Page 9 of 18
OG27.2 | Genital Tuberculosis — SDL Guide (Part 2)
Management — ATT and Fertility Outcomes
The management of genital tuberculosis is based on the same anti-tubercular therapy (ATT) principles as pulmonary TB, because the causative organism — Mycobacterium tuberculosis — is identical and its pharmacological sensitivity profile does not differ by the anatomical site of infection. The same drugs penetrate the genital tract and achieve bactericidal concentrations in infected tissue. ATT is definitively curative for the bacterial component of the disease: it eliminates the mycobacteria from the fallopian tubes and endometrium, arrests the ongoing granulomatous inflammation, prevents further tissue destruction, and prevents bacteraemic seeding of other organs. The rationale for treating genital TB is therefore not only to restore fertility (which may or may not be achievable) but also to eliminate a systemic infectious disease, prevent progression to other organ involvement, and reduce community transmission. However, the clinician must be unequivocal about one critical limitation: ATT cannot reverse structural damage that has already occurred. Fibrosed tubes, obliterated tubal lumina, and Asherman-type endometrial scarring are irreversible pathological changes — they represent scar tissue, not active infection, and no antibiotic dissolves scar. This is the most important concept governing post-treatment fertility counselling: bacteriological cure and fertility restoration are two different outcomes.
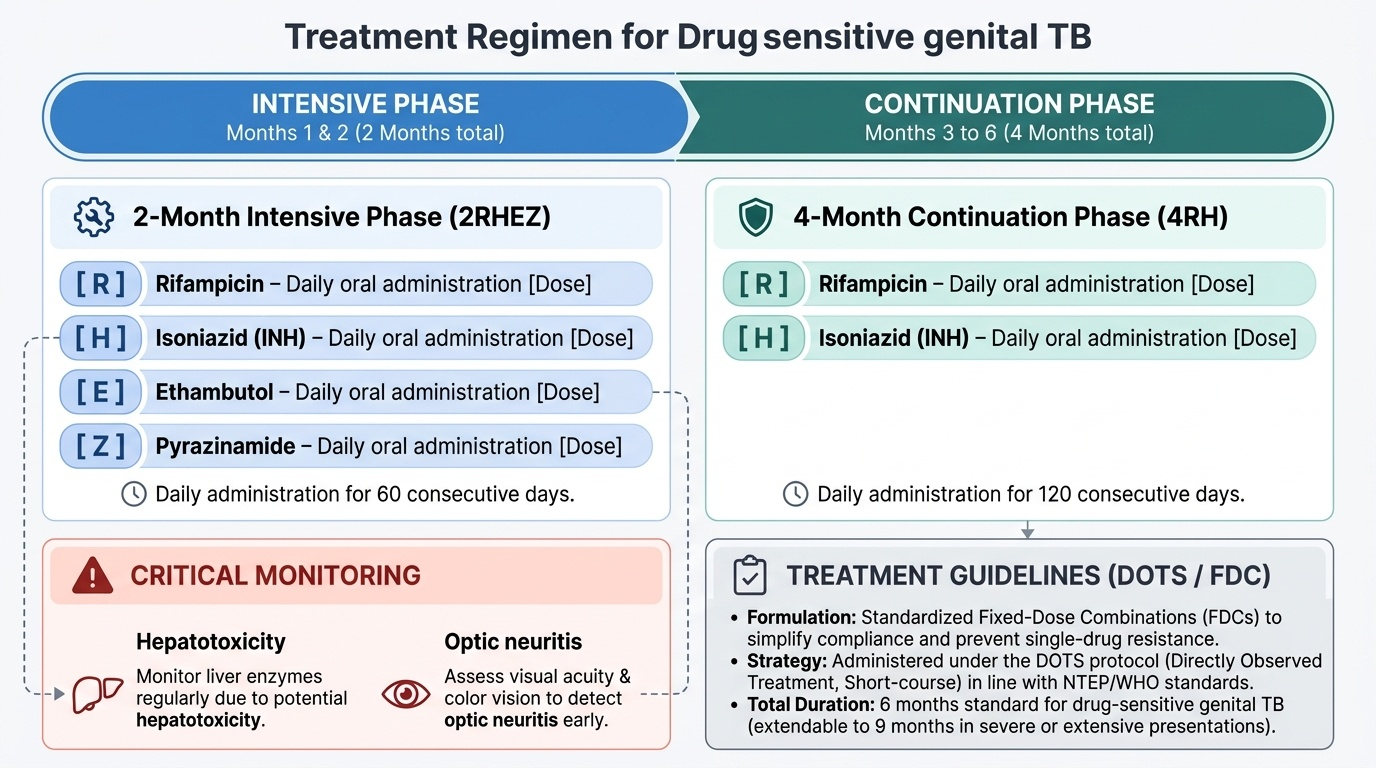
Standard first-line ATT regimen for drug-sensitive genital TB (RNTCP/WHO Category I):
Provided image
- Intensive phase (2 months): Rifampicin + Hisoniazid (INH) + Ethambutol + Pyrazinamide = RHEZ (or 2RHEZ). All four drugs are given daily.
- Continuation phase (4 months): Rifampicin + Hisoniazid = RH (or 4RH). Two drugs, daily.
- Total duration: 6 months for drug-sensitive, non-severe genital TB. Some authorities extend to 9 months for severe or extensive genital disease, but 6 months is standard per current NTEP/WHO guidelines.
- Drugs are given as Fixed-Dose Combinations (FDCs) under DOTS (Directly Observed Treatment, Short-course) in India's NTEP programme.
- Monitoring: liver function tests (rifampicin + INH are hepatotoxic), visual acuity/colour vision (ethambutol — monitor for optic neuritis), uric acid (pyrazinamide).
- Drug-resistant TB (MDR-TB): if rifampicin resistance is detected on CBNAAT, refer to MDR-TB treatment programme — longer regimens (18–20 months) with second-line drugs (fluoroquinolones, bedaquiline, linezolid).
Fertility outcomes after ATT — the key counselling points:
The prospect of achieving a pregnancy after ATT for genital TB depends critically on the extent of tubal and endometrial damage at the time treatment is started. Published outcome data from Indian series:
- Endometrial TB predominant (tubes relatively preserved): pregnancy rate 20–40% after ATT; these patients have the best outcomes.
- Unilateral tubal TB or early bilateral disease: pregnancy rate 10–20%.
- Bilateral tubal occlusion or extensive tubal destruction: pregnancy rate <5–10% by natural conception. ATT cures the infection but cannot re-open fibrosed tubes.
- IVF-ET is the realistic option for women with severe bilateral tubal TB. However, IVF outcomes are also suboptimal in genital TB because endometrial receptivity may be permanently impaired even after bacteriological cure. IVF pregnancy rates in genital TB are lower than in non-TB tubal occlusion.
Surgical management: The role of surgery is limited. Surgery is indicated for:
- Large tubo-ovarian masses that do not resolve with ATT
- Suspicion of malignancy co-existing with TB
- Resistant/recurrent disease
Tuboplasty (surgical reconstruction of the tubes) has a very poor success rate in TB-damaged tubes and is generally not recommended.
Intrauterine adhesions (Asherman syndrome) from endometrial TB may require hysteroscopic adhesiolysis — with guarded prognosis for endometrial recovery.
SELF-CHECK
A 30-year-old woman completes 6 months of ATT for genital TB confirmed on histopathology. Post-treatment HSG shows bilateral tubal block at the cornual end unchanged from the pre-treatment HSG. She asks about her chances of pregnancy. What is the most accurate counselling?
A. Pregnancy will occur naturally within 1 year now that the infection is cured
B. ATT will dissolve tubal fibrosis over 6-12 months post-treatment — continue to wait
C. ATT has eliminated the bacteria but bilateral tubal occlusion is structural and irreversible; IVF-ET is the realistic option
D. She should repeat another 6-month ATT course to achieve tubal patency
Reveal Answer
Answer: C. ATT has eliminated the bacteria but bilateral tubal occlusion is structural and irreversible; IVF-ET is the realistic option
ATT cures the mycobacterial infection — it kills the bacteria and prevents further tissue destruction. However, the fibrosis and structural occlusion that the tuberculous process has already caused are irreversible: no drug dissolves established fibrous scar tissue. Bilateral cornual block on post-treatment HSG confirms bilateral tubal occlusion that will not resolve spontaneously. The bacteria are gone, but the structural damage remains. IVF-ET is the appropriate management for this situation, though endometrial receptivity may also be reduced. A second course of ATT would serve no purpose — the bacteria are already eradicated.
Long-Term Implications and Prevention
The long-term implications of genital tuberculosis extend considerably beyond the immediate question of fertility and span three distinct domains: the irreversible structural consequences for the endometrium and adnexa, the biological risk of disease reactivation under conditions of impaired immunity, and the public health obligation to prevent transmission and detect secondary cases. Each of these dimensions requires active clinical attention during and after ATT — the clinician's role does not end when the six-month course is completed. A woman who has received ATT for genital TB faces the possibility of permanent infertility, the need for IVF referral, the risk of Asherman syndrome compromising any future pregnancy, and the lifelong background risk of TB reactivation if she ever becomes immunosuppressed. Addressing these implications honestly, sensitively, and at the right time in the therapeutic relationship is as important as prescribing the correct drug regimen. The clinician must also consider the public health dimension: genital TB does not arise in isolation — the patient's household contacts may carry latent TB infection and should be screened and considered for isoniazid preventive therapy.
Irreversible structural sequelae:
- Tubal occlusion and peritubal adhesions: the principal cause of infertility; structural, permanent, not reversible by ATT. Extent of pre-treatment damage determines prognosis.
- Endometrial fibrosis and Asherman syndrome: extensive endometrial TB leads to intrauterine synechiae (adhesions), obliterating the uterine cavity. Clinical consequence: amenorrhoea, oligomenorrhoea, recurrent miscarriage, and failed implantation. Hysteroscopic adhesiolysis can partially restore the cavity but endometrial receptivity remains impaired.
- Ovarian damage: tubo-ovarian masses may require surgical removal; premature ovarian insufficiency from bilateral ovarian destruction is a rare but recognised sequela.
Risk of reactivation:
Genital TB, like all extrapulmonary TB, carries a risk of reactivation — particularly with immunosuppression (HIV infection, corticosteroids, anti-TNF therapy, malnutrition). Patients should be counselled to complete the full ATT course, complete their DOTS, and report any recurrence of symptoms. After completing ATT, bacteriological cure is confirmed by symptom resolution, resolution of constitutional features, and repeat culture negativity (if applicable). Structural follow-up (repeat HSG/hysteroscopy) is performed to document post-treatment changes.
Prevention:
- BCG vaccination at birth is the primary preventive measure — BCG significantly reduces the risk of severe and disseminated TB in children, including haematogenous seeding of extrapulmonary sites. India's Universal Immunisation Programme mandates BCG at birth.
- Contact tracing and treatment: household and close contacts of active TB cases should be screened (TST/IGRA, chest X-ray) and given isoniazid preventive therapy (IPT) if indicated.
- Early diagnosis and complete treatment of pulmonary TB prevents haematogenous dissemination to the genital tract.
- Nutrition and HIV prevention: malnutrition and HIV are the two most important risk factors for TB progression from latent to active disease; addressing these reduces the overall TB burden.
CLINICAL PEARL
The key insight in genital TB: treatment cures the infection but NOT the damage. Many students (and some clinicians) make the error of reassuring a woman with bilateral tubal TB that 'the treatment will sort out the fertility problem.' This is factually wrong and potentially cruel — it delays appropriate referral for IVF. ATT eliminates the mycobacteria; it cannot rebuild destroyed tubal epithelium, re-open fibrosed cornual segments, or repair Asherman-scarred endometrium. The counselling message must be clear and honest: we are treating the infection to prevent further damage and systemic spread; the structural damage already present determines fertility prognosis, and in bilateral tubal disease, IVF is the appropriate path. Pre-menstrual endometrial curettage (day 21–25) is the optimal timing for biopsy — this is a common examination question.
Self-Assessment
You have now worked through the complete clinical arc for genital tuberculosis — from its insidious clinical presentation dominated by infertility and menstrual change, through the haematogenous pathogenesis and granulomatous histopathology that explain its anatomical distribution, the diagnostic challenge of a paucibacillary disease requiring a combination of histopathology, culture, CBNAAT, and laparoscopy, and the crucial management principle that ATT cures the infection but cannot reverse established structural damage. Before attempting the question below, confirm your recall of three key facts: (1) which site is most commonly affected in female genital TB and in what percentage, (2) why is endometrial curettage timed to the pre-menstrual phase, and (3) what is the prognosis for spontaneous pregnancy after ATT in a woman with bilateral cornual tubal block.
SELF-CHECK
Which site is most commonly affected in female genital tuberculosis, and what is the approximate frequency of its involvement?
A. Endometrium — affected in nearly all cases (90-100%)
B. Fallopian tubes — affected in nearly all cases (90-100%)
C. Ovaries — affected in nearly all cases (90-100%)
D. Cervix — affected in nearly all cases (90-100%)
Reveal Answer
Answer: B. Fallopian tubes — affected in nearly all cases (90-100%)
The fallopian tubes are the primary and most consistently affected site in female genital TB, involved in approximately 90–100% of cases. They are seeded first by haematogenous spread. The endometrium is involved secondarily in about 50–60% of cases (by descending spread from the tube), ovaries in 20–30%, and the cervix in 5–15%. Vulva and vagina are rarely affected. This anatomical hierarchy — tubes first — explains why bilateral tubal damage is the dominant pathological finding and tubal-factor infertility the dominant clinical consequence.