Page 11 of 24
OG28.4 | Assisted Reproduction Techniques — SDL Guide (Part 2)
Outcomes, Risks, and Success Rates
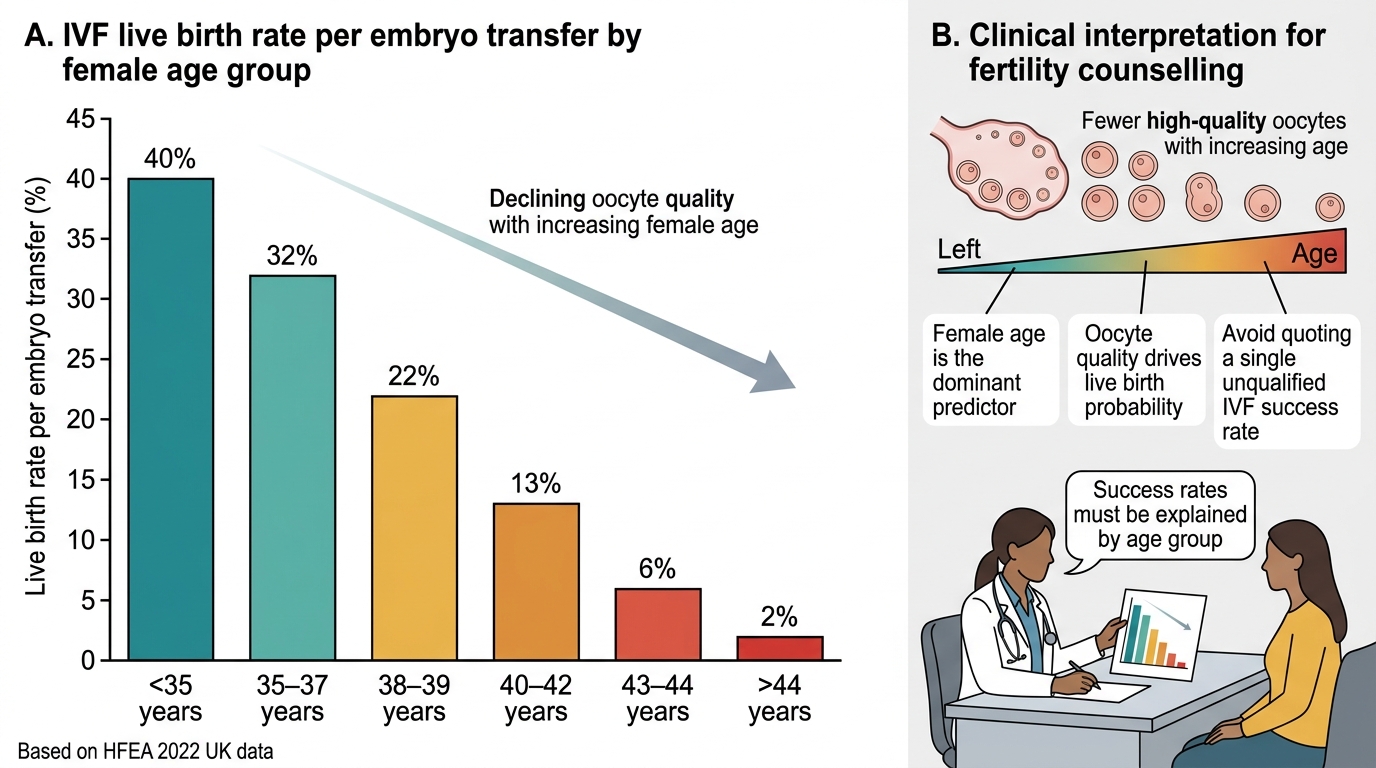
Realistic counselling about ART outcomes is one of the most important clinical skills in fertility medicine, because patients who are desperate and emotionally vulnerable consistently overestimate success rates and underestimate the physical, emotional, and financial demands of treatment. Evidence-based communication requires knowing the age-stratified data and being able to explain it clearly. The dominant message of the data is simple and must be delivered honestly: it is female age — specifically, oocyte quality — that determines the probability of a live birth from IVF, and this probability declines in a clinically significant, predictable, and unavoidable way as women age into their late thirties and forties. A patient who is told that IVF has a "40% success rate" without qualification may believe this applies to her at age 43; in reality, her probability of live birth with her own eggs may be 2–5%. Failing to communicate this clearly leads to multiple futile, expensive, and physically and emotionally exhausting cycles. The responsible clinician anchors the conversation in age-specific data from the outset.
IVF live birth rates decline steeply with female age, reflecting the decline in oocyte number and quality:
- Under 35 years: approximately 35–40% per embryo transfer
- 35–37 years: approximately 30–32% per transfer
- 38–39 years: approximately 20–22% per transfer
- 40–42 years: approximately 12–15% per transfer
- 43–44 years: approximately 5–7% per transfer
- Over 44 years: approximately 1–3% per transfer (with own eggs)
These figures are per-transfer; cumulative rates over multiple cycles are higher. With donor oocytes, success rates return to approximately 35–45% regardless of the recipient's age, because it is the egg donor's age that matters.
IUI success rates are approximately 10–15% per cycle (cumulative ~50–60% over 6 cycles in ideal candidates — young woman, patent tubes, mild male factor).
Risks of ART:
- OHSS: mild OHSS is common (~20–30% in gonadotrophin cycles); moderate OHSS in ~3–6%; severe OHSS in ~0.5–1%. Largely preventable with GnRH antagonist protocols and agonist trigger in high-risk patients.
- Multiple pregnancy: the most significant complication of IVF when multiple embryos are transferred. Twin pregnancy rates of ~15–20% increase risks of preterm delivery, gestational hypertension, operative delivery, and neonatal morbidity. Elective single embryo transfer (eSET) has reduced multiple rates in centres that adopt it.
- Ectopic pregnancy: risk ~2–5% with IVF (higher than spontaneous conception background); attributable to the presence of tubal disease in many ART candidates, not the technique itself.
- Congenital abnormalities: a small but consistently reported increase in the risk of certain birth defects (Beckwith-Wiedemann syndrome with imprinting defects; increased rates of hypospadias with ICSI). The absolute excess risk is small and must be contextualised against the significant risks of untreated infertility and advanced maternal age.
- Emotional burden: IVF failure is a significant psychological event; multiple cycles compound anxiety, depression, and relationship strain. Psychological support should be offered proactively.
IVF Live Birth Rates by Female Age
SELF-CHECK
A 44-year-old woman with diminished ovarian reserve (AMH 0.05 ng/mL, AFC 2) and 4 years of secondary infertility wishes to pursue IVF. After counselling, she remains committed to trying. What is the single most effective intervention to maximise her chance of a live birth through ART?
A. Increase the gonadotrophin dose to retrieve as many eggs as possible from her own ovaries
B. Use ICSI instead of conventional IVF to maximise fertilisation of any eggs retrieved
C. Proceed with donor oocyte IVF rather than own-egg IVF
D. Attempt IUI first with multiple cycles before IVF
Reveal Answer
Answer: C. Proceed with donor oocyte IVF rather than own-egg IVF
At 44 with severely diminished ovarian reserve, own-egg IVF carries a live birth rate of approximately 1–3% per cycle — the limiting factor is oocyte quality (aneuploidy rate >90% at this age), not quantity. Increasing the gonadotrophin dose will not improve oocyte quality. ICSI improves fertilisation but cannot correct aneuploid oocytes. IUI is futile at this age with poor reserve. Donor oocyte IVF — using eggs from a young donor — restores live birth rates to approximately 35–45% per transfer regardless of recipient age, because it is the donor's (younger) eggs that determine outcome. This is the single most effective change.
Regulation, Ethics, and Clinical Decision-Making
The practice of ART in India is governed by a specific statutory framework that final-year students must understand, both as a legal obligation and as a framework for ethical practice. This is an area where Indian law differs significantly from many Western jurisdictions, and applying foreign frameworks is inappropriate.
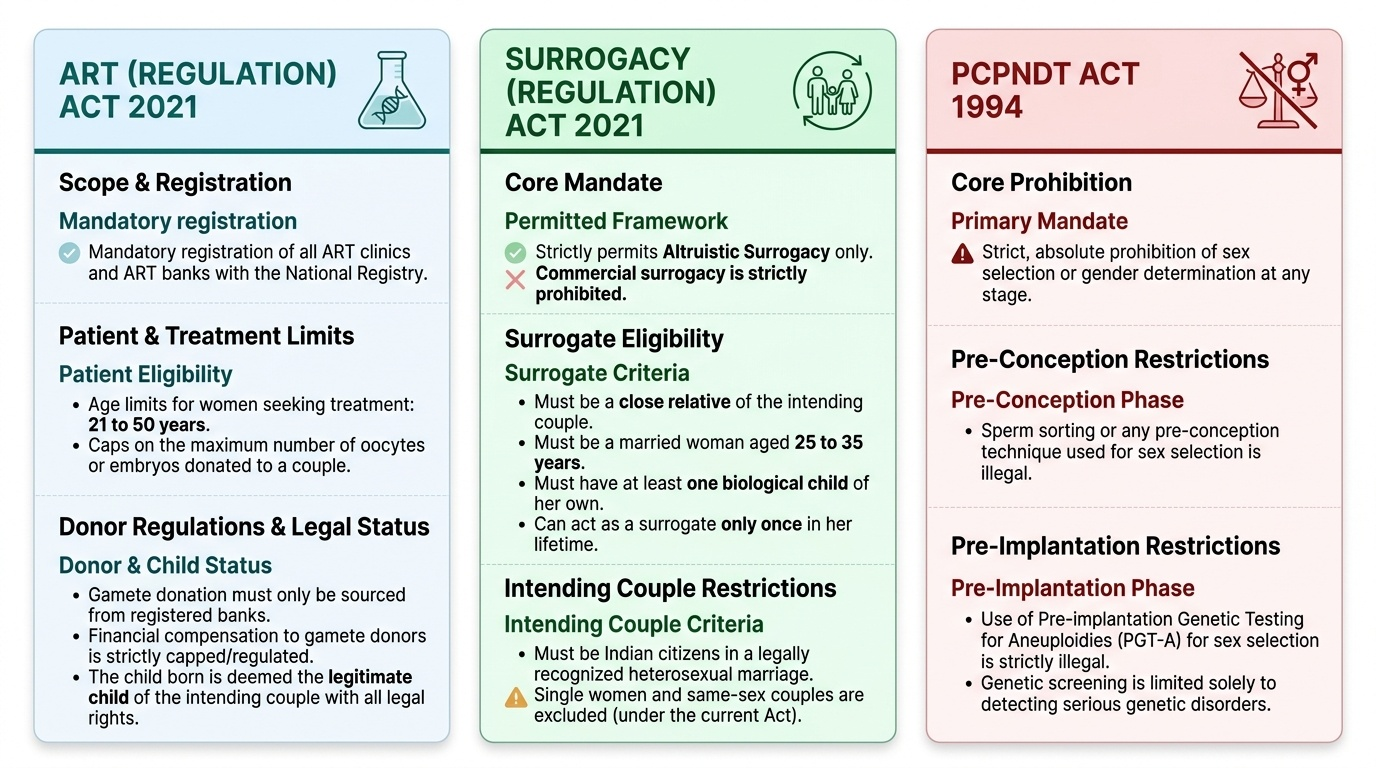
The Assisted Reproductive Technology (Regulation) Act 2021 (ART Act 2021) regulates ART clinics and ART banks in India. Key provisions: all ART clinics must be registered with the National Registry; the age limit for women seeking ART is 21–50 years; maximum number of oocytes or embryos that may be donated to a couple from one donor is limited; gamete donation must be from a registered bank; financial compensation for gamete donors is permitted within defined limits; the genetic parents of a child born through ART have all legal rights and responsibilities; a child born through ART shall be deemed to be the legitimate child of the couple.
The Surrogacy (Regulation) Act 2021 restricts surrogacy to altruistic surrogacy only — commercial surrogacy is prohibited. The surrogate must be a close relative of the intending couple; she must be a married woman aged 25–35 years who has at least one child of her own; she may act as surrogate only once in her lifetime. The intending couple must be Indian citizens in a heterosexual marriage; single women and same-sex couples cannot use surrogacy (under the current Act).
The PCPNDT Act 1994 (Pre-Conception and Pre-Natal Diagnostic Techniques) strictly prohibits sex selection at any stage including pre-conception (sperm sorting) and preimplantation (PGT-A used for sex selection). PGT-A for sex selection is illegal in India — PGT may only be used for medical indications (aneuploidy detection, monogenic disease). Any clinician or laboratory performing sex selection faces criminal prosecution.
When to stop ART: patients must be counselled about cumulative success rates and realistic limits. After 3–4 failed IVF cycles with own eggs in a poor responder or older woman, the probability of live birth with continued own-egg IVF is very low; transition to donor eggs, adoption, or acceptance of childlessness should be discussed compassionately. Continuing futile cycles is not ethically neutral — it causes physical, emotional, and financial harm.
Provided image
CLINICAL PEARL
The success rate of IVF is the age of the eggs, not the age of the uterus. A 45-year-old woman receiving donor eggs from a 28-year-old donor has approximately a 35–45% live birth rate per transfer — similar to a 28-year-old using her own eggs. This is one of the most counter-intuitive but important facts in reproductive medicine, and it has profound counselling implications: the woman's chronological age does not determine IVF outcome when donor oocytes are used. Also remember: ICSI does not improve IVF outcomes when sperm is normal — routine ICSI for all IVF cycles (a practice driven by commercial rather than clinical factors) provides no benefit over conventional insemination when semen parameters are normal or mildly abnormal.