Page 10 of 24
OG28.4 | Assisted Reproduction Techniques — SDL Guide
Learning Objectives
- Enumerate the main assisted reproduction techniques and state the indication for each
- Describe the steps of an IVF cycle from controlled ovarian stimulation to embryo transfer
- Distinguish between IVF and ICSI in terms of indication and laboratory technique
- State age-stratified IVF success rates and describe how female age influences treatment decisions
- Outline the regulatory framework governing ART practice in India (ART Regulation Act 2021; Surrogacy Regulation Act 2021)
INSTRUCTIONS
Assisted reproduction techniques represent the end of the infertility treatment spectrum — available when all simpler measures have failed or when the underlying cause (bilateral tubal block, azoospermia, severe endometriosis) makes natural conception impossible. For a final-year student, understanding ART at a conceptual and clinical level — what each technique does, who it is for, what the realistic success rates are, and what the legal and ethical framework in India demands — is both a curriculum requirement and a foundation for evidence-based counselling of infertile couples.
References
- DC Dutta's Textbook of Gynaecology, 8th edition, Ch 18 (ART) (textbook)
- Shaw's Textbook of Gynaecology, 17th edition, Ch 24 (ART) (textbook)
- NICE Fertility Guideline CG156, updated 2017 — IVF section (guideline)
- Assisted Reproductive Technology (Regulation) Act 2021, India (legislation)
- Surrogacy (Regulation) Act 2021, India (legislation)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ritu and Anand have been investigated for three years. Ritu has bilateral tubal occlusion confirmed at laparoscopy, with hydrosalpinges bilaterally that have already been treated with salpingectomy. Anand's semen analysis shows a concentration of 3 million/mL with 15% progressive motility — moderate oligoasthenospermia. They have no children. Their gynaecologist says: 'You will need IVF with ICSI.' For Ritu and Anand, this is both terrifying and hopeful. As the clinician, you need to explain: what exactly happens during IVF and ICSI, what are the realistic chances of success, what are the risks, and what does the law in India say about this treatment? This SDL provides the knowledge base for that conversation.
WHY THIS MATTERS
Assisted reproduction techniques have transformed the landscape of infertility treatment, enabling conception in situations that were previously hopeless: absent tubes, severe male factor azoospermia, poor ovarian reserve, and genetic disease in the embryo. In India, the ART sector has grown into one of the largest in the world, with thousands of IVF cycles performed annually. As a final-year student entering clinical practice, you will encounter patients who have either undergone ART or are considering it, and you will need to counsel them accurately — about success rates (which are age-dependent and often overestimated by patients), the physical and emotional demands of treatment, the legal protections afforded by the ART Regulation Act 2021, and the clear prohibition on sex selection under the PCPNDT Act.
RECALL
Recall from Physiology: fertilisation normally occurs in the ampulla of the fallopian tube within 12–24 hours of ovulation; the fertilised egg undergoes cleavage divisions over 3–5 days as it travels to the uterus, arriving as a morula (day 3–4) and then a blastocyst (day 5–6); implantation occurs on day 6–10 post-fertilisation in the receptive endometrium. ART bypasses the requirement for a patent fallopian tube by achieving fertilisation in the laboratory (in vitro) and placing the embryo directly into the uterine cavity. Recall also from Physiology: the acrosome reaction in sperm — triggered by zona pellucida contact — releases enzymes that digest the zona, allowing one sperm to penetrate the oocyte; ICSI bypasses this step entirely by injecting the sperm directly into the cytoplasm.
Clinical Presentation and Indications for ART
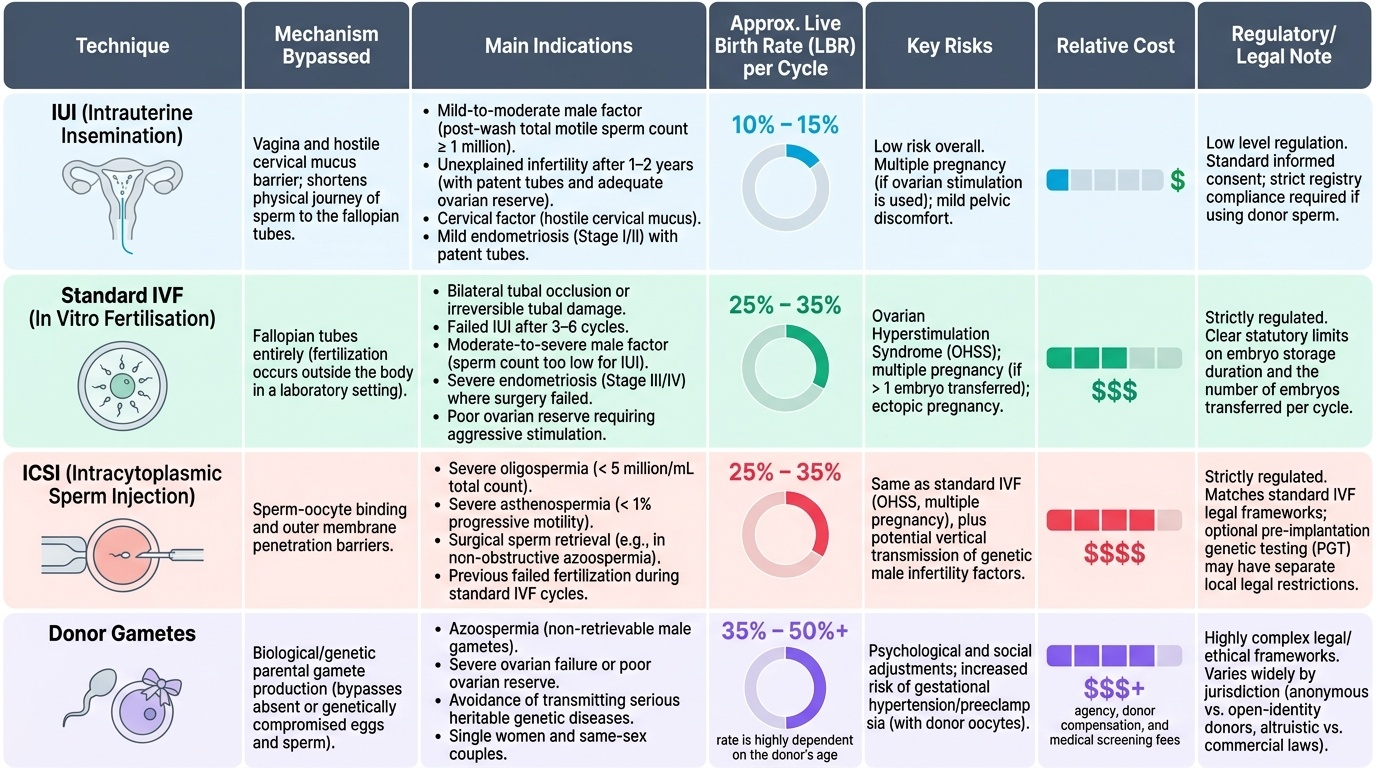
The decision to proceed to ART is made when simpler, less invasive treatments have either failed or are clearly unsuitable for the identified cause of infertility. This decision is not arbitrary — it is driven by the specific barrier to natural conception that has been identified through systematic investigation, and matching the ART technique to that barrier is the foundation of rational, evidence-based management. ART is not a homogeneous category: intrauterine insemination, standard IVF, ICSI, and donor gamete programmes address fundamentally different physiological problems, carry different success rates and risks, involve very different levels of physical and financial burden, and have different regulatory frameworks. A couple with bilateral tubal block requires IVF; a couple with mild male factor and patent tubes may need only IUI; a couple with non-obstructive azoospermia requires IVF with surgical sperm retrieval and ICSI. Conflating these or applying a single approach to all couples is poor medicine. ART represents a spectrum of interventions of increasing complexity, cost, and invasiveness, and matching the technique to the indication is fundamental to rational management.
Intrauterine insemination (IUI) is the least invasive ART technique and is indicated when:
- Mild to moderate male factor: post-wash total motile sperm count ≥1 million (concentration ≥5 million/mL pre-wash)
- Unexplained infertility after 1–2 years, when tubes are patent and ovarian reserve is adequate
- Cervical factor: hostile cervical mucus reducing sperm penetration
- Mild endometriosis (stage I/II) with patent tubes
- Donor insemination: for azoospermia (non-retrievable), single women, same-sex female couples
In vitro fertilisation (IVF) is indicated when:
- Bilateral tubal occlusion (irreversible or surgically unfeasible)
- Failed IUI after 3–6 cycles
- Moderate–severe male factor (sperm count too low for IUI but surgical retrieval possible)
- Severe endometriosis (stage III/IV) where surgery has failed or is not appropriate
- Unexplained infertility after 2 years with failed simpler interventions
- Poor ovarian reserve requiring aggressive stimulation and embryo selection
Intracytoplasmic sperm injection (ICSI) is used when:
- Severe oligospermia (<5 million/mL total count) or severe asthenospermia (<1% progressive motility)
- Azoospermia with surgically retrieved sperm (PESA, TESA, micro-TESE)
- Prior IVF fertilisation failure (failed conventional IVF fertilisation despite adequate sperm)
- Frozen sperm (lower motility post-thaw)
- PGT cycles (where biopsy requires confirmation of paternal origin)
Donor gametes:
- Donor oocytes: for premature ovarian insufficiency (POI), poor responders to stimulation (AMH <0.1 ng/mL, AFC <3), Turner syndrome, or women at risk of transmitting genetic disease
- Donor sperm: for obstructive/non-obstructive azoospermia where surgical retrieval fails, or severe genetic conditions
- Embryo donation (rare): for couples with neither viable eggs nor viable sperm
Provided image
Pathophysiology and Basis of ART: Overcoming Natural Barriers to Conception
Each ART technique is designed to bypass a specific anatomical or physiological barrier to conception, and understanding this mapping clarifies why each technique is indicated for its specific cause rather than being interchangeable.
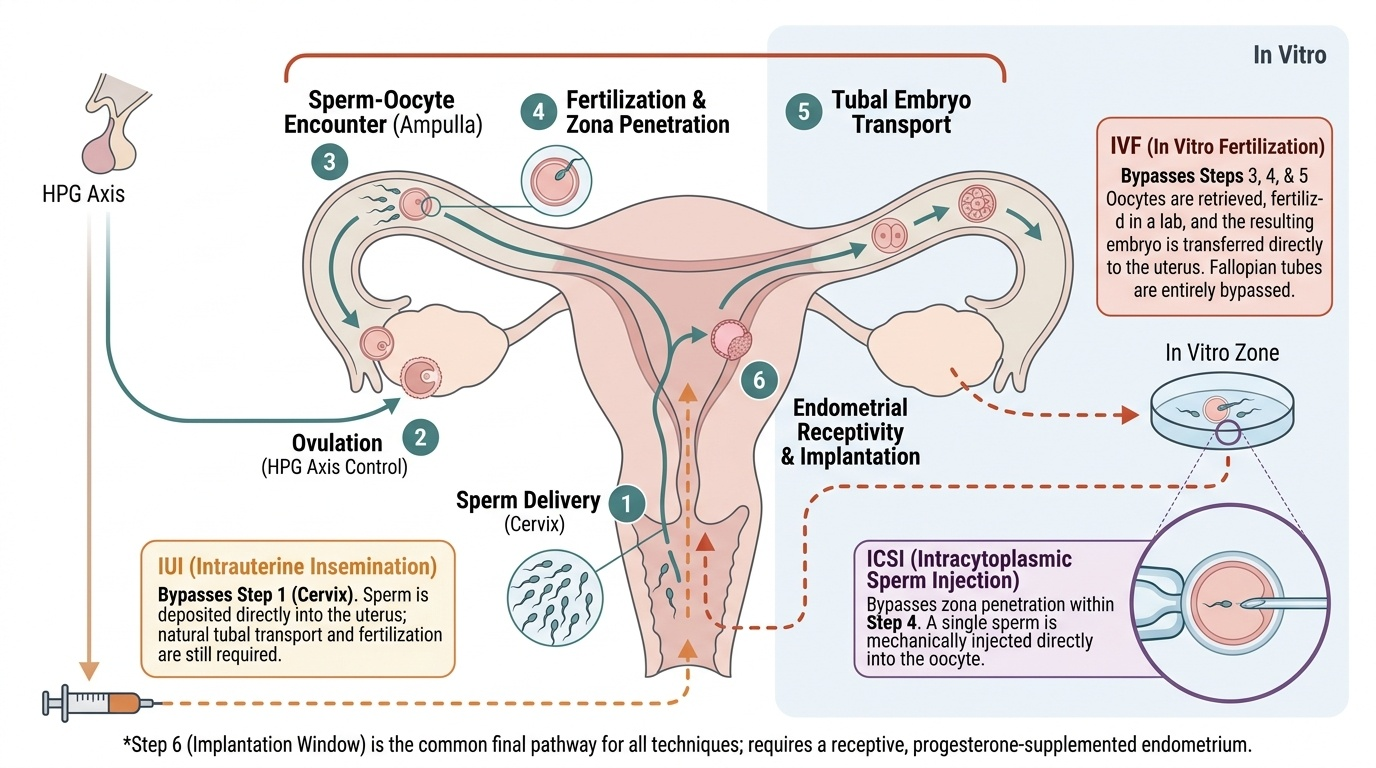
Natural conception requires: (1) sperm delivery to the upper reproductive tract through a patent cervix; (2) ovulation of a mature oocyte; (3) sperm–oocyte encounter in a patent ampulla; (4) acrosome reaction, zona penetration, fertilisation, and formation of a zygote; (5) tubal transport of the developing embryo to the uterine cavity; and (6) endometrial receptivity for implantation. A failure at any one of these steps requires a specific intervention.
IUI addresses step 1 only: it bypasses the cervix and places washed, concentrated, motile sperm directly into the uterine cavity at the time of ovulation, increasing the sperm density available to enter the fallopian tube. It cannot help when the tube is blocked or the sperm count is too low to achieve fertilisation even with direct placement. The sperm must still travel up the tube and fertilise the oocyte naturally.
IVF bypasses steps 3, 4, and 5 simultaneously: it retrieves mature oocytes directly from the ovarian follicles (bypassing the need for tubal transport of the oocyte), fertilises them in a culture dish in the laboratory (bypassing the need for sperm–oocyte encounter in the tube), cultures the resulting embryo for 3–5 days, and transfers it directly into the uterine cavity (bypassing the need for tubal embryo transport). Tubes are entirely irrelevant in IVF — which is why bilateral tubal block is a classic IVF indication.
ICSI addresses a specific failure within step 4: when sperm cannot penetrate the zona pellucida because of inadequate numbers, poor motility, abnormal morphology, or absent acrosome reaction, a single sperm is mechanically injected through the zona and into the oocyte cytoplasm using a glass micropipette under microscopic guidance. ICSI achieves fertilisation rates of approximately 70–80% of injected oocytes regardless of sperm quality, making it transformative for severe male factor infertility.
The implantation window (steps 5–6) is common to all ART techniques: the endometrium must be receptive (oestrogen-primed, progesterone-supplemented, synchronised with the embryo's developmental stage) for implantation to succeed. This is why controlled progesterone supplementation after embryo transfer is universal in ART — the pituitary is suppressed and luteal phase support must be exogenous.
Provided image
SELF-CHECK
A couple presents with 3 years of primary infertility. The woman has patent tubes, regular ovulation, and normal hormones. The man has a semen analysis showing sperm concentration of 2 million/mL with 10% progressive motility. Which ART technique is most appropriate?
A. IUI with husband's sperm — mild male factor responds well to IUI
B. IVF with conventional insemination — the sperm will fertilise oocytes naturally in culture
C. IVF with ICSI — severe oligoasthenospermia requires single sperm injection for reliable fertilisation
D. Donor sperm IUI — the sperm count is too low for any procedure with husband's sperm
Reveal Answer
Answer: C. IVF with ICSI — severe oligoasthenospermia requires single sperm injection for reliable fertilisation
A concentration of 2 million/mL with 10% progressive motility constitutes severe oligoasthenospermia. IUI requires a post-wash total motile count ≥1 million and is suitable for mild–moderate male factor; this case is too severe. Conventional IVF insemination requires adequate sperm density for natural zona penetration, which will fail at this count. ICSI is the technique of choice for severe male factor — it achieves fertilisation in ~70–80% of injected oocytes regardless of sperm quality. Donor sperm is premature before attempting ICSI with husband's sperm.
ART Procedures: IUI, IVF, and ICSI — Steps and Techniques
Understanding the procedural steps of IUI and IVF/ICSI at a conceptual level is essential for counselling patients and for understanding the complications that arise at each stage. Patients who embark on ART face a sequence of clinical encounters — consultations, injections, monitoring scans, procedures under sedation, anxious waiting for fertilisation and embryo development reports, and ultimately a two-week wait after transfer before a pregnancy test. The clinician who can walk a couple through these steps clearly and honestly — explaining what happens at each stage, what the decision points are, and what the options are if a stage does not go as hoped — provides enormous reassurance and enables genuinely informed consent. The procedural descriptions below are written at the level of clinical understanding a final-year student needs: you do not need to know how to perform TVOR or how to manipulate a micropipette, but you do need to understand what happens and why each step matters for the ultimate outcome of a live birth.
IUI procedure:
1. Cycle preparation: either natural cycle (timed to spontaneous LH surge) or mild ovarian stimulation (letrozole or low-dose FSH) to produce 1–2 dominant follicles
2. Semen preparation: the ejaculate is processed by gradient centrifugation or swim-up technique within 1–2 hours of collection to isolate motile sperm and remove seminal plasma, prostaglandins, and non-motile sperm
3. Timing: ovulation is confirmed by USS and LH surge detection; insemination is performed 24–40 hours after hCG trigger or LH surge
4. Insemination: a soft catheter is passed through the cervix into the uterine cavity; 0.3–0.5 mL of prepared sperm suspension is gently deposited
5. Luteal phase support: progesterone pessaries 400 mg vaginally BD for 2 weeks; pregnancy test on day 14
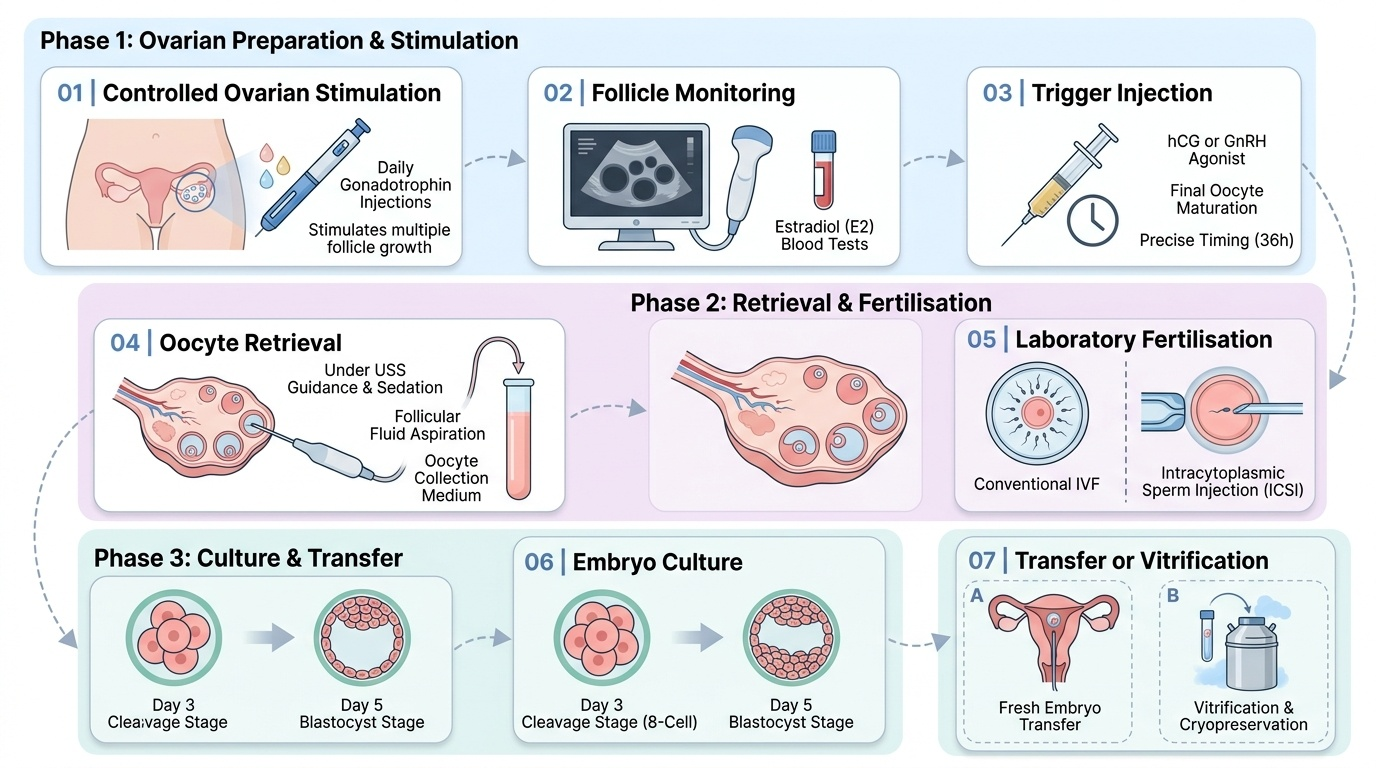
IVF/ICSI procedure — seven key stages:
Stage 1 — Controlled ovarian stimulation (COS): injectable gonadotrophins (rFSH ± rLH or hMG, 150–450 IU/day) are administered from day 2–3 of the cycle, with a GnRH agonist (downregulation protocol — long protocol) or GnRH antagonist (shorter, flexible — preferred for PCOS risk) to prevent premature LH surge. Goal: develop 8–15 mature follicles.
Stage 2 — Monitoring: serial transvaginal USS (days 5, 7, 9+ of stimulation) and serum oestradiol to track follicular development and detect early OHSS.
Stage 3 — Trigger: when ≥3 follicles reach ≥17 mm, final oocyte maturation is triggered with hCG 5,000–10,000 IU IM (conventional) or GnRH agonist (preferred in PCOS/high responders — lower OHSS risk, must be combined with freeze-all strategy).
Stage 4 — Transvaginal oocyte retrieval (TVOR): performed under USS guidance, 34–36 hours after trigger, under conscious sedation or general anaesthesia; a long aspirating needle passed through the vaginal wall into each follicle aspirates follicular fluid; retrieved oocytes are immediately handed to the embryologist.
Stage 5 — Fertilisation (IVF or ICSI): in conventional IVF, 50,000–100,000 processed sperm are placed with each oocyte in culture medium and allowed to fertilise over 16–18 hours; in ICSI, a single morphologically selected sperm is injected directly into the oocyte cytoplasm. Fertilisation is confirmed at 16–18 hours by the appearance of two pronuclei (2PN).
Stage 6 — Embryo culture and selection: embryos are cultured in incubators (controlled CO₂, humidity, temperature) for 3 days (cleavage stage, 6–8 cells) or 5 days (blastocyst — inner cell mass + trophectoderm). Blastocyst transfer is generally preferred as it allows better embryo selection — only embryos capable of sustained development reach blastocyst stage. Optional: preimplantation genetic testing (PGT-A — aneuploidy screening; PGT-M — monogenic disease) via trophectoderm biopsy.
Stage 7 — Embryo transfer or cryopreservation: 1–2 embryos transferred into the uterine cavity via a soft catheter (without anaesthesia); remaining good-quality embryos vitrified (rapid freeze) for future frozen embryo transfer (FET) cycles. Elective single embryo transfer (eSET) is recommended to minimise multiple pregnancy.
Provided image
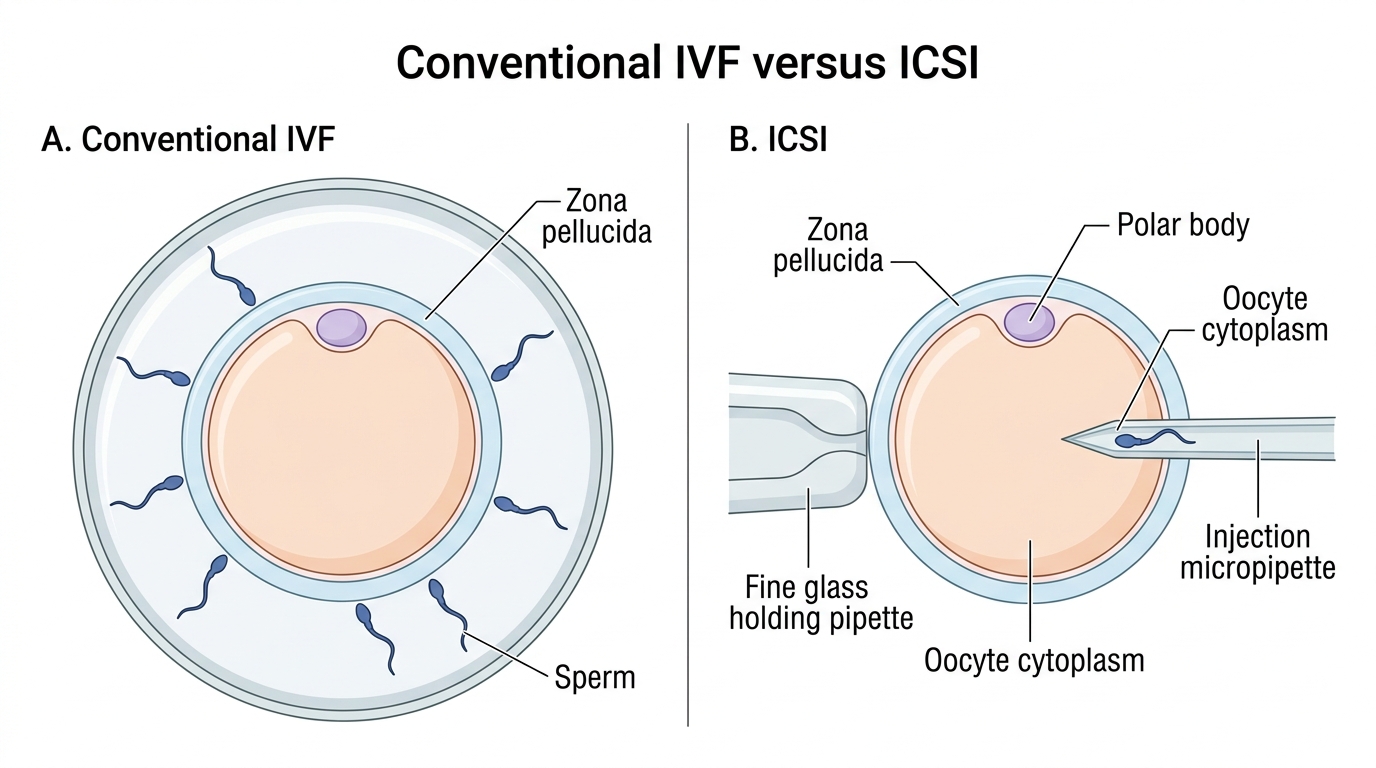
Conventional IVF versus ICSI
SELF-CHECK
In an IVF cycle for a 29-year-old woman with PCOS who is at high risk of OHSS, which trigger and embryo management strategy minimises the risk of severe OHSS while preserving IVF success?
A. hCG 10,000 IU trigger followed by fresh embryo transfer on day 5
B. GnRH agonist trigger followed by freeze-all strategy with frozen embryo transfer in a subsequent cycle
C. hCG 5,000 IU trigger with immediate IUI instead of embryo transfer
D. Cancel the cycle and start a new cycle with lower gonadotrophin dose
Reveal Answer
Answer: B. GnRH agonist trigger followed by freeze-all strategy with frozen embryo transfer in a subsequent cycle
In high-risk PCOS patients undergoing IVF COS, the GnRH agonist trigger replaces hCG for final oocyte maturation. It causes a brief LH/FSH surge that is rapidly cleared, avoiding the prolonged VEGF-stimulating effect of hCG (which persists for 10–14 days). Combined with a freeze-all strategy (no fresh embryo transfer in the stimulated cycle), this virtually eliminates early-onset OHSS risk. Success is maintained as frozen embryo transfer in the subsequent natural or programmed cycle achieves comparable or better outcomes. hCG trigger in a high-risk patient risks severe OHSS.