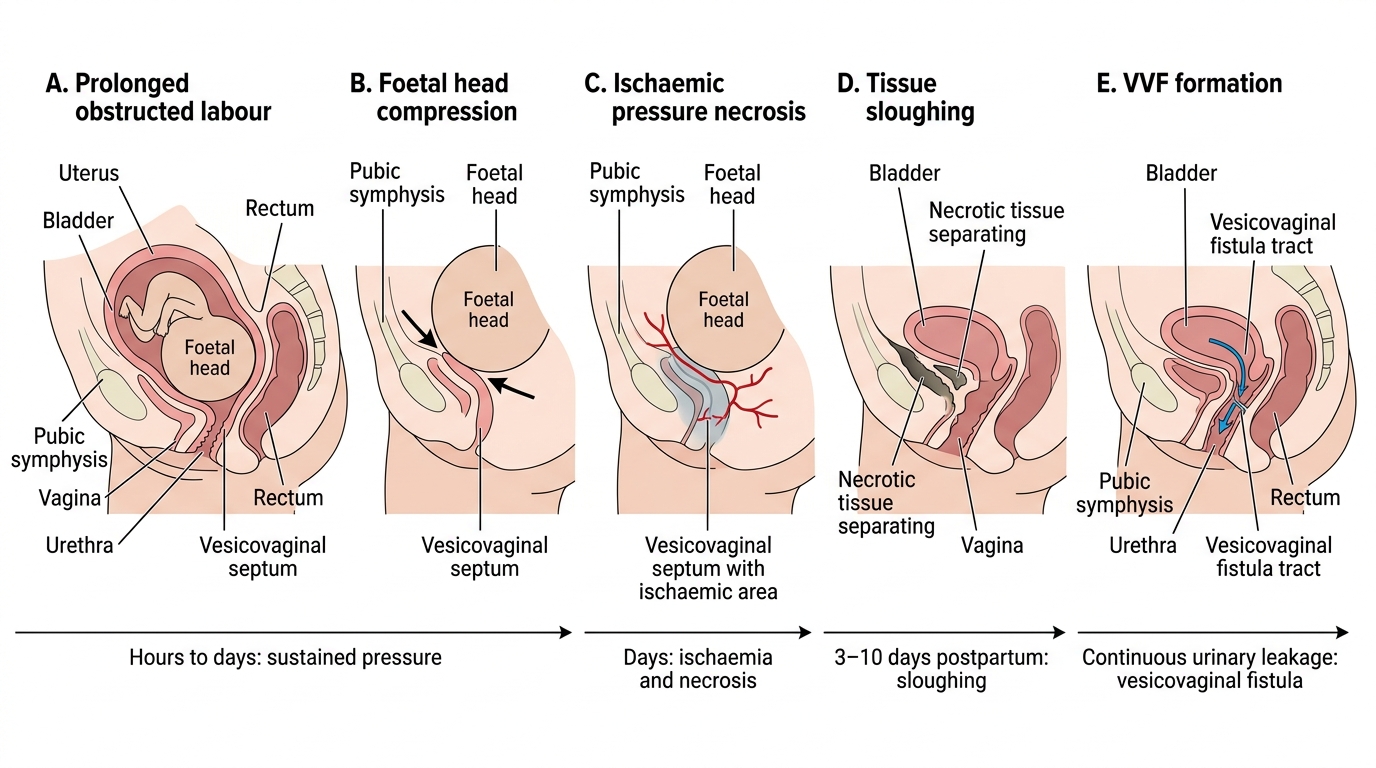
Mechanism of Vesicovaginal Fistula After Obstructed Labour
For acute genital injuries, the mechanisms include:
- Obstetric trauma: uncontrolled delivery, instrumental delivery, shoulder dystocia manoeuvres, inappropriate fundal pressure
- Coital injury: particularly in adolescents, post-menopausal atrophic vagina, or following sexual assault
- Accidental injury: straddle injuries (e.g., falling astride a fence)
- Surgical injury: colpotomy, dilation and curettage, manual removal of placenta
Types of Genital Injuries
Acute genital injuries encompass a broad spectrum of tissue disruptions that occur at the time of delivery, during gynaecological procedures, or from accidental trauma. They are classified by anatomical site — vulva, vagina, perineum, cervix, uterus — and by the depth of tissue involvement. A systematic approach to classification is essential in clinical practice: it guides the extent of repair required, determines whether specialist referral is necessary, and prevents missed injuries that can lead to serious long-term sequelae such as faecal incontinence, haematoma expansion, or secondary haemorrhage. Every woman who delivers vaginally must be examined after delivery for genital tract lacerations, regardless of whether the delivery appeared straightforward. The examination should be performed under good lighting with adequate analgesia, and should proceed from the vulva inward — inspecting the labia minora, clitoris, perineum, vaginal walls, and cervix in turn. Rectal examination is mandatory to exclude anal sphincter involvement whenever a perineal tear is found.
Vulvovaginal and perineal lacerations are graded according to depth and tissue involvement. The classification of perineal tears is standardised and clinically important:
| Degree | Structures Involved | Key Features |
|---|---|---|
| First degree | Perineal skin and vaginal mucosa only | No muscle involvement; most heal without suturing |
| Second degree | Perineal skin, vaginal mucosa, AND perineal muscles (bulbospongiosus, superficial transverse perinei) — external anal sphincter (EAS) INTACT | Requires layer-by-layer repair |
| Third degree | Perineal body + partial/complete tear of external anal sphincter (EAS) | Subdivided: 3a (<50% EAS), 3b (>50% EAS), 3c (internal anal sphincter IAS also torn) |
| Fourth degree | Perineal body + EAS + IAS + anorectal mucosa (through full rectal wall) | Requires specialist repair; risk of faecal incontinence |
Third and fourth degree tears are collectively termed obstetric anal sphincter injuries (OASIS) and carry significant risk of faecal incontinence if not recognised and repaired correctly. Risk factors for OASIS include forceps delivery (highest risk), large baby, persistent occiput posterior position, mediolateral episiotomy (protective), and primiparity.
Cervical lacerations are common after rapid second stage, precipitate delivery, or forceps application. Most are superficial and heal spontaneously. Deep lateral cervical lacerations may extend into the vaginal fornix or paracervical tissue and cause significant haemorrhage; they should be repaired under adequate visualisation and anaesthesia. Rarely, a cervical tear extends into the lower uterine segment — this is a partial uterine rupture.
Paravaginal and broad ligament haematomas form when bleeding from torn vessels tracks into the loose areolar tissue alongside the vagina or into the broad ligament. Superficial haematomas may be managed conservatively with analgesia and ice packs if small and stable. Expanding haematomas require drainage and ligation of the bleeding point.
Uterine rupture represents the most life-threatening acute genital injury — most commonly in the lower uterine segment, associated with previous uterine scar (e.g., caesarean section). It is covered in more detail in the obstructed labour module.