Page 2 of 18
OG26.1-2 | Genital Injuries and Fistulae — SDL Guide (Part 2)
Types and Classification of Fistulae
Genital fistulae are abnormal communications between the genital tract and an adjacent hollow viscus — most commonly the urinary bladder, ureter, urethra, or rectum. They represent a diverse group of conditions that share the common consequence of involuntary loss of urine or faeces through the vagina, with profound effects on the patient's physical health, psychological wellbeing, and social functioning. A systematic classification by anatomical site and by aetiology is essential because it directly determines the investigation pathway and the surgical approach. The anatomy defines which viscus is involved and which surgical technique restores continuity; the aetiology determines whether the repair is straightforward (fresh obstetric) or exceptionally challenging (radiation-induced, recurrent, or malignancy-associated). Every clinician involved in women's health must be able to distinguish at least the two commonest types — vesicovaginal and ureterovaginal fistulae — because confusing one for the other leads to the wrong operation and potentially irreversible harm.
Anatomical classification:
- Urogenital fistulae — communicating with the urinary tract:
- Vesicovaginal fistula (VVF): between the bladder (most commonly the posterior/trigonal wall) and the anterior vaginal wall — the COMMONEST type in obstetric practice
- Ureterovaginal fistula (UVF): between a ureter and the vagina — most often surgical (post-hysterectomy ureteric injury)
- Urethrovaginal fistula: between the urethra and the anterior vaginal wall — can result from anterior colporrhaphy or prolonged catheterisation
- Vesicouterine fistula: between the bladder and the uterine cavity — rare; associated with uterine rupture or caesarean section
- Rectogenital (colorectal) fistulae:
- Rectovaginal fistula (RVF): between the rectum and the posterior vaginal wall — obstetric (fourth degree tear breakdown), surgical, Crohn's, radiation, malignancy
- Colovaginal fistula: less common; associated with diverticular disease or cancer
Aetiological classification:
- Obstetric: prolonged obstructed labour (pressure necrosis) — by far the commonest cause globally and in India
- Surgical (iatrogenic): hysterectomy, anterior colporrhaphy, pelvic dissection — commonest cause in developed countries
- Radiation: post-radiotherapy for cervical/endometrial cancer — delayed, poor vascularity, high recurrence after repair
- Malignant: direct tumour erosion — must be excluded before any repair is attempted
- Inflammatory: Crohn's disease (RVF), lymphogranuloma venereum
- Congenital: rare (ectopic ureter, cloacal abnormality)
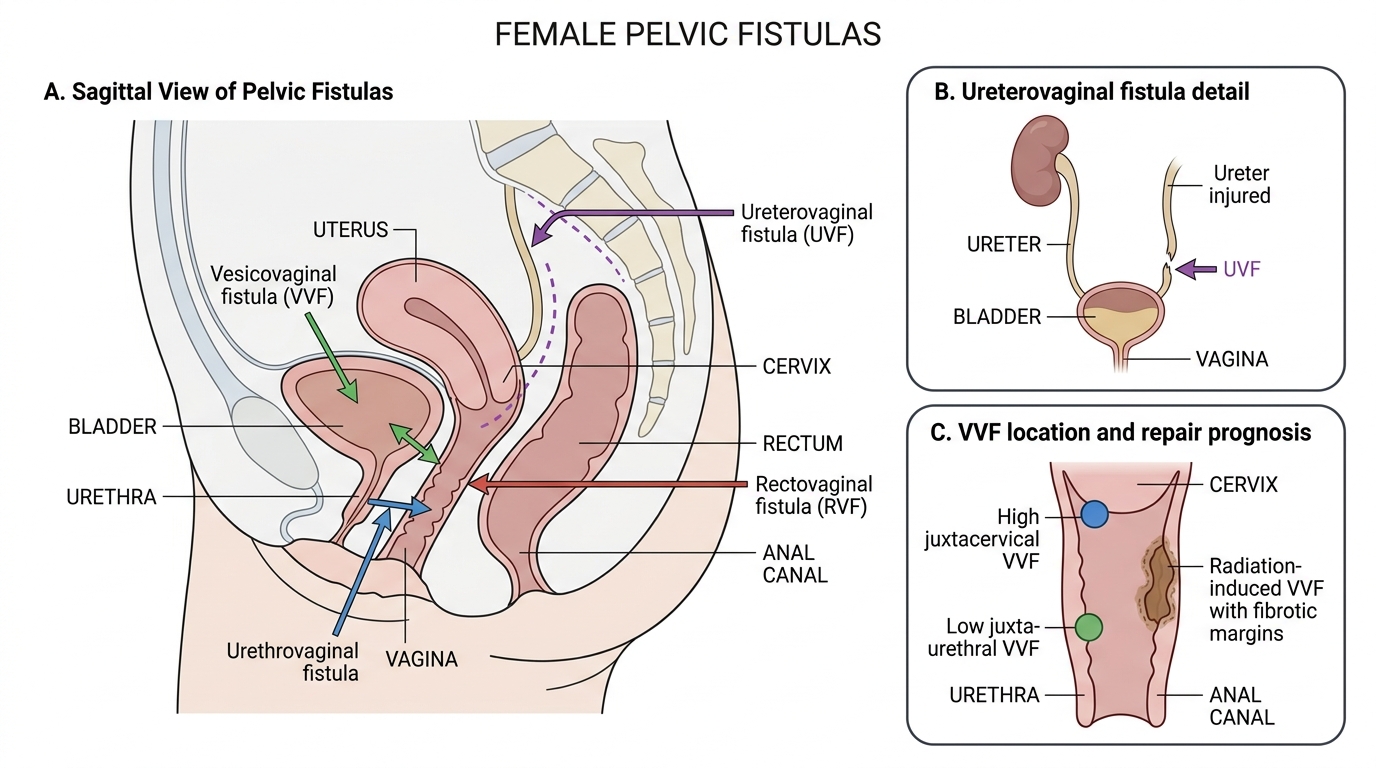
Female Pelvic Fistula Types
The size and location of a VVF also carry prognostic and management implications. Juxtacervical (near the cervix, high) fistulae are most often obstetric and may be large. Juxta-urethral (near the urethra, low) fistulae carry risk of post-repair stress incontinence because of proximity to the continence mechanism. Radiation-induced fistulae have poorly vascularised, fibrotic margins and carry the worst prognosis for repair.
SELF-CHECK
A 25-year-old woman complains of continuous urinary leakage following a vaginal hysterectomy 10 days ago. She reports she still feels the urge to void and can pass urine normally, but notes a constant wet vaginal discharge as well. Which fistula type is most likely?
A. Vesicovaginal fistula (VVF)
B. Ureterovaginal fistula (UVF)
C. Urethrovaginal fistula
D. Rectovaginal fistula (RVF)
Reveal Answer
Answer: B. Ureterovaginal fistula (UVF)
The key distinguishing feature is that she retains the urge to void and can pass urine voluntarily — this means her bladder still fills and empties, ruling out VVF (in which the bladder never fills, there is no urge, and leakage is completely constant). A ureterovaginal fistula (UVF) from ureteric injury at hysterectomy produces continuous vaginal leakage while the opposite kidney continues to drain normally into the bladder, so bladder function and urge are preserved. The surgical context (post-hysterectomy) is also typical for UVF.
Diagnosis and Investigation
The diagnosis of a genital fistula begins at the bedside with a carefully elicited history and targeted examination, and is confirmed by a structured sequence of investigations. The history typically establishes the precipitating event (obstructed labour, recent surgery, radiotherapy, or known malignancy), the timing of symptom onset relative to that event, and the character of the leakage — continuous versus intermittent, urine versus faecal material, and whether normal voiding is preserved. Examination under good lighting with a Sims speculum will often reveal the fistula opening directly on the anterior or posterior vaginal wall. However, small fistulae may not be visible on routine inspection, and even when a fistula is seen, further investigation is mandatory before surgery to (a) confirm the anatomical site and size, (b) determine the number of fistulae (multiple are not uncommon in obstetric cases), (c) precisely distinguish VVF from UVF — since this determines the operation — (d) assess the condition of surrounding tissue, and (e) exclude an underlying malignancy, which must never be missed.
Dye tests form the cornerstone of bedside diagnosis:
- Methylene blue dye test (for VVF): 200–300 mL of methylene blue dye is instilled into the bladder via a catheter, and three swabs are placed in the vagina. If the upper swab becomes blue-stained, the dye has passed through a bladder-to-vagina fistula (VVF confirmed). If the uppermost swab remains dry but the other swabs are wet, the leak is from the urethra. If the swabs remain unstained but are wet, the leak is not from the bladder — a three-swab test variant then uses oral phenazopyridine (which colours urine orange) to check for ureteric leak.
- Indigo carmine test (for UVF): indigo carmine 5 mL is given intravenously; 10–20 minutes later, the vaginal swabs are inspected. Orange-stained swab indicates ureteric leakage (UVF confirmed). This test is used when the methylene blue test is negative but vaginal leakage continues.
Cystoscopy is essential before any surgical repair. It identifies the position of the fistula relative to the ureteric orifices, the size and number of fistulae, any surrounding inflammation, necrotic tissue, or stone formation, and the condition of the bladder mucosa. Small fistulae (<0.5 cm) not visible on speculum may only be found on cystoscopy.
Intravenous urogram (IVU) / IVP is performed to assess the upper urinary tract, particularly to identify ureteric obstruction, hydronephrosis (suggesting ureteric injury at hysterectomy), or ectopic ureteric opening. It is mandatory when UVF is suspected.
MRI is particularly useful for complex or recurrent fistulae, radiation-induced cases, and to define the fistula tract relative to surrounding structures before complex repair.
Examination under anaesthesia (EUA): for fistulae that are not clearly visible on outpatient examination, EUA with careful vaginal inspection, probing of the tract, and simultaneous cystoscopy provides the most complete preoperative assessment.

Provided image
Important diagnostic principles:
1. Always exclude malignancy — biopsy the fistula edge if there is any suspicion of tumour, or if the fistula appeared spontaneously without prior surgery or obstructed labour
2. Multiple fistulae are not rare in obstetric cases — assess the entire vaginal wall
3. Assess renal function (serum creatinine, urea) before surgery — ureteric involvement may cause chronic obstructive nephropathy
SELF-CHECK
A methylene blue dye test is performed in a woman with continuous vaginal wetness after obstetric delivery. The vaginal swabs remain unstained but are clearly wet. What should be the next diagnostic step?
A. Repeat the methylene blue test with a larger dye volume
B. Perform intravenous indigo carmine test to check for ureterovaginal fistula
C. Proceed directly to cystoscopy
D. Diagnose urethrovaginal fistula and plan repair
Reveal Answer
Answer: B. Perform intravenous indigo carmine test to check for ureterovaginal fistula
Unstained but wet swabs after methylene blue instillation means the urine leak is NOT from the bladder — ruling out VVF. The leak is from the upper urinary tract (ureter). The next step is an intravenous indigo carmine test: IV administration followed by inspection for orange staining of the vaginal swabs confirms ureterovaginal fistula (UVF). Cystoscopy alone would not diagnose UVF, and repeating the methylene blue test would give the same result.
Management — Principles and Surgical Repair
The management of genital injuries and fistulae is guided by the type and anatomical site of the injury, the size and location of the fistula, the timing of presentation relative to the precipitating event, and crucially, the condition of the surrounding tissues at the time of intervention. These factors together determine whether immediate repair is feasible, whether conservative measures should be tried first, and how long to wait before definitive surgery. The overarching goals are: to restore the anatomical integrity of the genital tract; to re-establish urinary or faecal continence; to eradicate infection, which impairs healing; to preserve fertility where relevant; and to optimise the patient's long-term quality of life. Prevention — through skilled birth attendance, access to emergency obstetric care, and safe surgical technique — remains the most powerful and cost-effective intervention, and the clinician must understand both the curative and preventive dimensions of management to counsel patients and advocate for system-level change.
Management of acute genital injuries:
- All perineal tears should be repaired under adequate anaesthesia (regional or local infiltration) with good visualisation and lighting.
- First-degree tears: most do not require suturing; if repaired, a single layer of continuous absorbable suture suffices.
- Second-degree tears: repair in layers — vaginal mucosa first, then perineal muscles (continuous or interrupted absorbable suture), then perineal skin.
- OASIS (3rd and 4th degree): requires expert repair, ideally in an operating theatre. The anal sphincter ends must be identified and approximated — either end-to-end (overlapping technique preferred for EAS). The IAS is repaired separately. Postoperative care includes broad-spectrum antibiotics, laxatives to prevent constipation, and careful follow-up.
- Haematomas: small, stable haematomas (<5 cm) — ice, analgesia, close observation; expanding or large haematomas — incision, evacuation, ligation of bleeding vessel, packing or drainage.
Management of fistulae — conservative:
For very small VVF (less than 0.5 cm) detected within the first week, continuous bladder drainage by indwelling catheter for 4–6 weeks may allow spontaneous closure in up to 20–30% of cases. This approach requires that the fistula be fresh and not associated with significant tissue necrosis. Concurrent urinary tract infection must be treated.
Timing of surgical repair — the fundamental rule:
The single most important principle in fistula management is the timing of surgery. Two approaches apply:
- Early repair (within 48–72 hours): indicated when the fistula is recognised immediately (e.g., bladder injury identified intraoperatively) or as an immediate fresh traumatic injury. Conditions: fresh, non-oedematous, non-infected tissue with clear margins that can hold sutures.
- Delayed repair (traditionally 3 months, often extended to 6 months for obstetric fistulae with significant tissue necrosis): the principle is to allow full resolution of inflammation, oedema, and necrosis so that healthy, vascularised tissue is available for repair. Operating on inflamed, friable, necrotic tissue leads to repair breakdown and recurrence.
Surgical Principles of VVF Repair
Principles of surgical repair (applicable to all fistulae):
1. Adequate exposure and visualisation: the entire fistula must be clearly seen; use adequate lighting, retractors, and anaesthesia
2. Healthy tissue margins: excise all necrotic or fibrotic tissue back to healthy, bleeding, well-vascularised edges
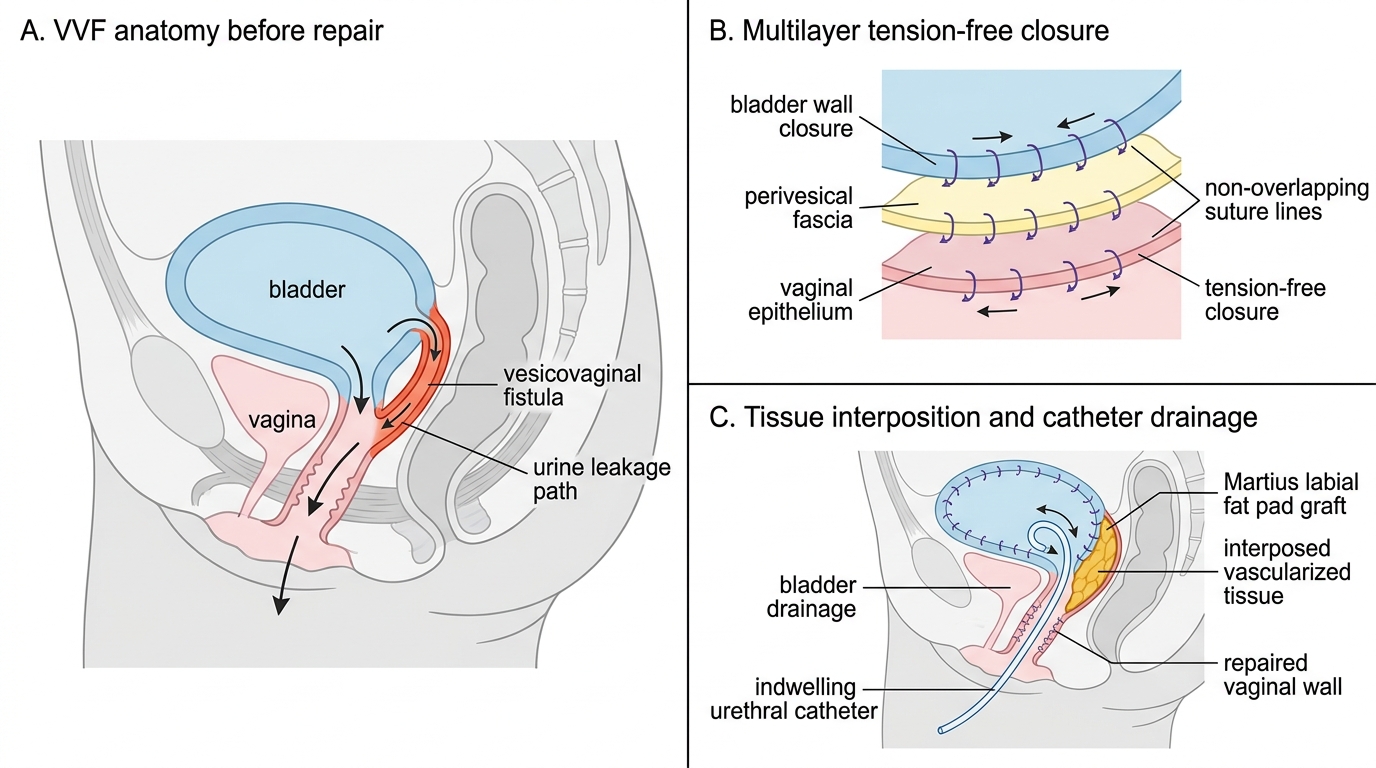
3. Tension-free closure: the suture line must not be under tension — mobilise surrounding tissue adequately before closing
4. Multilayer closure: close in separate layers to interpose healthy tissue between suture lines; avoid suture line overlap
5. Vascularised tissue interposition: for large, complex, or radiation-induced fistulae — interpose a pedicled flap of healthy tissue (e.g., Martius labial fat pad graft for VVF; omentum for abdominal repairs) between the suture lines
6. Adequate post-operative drainage: indwelling urethral catheter for 10–14 days (some surgeons extend to 21 days); suprapubic catheter for large repairs; anti-spasmodic agents to reduce bladder contractions
Specific surgical approaches:
- VVF — vaginal approach (preferred for most VVF): Latzko colpocleisis (extraperitoneal, excises the fistula with surrounding vaginal tissue and closes the defect; simplest for post-hysterectomy, high VVF) or formal layered repair (dissection of vesicovaginal space, separate bladder and vaginal wall closure with tissue interposition). Success rate >90% for primary obstetric VVF at expert centres.
- VVF — abdominal approach: for complex, high, or recurrent fistulae requiring simultaneous ureteric reimplantation; also used when there is associated uterine pathology
- UVF: ureteric reimplantation (ureteroneocystostomy) is required — the damaged ureteric segment is excised and the ureter reimplanted directly into the bladder
- RVF: layered repair via vaginal or perineal approach; protective diverting colostomy may be required for large or radiation-associated RVF
Prevention — the most important intervention:
- Skilled birth attendance and access to emergency obstetric care for all women
- Early recognition and management of obstructed labour (avoiding prolonged unattended labour)
- Adequate surgical training to prevent iatrogenic injuries
- Safe surgical techniques: identification and dissection of ureters before uterine vessel ligation; careful bladder mobilisation at caesarean section
SELF-CHECK
A woman delivered vaginally 6 weeks ago after a prolonged obstructed labour. She now has a 2 cm VVF confirmed on cystoscopy. The vaginal tissues are still oedematous and indurated on examination. What is the most appropriate management?
A. Immediate surgical repair (Latzko procedure) within the next week
B. Continuous bladder catheterisation for 4–6 weeks in the hope of spontaneous closure
C. Delay surgery for a further 6–10 weeks to allow complete tissue resolution, then repair
D. Recommend permanent urinary diversion
Reveal Answer
Answer: C. Delay surgery for a further 6–10 weeks to allow complete tissue resolution, then repair
For obstetric VVF presenting at 6 weeks, the tissues are still in the active inflammatory/resolution phase — oedematous, indurated, poorly vascularised. Operating at this stage leads to repair failure because the sutures cannot hold. The standard principle is to delay repair until tissues are soft and well-vascularised — conventionally 3 months from delivery, sometimes 6 months for large obstetric fistulae with significant necrosis. Catheter drainage is appropriate for small (<0.5 cm) fistulae in the first week, not a 2 cm established fistula. Permanent diversion is a last resort.
CLINICAL PEARL
The two hallmarks that distinguish VVF from UVF at the bedside: (1) In VVF, the woman CANNOT store urine — the bladder never fills, she has no desire to void, and leakage is completely continuous. In UVF (from one ureter), the opposite kidney continues to drain, the bladder fills, the patient retains the urge to void and can pass urine normally — the constant vaginal wetness is on TOP of normal voiding. (2) The methylene blue dye test confirms VVF (blue-stained swab) but will be NEGATIVE in UVF — the next step is intravenous indigo carmine or IVU. Confusing these two conditions leads to the wrong surgery: UVF requires ureteric reimplantation, not VVF repair. This distinction is a favourite examination question.