Page 8 of 18
OG27.2 | Genital Tuberculosis — SDL Guide
Learning Objectives
- Describe the aetiology and pathogenesis of female genital tuberculosis including the route of spread and sites of involvement
- Identify the clinical presentations of genital TB, particularly its role as a cause of primary infertility in India
- List the investigations used in the diagnosis of genital TB including endometrial biopsy, CBNAAT, laparoscopy, and HSG
- Describe the histopathological features that confirm genital TB
- Outline the standard anti-tubercular therapy (ATT) regimen and its duration for genital TB
- Discuss the long-term implications including irreversible tubal damage, endometrial fibrosis, and fertility prognosis post-treatment
INSTRUCTIONS
Female genital tuberculosis is a clinically silent but destructive disease that silently destroys the fallopian tubes and endometrium, leading to infertility. In India, it is one of the commonest causes of tubal-factor infertility. It is insidious — most women present with infertility and have no obvious constitutional symptoms, making a high index of clinical suspicion essential. This module follows the OG disease arc: clinical presentation → pathology → diagnosis → management → self-assessment.
References
- DC Dutta's Textbook of Gynaecology, 7th ed., Ch 21 (Tuberculosis of the Female Genital Tract) (textbook)
- Shaw's Textbook of Gynaecology, 16th ed., Ch 23 (Genital Tuberculosis) (textbook)
- RNTCP/NTEP India: National Strategic Plan for TB Elimination 2017-2025; WHO Treatment of Drug-Susceptible Tuberculosis, 2022 (guideline)
- Jeffcoate's Principles of Gynaecology, 8th ed., Ch 26 (Pelvic Infections) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old married woman from a small town in Rajasthan presents to the infertility clinic with a four-year history of primary infertility. She has never conceived despite regular unprotected intercourse. Her husband's semen analysis is normal. Her menstrual cycles have become progressively lighter over the past two years, and her last period was scanty. She has no fever, night sweats, or weight loss. A routine chest X-ray shows a small calcified hilar lymph node. Hysterosalpingography (HSG) reveals bilateral tubal block at the cornual region with a beaded, irregular appearance of both tubes. Endometrial biopsy on day 22 shows epithelioid granulomas with Langhans giant cells and central caseation on histopathology. This is genital tuberculosis — a disease that announces itself through its consequences (infertility, menstrual changes) rather than through the fever and cough we associate with TB. Understanding its pathogenesis, diagnosis, and treatment is essential for every gynaecologist practising in India.
WHY THIS MATTERS
India carries approximately 25% of the global tuberculosis burden (WHO 2022), and genital TB is estimated to account for 5–10% of all TB cases in India. Among women presenting with infertility, studies from major Indian centres (AIIMS, PGI Chandigarh) report genital TB in 4–16% of laparoscopic evaluations — and in some series it is found in up to 40% of women diagnosed with tubal-factor infertility. This makes genital TB a major, and often missed, cause of infertility in India. The clinical importance extends beyond fertility: endometrial TB causes intrauterine adhesions (Asherman syndrome) and recurrent pregnancy loss; tubal TB can mimic ectopic pregnancy, ovarian mass, or chronic PID. Because the symptoms are often non-specific and the disease is paucibacillary (few organisms in genital specimens), diagnosis requires a combination of histopathology, culture, and increasingly, molecular tests. The clinician who maintains a high index of suspicion in any woman with infertility and a history of TB exposure or immunosuppression will diagnose this condition where others miss it.
RECALL
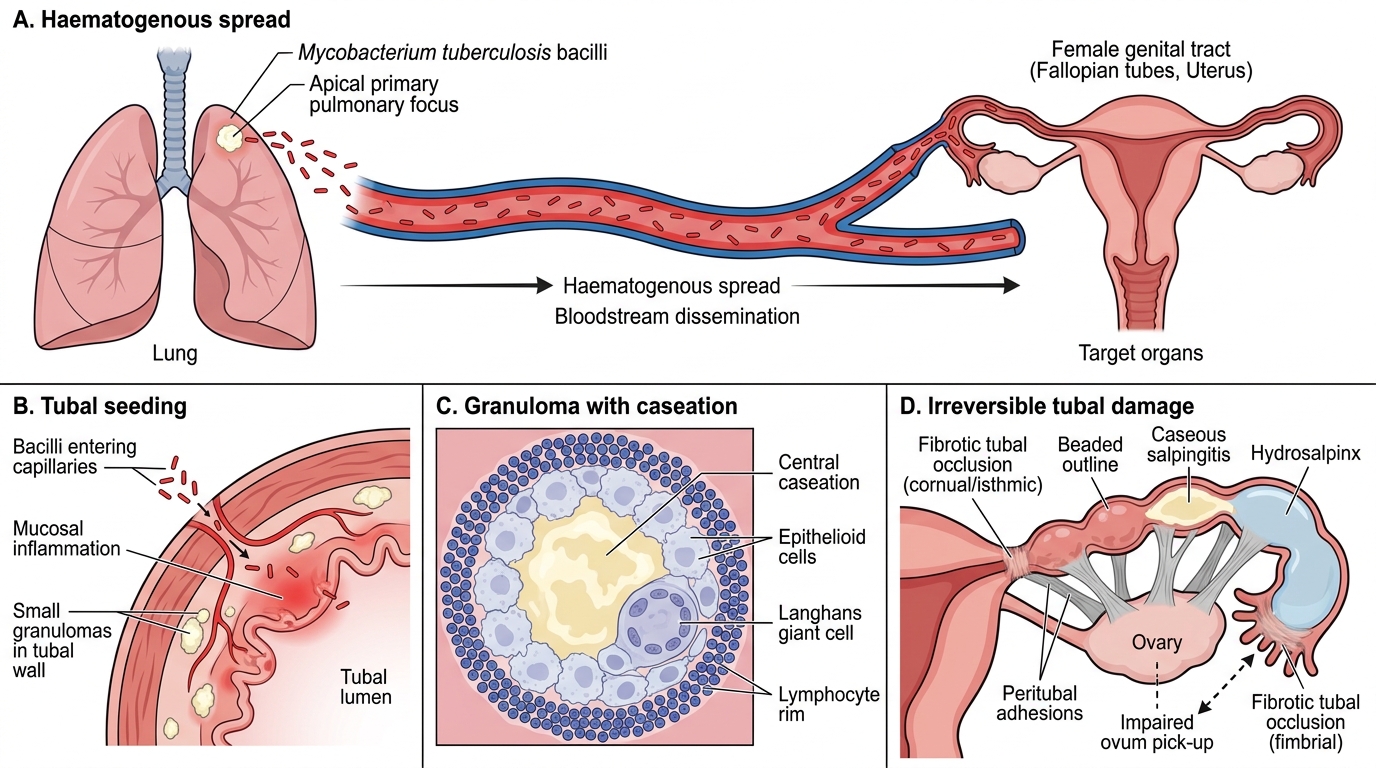
Before proceeding, activate your prior knowledge of tuberculosis. Recall from Medicine and Microbiology: Mycobacterium tuberculosis is an acid-fast bacillus (AFB) — it does not stain by standard gram stain but is identified by the Ziehl-Neelsen technique (carbol fuchsin with acid-alcohol decolourisation). TB infection begins with inhalation of droplet nuclei, primary focus (Ghon's focus) forms in the lung, and spreads to hilar lymph nodes forming the primary complex. In the majority, the primary complex heals by calcification. However, if haematogenous spread occurs before immunity is established — or during re-activation — bacilli can seed any organ, including the fallopian tubes. From Pathology, recall the structure of a tuberculous granuloma: central caseation necrosis surrounded by epithelioid macrophages and Langhans giant cells (peripheral nuclei in horseshoe pattern), with a rim of lymphocytes. This histological pattern is the hallmark of TB and, when found in the endometrium or tube, is diagnostic of genital TB.
Clinical Presentation of Genital Tuberculosis
Genital tuberculosis is characteristically a silent disease — it causes progressive, irreversible damage to the fallopian tubes and endometrium over months to years while the patient remains largely asymptomatic or attributes her symptoms to other causes. By the time she presents to a gynaecologist, the structural damage to the reproductive tract may already be complete and irreversible. This insidious natural history is what makes genital TB fundamentally different from other pelvic infections: there is no acute febrile episode, no dramatic presentation, no obvious point of first-contact diagnosis. The disease is identified most often in women of reproductive age — typically 20–40 years — precisely the age group in which the consequences of infertility carry the greatest personal and social weight. In India, the clinical context is critical: a young woman with primary infertility, progressively scanty periods, and a history of TB exposure in the household, combined with a calcified hilar node on chest X-ray, should trigger immediate investigation for genital TB. The majority of patients in India have no active pulmonary disease at the time of genital TB diagnosis — the primary focus has already healed, but haematogenous seeding of the tubes occurred silently years earlier.
The clinical presentations of female genital TB range across a spectrum:
- Primary infertility — the single commonest presentation, accounting for 45–60% of cases. The tubes are damaged by the tuberculous process (bilateral cornual block, peritubal adhesions, hydrosalpinx) before the woman ever attempts conception. There are no symptoms pointing to the diagnosis.
- Menstrual irregularities — hypomenorrhoea (scanty periods) and oligomenorrhoea are characteristic of endometrial TB; amenorrhoea (complete cessation) may develop as the endometrium is progressively replaced by fibrous tissue. Menorrhagia is less common but can occur from local endometrial irritation in early disease.
- Chronic pelvic pain and dyspareunia — resulting from tubo-ovarian masses, adhesions, and peritoneal involvement.
- Constitutional symptoms — low-grade fever, evening rise of temperature, night sweats, and weight loss are classically described but are present in only a minority of patients with genital TB. Their absence does not exclude the diagnosis.
- Vaginal discharge — uncommon; when present, may be serous, blood-stained, or purulent.
- Incidental finding — discovered at laparoscopy for infertility investigation, hysteroscopy, or at operation for a presumed pelvic mass.
On examination, findings are often minimal. There may be a pelvic mass (tubo-ovarian abscess or 'cold' tubo-ovarian mass), tenderness on bimanual examination, or thickening of the adnexae. The absence of acute inflammatory signs despite adnexal pathology — the 'cold' nature of tuberculous pelvic disease — should raise suspicion.
Pathology and Pathogenesis
The pathogenesis of female genital TB follows a consistent sequence that begins in the lung and ends in the reproductive tract. Understanding this sequence explains the anatomical distribution of the disease, why the fallopian tube is almost universally involved, and why treatment with ATT can eradicate the bacteria but cannot reverse the structural damage already done.
Route of spread: The primary route is haematogenous — bacilli released from the primary pulmonary focus (or reactivated latent pulmonary focus) circulate in the blood and seed the fallopian tubes during a period of bacteraemia. This is why genital TB occurs predominantly in women of reproductive age whose primary pulmonary infection was either subclinical or occurred years earlier, and why the patient may have no active lung disease at the time of diagnosis. Less commonly, the peritoneum is involved first (from mesenteric lymph nodes or ileocaecal TB), and the tubes are seeded secondarily via direct peritoneal spread. Lymphatic spread from pelvic lymph nodes is another minor route. Direct spread from the rectum or bladder (in TB of those organs) is rare.
Sites of involvement (in order of frequency):
- Fallopian tubes (~90–100% of cases): the tubes are seeded first, and almost always bilaterally. The haematogenous bacilli lodge in the tubal epithelium, particularly at the ampullary and fimbrial ends. The acute phase shows mucosal oedema and hyperaemia; a chronic granulomatous process follows.
- Endometrium (~50–60%): seeded from the tubes by descending spread via the tubal lumen. TB endometritis is patchy — the functionalis layer is shed with each menstruation, so the infection seeds from the basalis. Histology shows the characteristic granulomas in the endometrial stroma.
- Ovaries (~20–30%): usually a 'cold' tubo-ovarian abscess or periovarian adhesions; rarely primary ovarian TB.
- Cervix (~5–15%): can mimic carcinoma clinically — ulcerative or papillary lesion; biopsy is diagnostic.
- Vulva/vagina: rare.
Haematogenous Spread of Tuberculosis to the Fallopian Tube
Pathological consequences in the tube: The granulomatous inflammation causes progressive destruction of the tubal epithelium and wall. Caseation may lead to a caseous salpingitis (a tube filled with cheesy caseous material). The tubal lumen becomes progressively obstructed — at the cornual end (isthmic block), within the tube, or at the fimbrial end (fimbrial occlusion with hydrosalpinx). Peritubal adhesions from peritoneal involvement further impair ovum pick-up. These structural changes are largely irreversible — ATT kills the bacilli but cannot rebuild the destroyed epithelium or re-open a fibrosed tube. This is the fundamental clinical reality that explains the poor fertility outcomes even after successful ATT.
SELF-CHECK
A 26-year-old woman with primary infertility undergoes laparoscopy. The surgeon notes bilateral 'beaded' fallopian tubes with multiple white nodules on the tubal surface, dense adnexal adhesions, and peritoneal deposits. Endometrial curettage histology shows epithelioid granulomas with Langhans giant cells and caseation. Which diagnosis is confirmed?
A. Endometriosis
B. Chlamydial salpingitis
C. Female genital tuberculosis
D. Peritoneal carcinomatosis
Reveal Answer
Answer: C. Female genital tuberculosis
The combination of bilateral beaded/nodular tubes with peritubal adhesions, peritoneal deposits, and — critically — endometrial histology showing epithelioid granulomas with Langhans giant cells and central caseation is pathognomonic of genital tuberculosis. Endometriosis causes chocolate cysts and powder-burn lesions; chlamydial salpingitis causes acute suppurative inflammation without granulomas; carcinomatosis has malignant cells on biopsy. Granulomas with caseation = TB until proven otherwise.
Diagnosis and Investigations
Diagnosing genital tuberculosis is challenging because the disease is paucibacillary — the number of organisms in genital specimens is low — and the clinical presentation is non-specific. No single test has sufficient sensitivity to exclude the diagnosis, and diagnosis often requires a combination of histopathology, microbiological culture, and molecular testing, interpreted in the context of the clinical picture and epidemiological risk. A high index of suspicion is the clinician's most important diagnostic tool.
Endometrial biopsy (histopathology and culture) — the most important investigation:
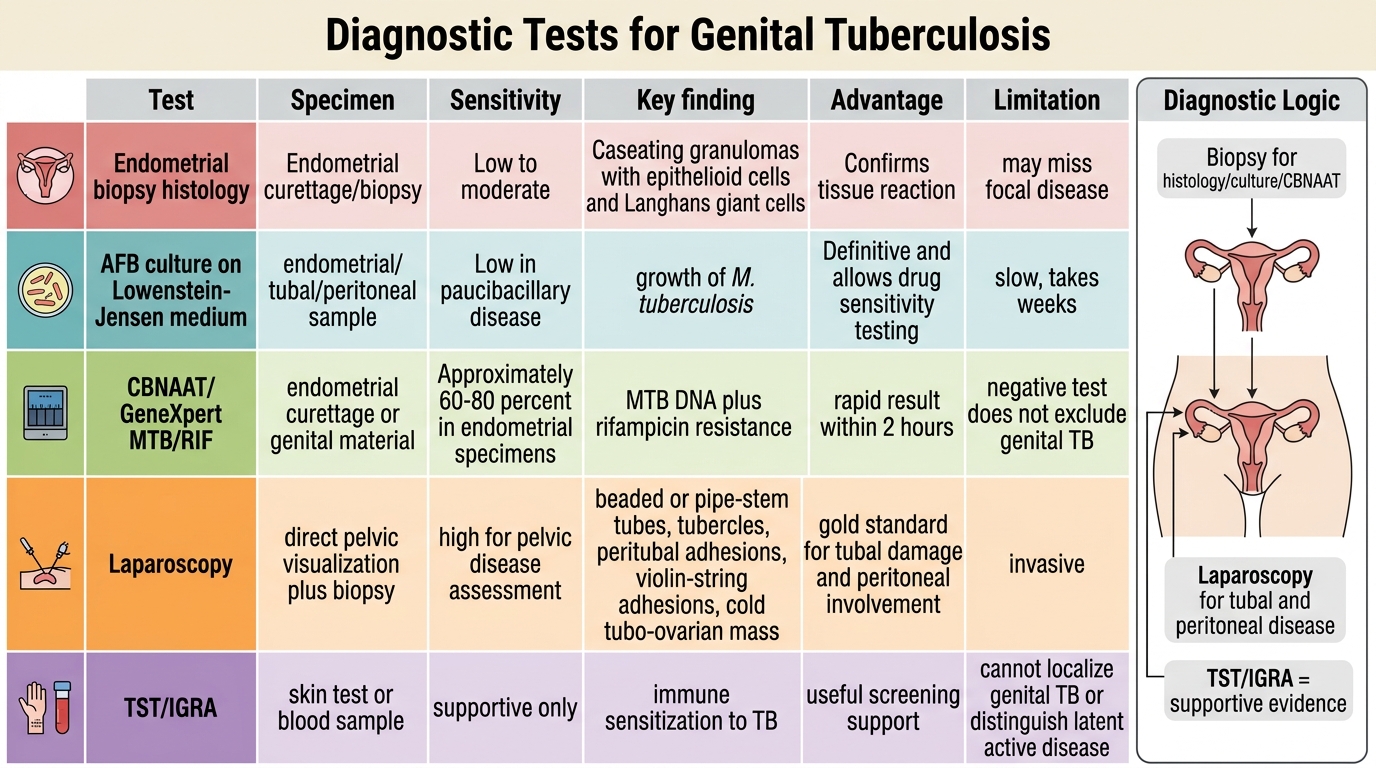
Endometrial curettage performed in the pre-menstrual phase (day 21–25 of the cycle) — when the endometrial bacillary load is maximal — provides material for both histopathology and culture. Histology showing epithelioid granulomas with Langhans giant cells and caseating necrosis in the endometrial stroma is diagnostic. Culture of the specimen on Löwenstein-Jensen (LJ) medium (or BACTEC/MGIT liquid culture) takes 6–8 weeks but allows drug sensitivity testing. A single endometrial biopsy has sensitivity ~60–70%; repeating or combining with laparoscopic specimens increases yield.
Diagnostic Tests for Genital Tuberculosis
CBNAAT (Cartridge-Based Nucleic Acid Amplification Test — GeneXpert MTB/RIF): The most important advance in recent TB diagnostics. Applied to endometrial curettage specimen or other genital material, CBNAAT detects M. tuberculosis DNA and simultaneously tests for rifampicin resistance (a proxy for multidrug resistance, MDR-TB). Sensitivity ~60–80% in endometrial specimens (lower in paucibacillary disease); results within 2 hours. Endorsed by WHO and RNTCP for genital TB diagnosis. Negative CBNAAT does NOT exclude genital TB.
Laparoscopy: Provides direct visualisation of the pelvic organs and is the gold standard for assessing tubal damage and peritoneal involvement. Characteristic laparoscopic findings include: bilateral beaded or 'pipe-stem' tubes; tubal nodularity (miliary tubercles); peritubal adhesions; 'violin-string' adhesions across the pelvis; peritoneal tubercles (white miliary deposits); and 'cold' tubo-ovarian masses without the acute erythema/pus of pyogenic PID. Biopsy specimens from tubal or peritoneal deposits can be sent for histopathology, culture, and CBNAAT.
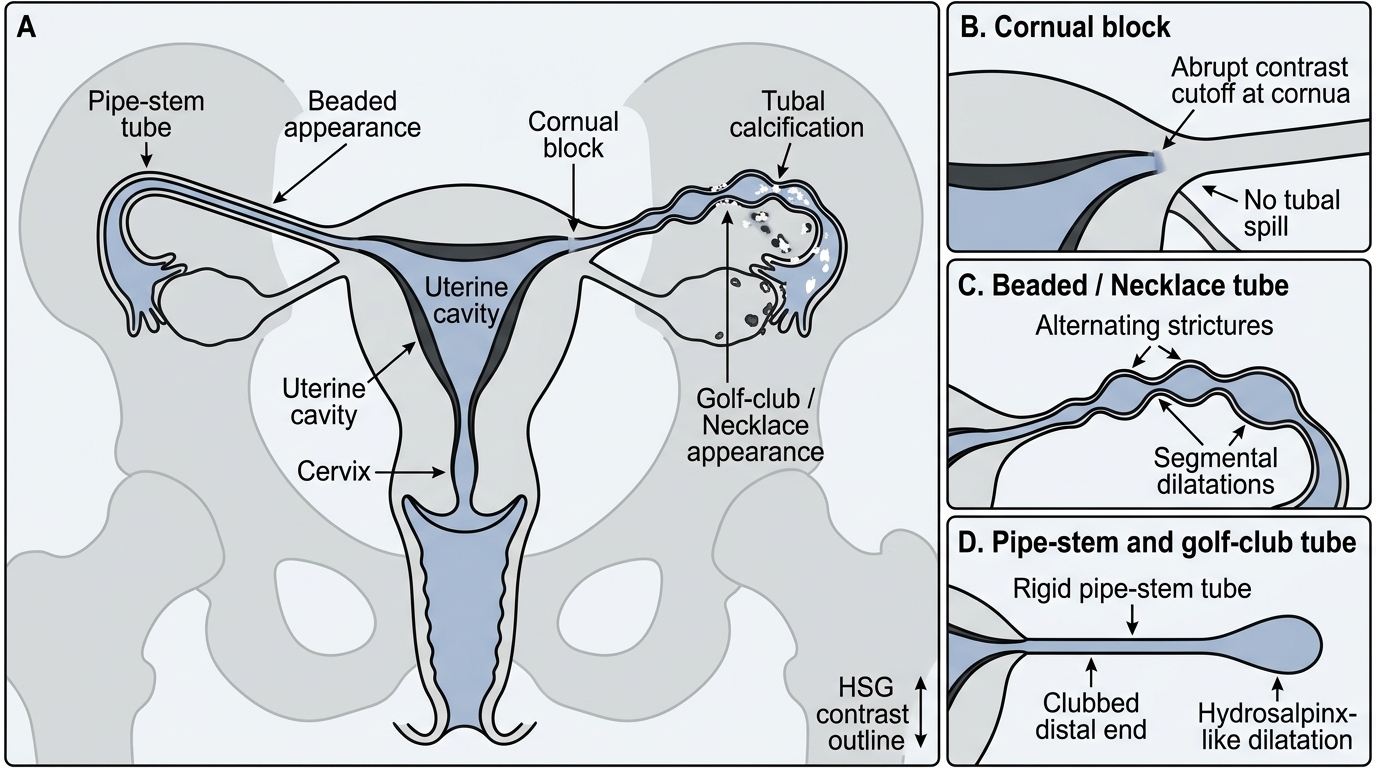
Hysterosalpingography (HSG): Demonstrates tubal abnormalities and intrauterine pathology. Characteristic findings include: bilateral cornual block; 'pipe-stem' (lead-pipe) rigid tubes; beaded or irregular tubal outline; 'golf-club' or 'necklace' appearance; calcification in the tubes or pelvis; and intrauterine filling defects or Asherman-type synechiae from endometrial scarring.
HSG Findings in Genital Tuberculosis
Tuberculin skin test (TST/Mantoux) / IGRA (Interferon-Gamma Release Assay): A positive TST (induration ≥10 mm at 48–72 h) or a positive IGRA (QuantiFERON-TB Gold) indicates latent or past TB infection — not active disease per se. Supportive but not diagnostic; false-negatives occur in immunocompromised patients.
AFB smear (Ziehl-Neelsen stain): Directly stains acid-fast bacilli in specimens — rapid but has very low sensitivity in paucibacillary genital specimens. Positive smear in genital material is strongly suggestive but negative smear does not exclude TB.
Other investigations: Complete blood count (raised ESR, lymphocytosis); chest X-ray (hilar lymphadenopathy, calcified primary complex, active pulmonary TB); ultrasound pelvis (tubo-ovarian masses, free fluid, peritoneal nodules).
SELF-CHECK
Endometrial curettage is performed on day 22 of the cycle in a woman with suspected genital TB. CBNAAT returns negative. What is the correct interpretation?
A. Genital TB is excluded — CBNAAT has near-100% sensitivity
B. A negative CBNAAT does not exclude genital TB; histopathology and culture results are still required
C. A second curettage on day 5 of the next cycle should be performed to increase sensitivity
D. The diagnosis should be changed to chronic PID as TB is ruled out
Reveal Answer
Answer: B. A negative CBNAAT does not exclude genital TB; histopathology and culture results are still required
CBNAAT sensitivity in endometrial specimens is approximately 60–80% — it is NOT 100%, particularly in paucibacillary genital TB. A negative CBNAAT does not exclude the diagnosis. Histopathology (granulomas + Langhans cells + caseation) and culture (LJ medium or BACTEC) remain essential and must be interpreted alongside CBNAAT. Pre-menstrual curettage (day 21–25) is already the optimal timing — day 5 would be in the proliferative phase with lower bacterial load. Clinical judgement, laparoscopy, and the full diagnostic picture must be integrated.